
Abstract
Introduction:
To evaluate the flow characteristics produced by a manual and automated-pump irrigation system connected to a flexible ureteroscope.
Materials and Methods:
An in vitro analysis of a manual hand-pump infuser (HP) and the UROMAT Endoscopic Automatic System for Irrigation® (E.A.S.I.) pump was performed. Standard irrigation tubing was used to connect a three-way valve to a flexible ureteroscope, the irrigation system, and a digital manometer. Flow rate and irrigation pressure measurements were recorded over a 15-minute period using pressure settings of 150 and 200 mm Hg for both irrigation pump systems. Once the HP was inflated to the initial pressure, it was not reinflated over the course of the trial. Data were collected with the working channel unoccupied and with placement of a 200 μm (0.6F) holmium laser fiber, 1.7F nitinol stone retrieval basket, or 2.67F guidewire.
Results:
The difference in pressure measured at the site of inflow of irrigation to the ureteroscope was significantly greater using the HP compared to the E.A.S.I. pump at pressure settings of 150 mm Hg with and without the use of ureteroscopic instrumentation (p < 0.001), and at 200 mm Hg with instrumentation in the working channel (p < 0.01). There was no significant difference in the flow rate of irrigation through the open-channel ureteroscope over the course of 5 minutes between the two pump systems.
Conclusion:
The flow rates of irrigation produced by the HP and the E.A.S.I. pump are similar at pressures of 150 and 200 mm Hg irrespective of the occupancy of a ureteroscope's working channel during the first 5-minutes of irrigation. Irrigation pressure at the entry site of the ureteroscope is subject to significant variability with use of the HP compared to the E.A.S.I. pump irrigation system.
Introduction
C
Despite improvements in ureteroscopic technology, modern day ureteroscopes continue to be paired with antiquated hand-pump infuser (HP) devices. 4 The HP consists of a manually inflatable airbag that is coupled to the irrigant reservoir and is capable of increasing the flow rate beyond that achieved by gravity. Current HPs are equipped with a pressure gauge to indicate the degree of compression on the irrigant; however, the pressure and flow rate of irrigation delivered to the ureteroscope has not been verified, to the best of our knowledge. Alternatively, automated-pump systems have been developed that are capable of pressurizing irrigation according to the desired flow, yet the performance and safety of these devices during ureteroscopy are still under review. 5,6
In an effort to evaluate the flow and pressure properties of contemporary irrigation systems, we performed an in vitro fluid dynamic analysis of manual and automated-pump irrigation through a flexible ureteroscope with and without instrumentation in the working channel.
Materials and Methods
Irrigation device description
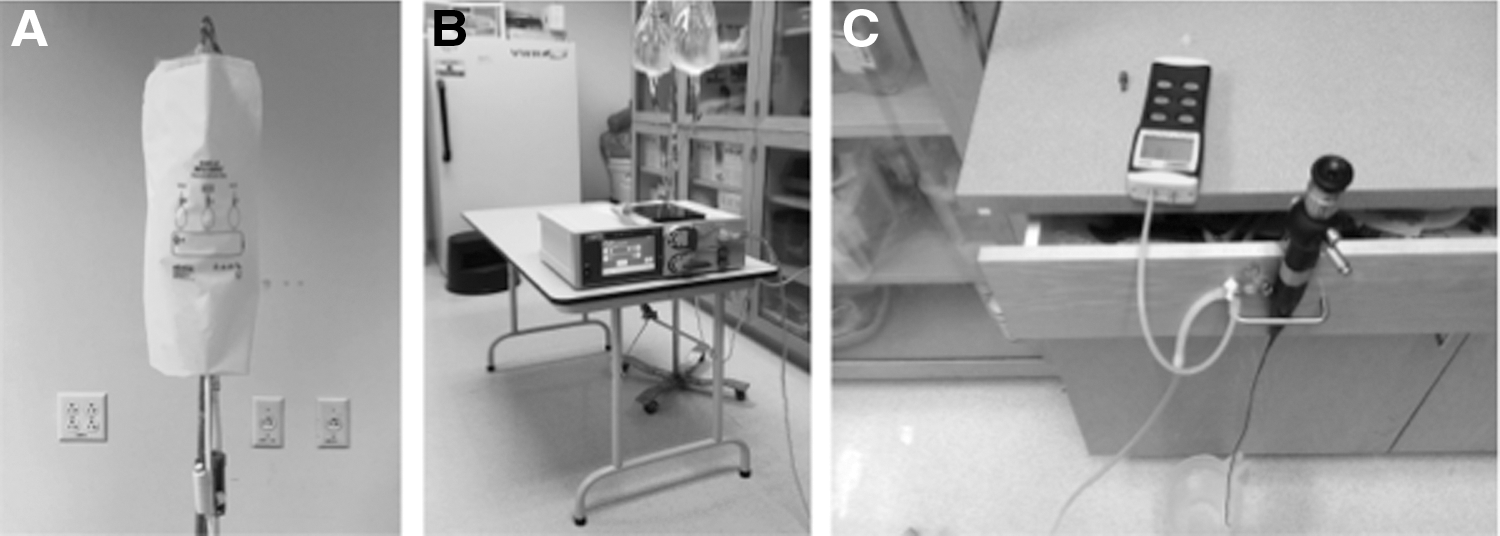
The HP (Ethox Infu-surg®; SunMed LLC., Grand Rapids, MI) consists of a reusable 1000 mL inflatable airbag with a sleeve that accommodates a 3 L bag of irrigant; the cost of the infuser and the 3 L bag is ∼$90 to $140. The HP is equipped with a pressure gauge (range 0–300 mm Hg), a three-way stopcock, and an oval bulb for manual inflation (Fig. 1A). It is connected to the ureteroscope via standard operating room tubing (3M™ Ranger™ Irrigation Fluid Warming Set; 3M Company, Maplewood, MN) at a cost of $40. The UROMAT Endoscopic Automatic System for Irrigation® (E.A.S.I.) pump (Karl Storz, Inc., Germany) is a pressure-controlled double roller pump that operates according to preset procedure-dependent settings (i.e., “hysteroscopy,” “resection,” etc.) or by manually entering the desired pressure or flow rate of irrigation. Up to two 3 L bags of irrigant can be connected to the E.A.S.I. pump, with the irrigation tubing placed into the designated roller apparatus (Fig. 1B). Once the E.A.S.I. pump is activated, pressure and flow rate measurements appear as a continuous real-time display on the pump's screen. The cost to purchase the E.A.S.I. pump is estimated at $16,000 to $20,000, while the cost for disposable tubing is $30 to $40. *
Irrigation flow rate and pressure measurements
A 7.5F flexible ureteroscope (Flex-X2; Karl Storz, Inc.) was connected to a 3 L bag of saline using standard irrigation tubing. The 3 L bag was placed into an HP and suspended from an intravenous pole at a height of 180 cm. A three-way valve was attached with one valve to the irrigant, one valve to a digital manometer (DM8252; General Tools and Instruments LLC., Secaucus, NJ), and the remaining valve to the ureteroscope (Fig. 1C). Two 15-minute trials were completed for each HP setting; flow and pressure measurements were performed at 150 and 200 mm Hg. Once the HP was inflated to the desired pressure, it was not reinflated during the 15-minute trial. Data were collected at set time intervals (1, 2, 5, 10, and 15 minutes); the working channel (3.6F) flow was studied when it was unoccupied and when it contained a 200 μm (0.6F) holmium laser fiber (Cook Medical, Inc., Bloomington, IN), 1.7F nitinol stone basket (Ngage; Cook Medical, Inc.), and 2.67F guidewire (Amplatz Super Stiff; Boston Scientific Co., Marlborough, MA). The digital manometer was tared before measuring the inflow pressure at the beginning of each trial.
For E.A.S.I. pump irrigation, a set of single-use proprietary tubing was connected to two 3 L bags of irrigant, the digital manometer, and the flexible ureteroscope using a three-way valve. Flow and pressure measurements were performed using the same protocol as that of the HP; however, the E.A.S.I. pump was set to manual-mode pressure settings of 150 and 200 mm Hg. Of note, the device's software limits the maximum pressure setting to 200 mm Hg.
Statistical analysis
The Wilxocon rank sum (Mann–Whitney) test was used to determine differences in the mean flow rates with the use of ureteroscopic instrumentation at 150 and 200 mm Hg for the HP compared to the E.A.S.I pump. The Mann–Whitney test was also used to determine the variability in the mean differences between the measured and set pressures between the HP and the E.A.S.I. pump. A cutoff of 5 minutes was used to limit the variablitiy in flow and pressure inherent with the use of a HP. All statistical models were two-sided using SAS® 9.4. Statistical significance was defined as p ≤ 0.05.
Results
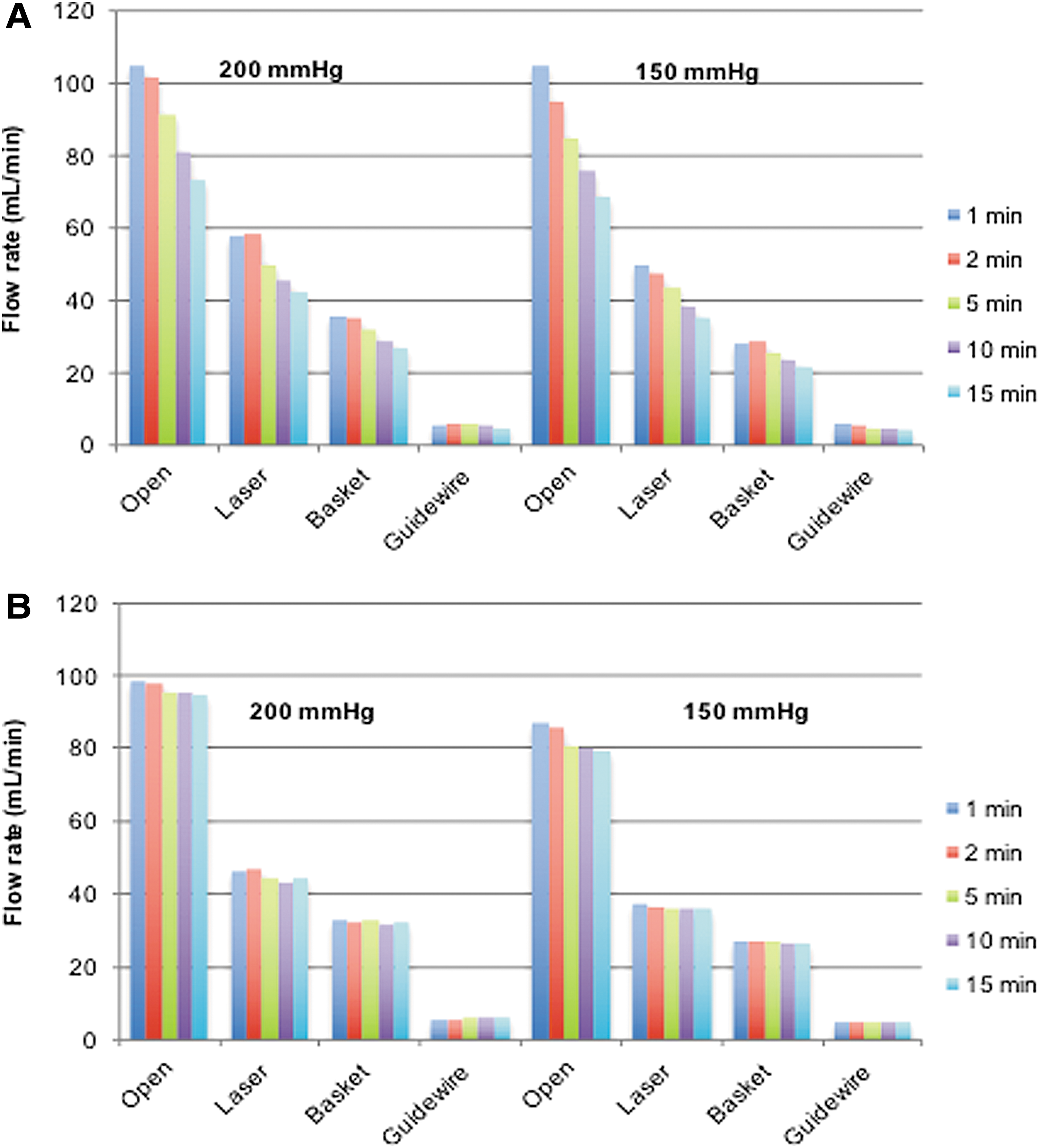
The flow rate of irrigation produced by the HP and the E.A.S.I. pump for each experimental condition are displayed in Figure 2. The flow rate declined steadily in each of the experimental conditions for the HP. For instance, the flow rates at 200 mm Hg when the working channel was unoccupied were 105 and 73.3 mL/min at 1 and 15 minutes, respectively. With the E.A.S.I. pump, the flow rates at 200 mm Hg when the working channel was unoccupied were 98.5 and 94.5 mL/min at 1 and 15 minutes, respectively.
Mean flow rate of irrigation produced by the hand-pump infuser
Comparisons of the flow rates of irrigation between the devices are presented in Table 1. The flow rate of both the HP and the E.A.S.I. pump were greatest when the working channel of the ureteroscope was unoccupied at 150 mm Hg (95.0 ± 10.0 mL/min vs 84.4 ± 3.3 mL/min, p = 0.400) and at 200 mm Hg (99.3 ± 7.1 mL/min vs 97.1 ± 1.7 mL/min, p = 0.700). The flow rate of both the HP and the E.A.S.I. pump were lowest when the working channel of the ureteroscope was occupied with a 2.67F guidewire at 150 mm Hg (5.5 ± 0.5 mL/min vs 4.9 ± 0.1 mL/min, p = 0.100) and at 200 mm Hg (5.8 ± 0.3 mL/min vs 5.8 ± 0.1 mL/min, p = 1.000).
E.A.S.I. = Endoscopic Automatic System for Irrigation®; HP = hand-pump infuser.
The irrigation pressure measurements for the HP and E.A.S.I. pump with an unoccupied working channel are shown in Figure 3. For the HP, the irrigant pressure reached the initial inflation pressure after ∼10 minutes at a setting of 150 mm Hg and after 5 minutes at a setting of 200 mm Hg. Using the E.A.S.I. pump, the irrigant pressure did not significantly change during the 15-minute trial at settings of 150 and 200 mm Hg.
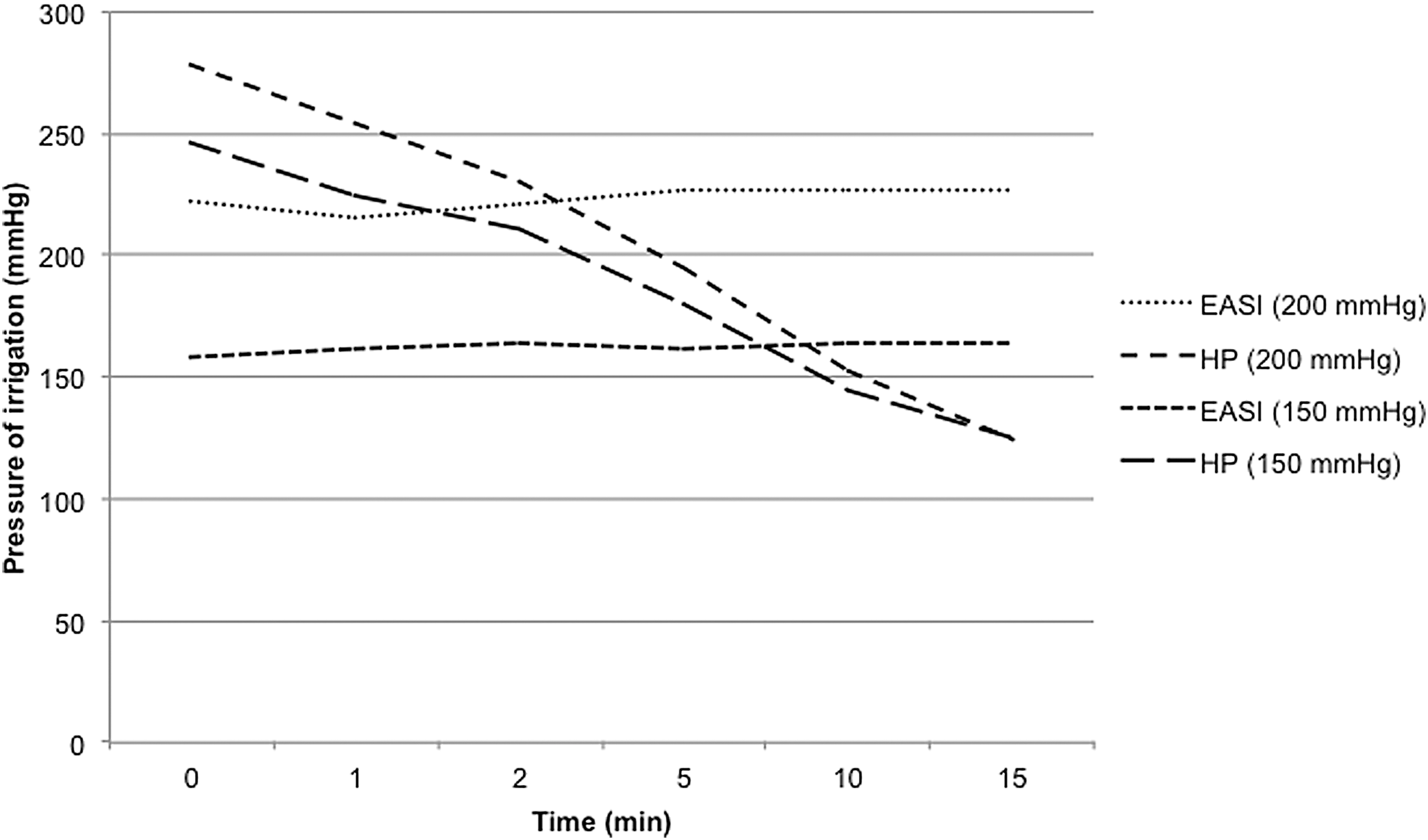
Mean irrigation pressure produced by the hand-pump infuser and the E.A.S.I pump at settings of 150 and 200 mm Hg with an open working channel.
At a pressure setting of 150 mm Hg, the difference in irrigant pressure at the site of entry into the ureteroscope was significantly greater using the HP compared to the E.A.S.I. pump when the working channel was open (p < 0.0001) and when it was occupied with instrumentation (p < 0.001) (Table 2). At a pressure setting of 200 mm Hg, the difference in irrigant pressure at the site of working port entry was significantly greater using the HP than the E.A.S.I. pump only when the working channel was occupied (p < 0.01); with an open working channel, the pressure difference was not significantly different (42.1 ± 29.3 mL/min vs 21.5 ± 9.1 mL/min, respectively, p = 0.22).
Discussion
Irrigation techniques used for flexible ureteroscopy have evolved. In 1971, Takagi et al. first described the clinical use of an actively deflectable flexible ureteroscope, in which intrinsic irrigation was provided by diuresing the patient with mannitol. 7 In 1974, Takayasu and Aso introduced the concept of a the ureteral “guide tube” to facilitate passage of a flexible ureteroscope and allow for the use of saline irrigation to improve visualization. 8 A decade later, Lyon et al. performed flexible ureteroscopy with irrigation connected to the ureteroscope's working channel and used the force of gravity to maintain the irrigant flow by placing a saline bag 30 cm above the level of the kidney. 9 By 1984, manual pump systems became standard operating procedure, which has continued unchanged over the ensuing 33 years.
Much of the recent developments in ureteroscopy have focused on improvements to ureteroscope design, 1,10,11 digital imaging systems, and ureteroscopic instrumentation. 12,13 The objective of many of these developments is procedural optimization, for which visualization is key. The quality of visualization is determined by the combination of superior optics and a clear operative field; the latter is very much dependent on irrigant flow. Okhunov and colleagues demonstrated that a superior flow during ureteroscopy also leads to superior surgical performance 14 ; however, studies exploring differences in outcomes with the use of various irrigation systems have been limited. 5,6,15 –18
Our results corroborate prior findings of a marked loss of flow as the diameter of instrumentation increased. 19 Importantly, the relationship of irrigation pressure and flow rate relates to a principle in physics derived from Ohm's law (I = V/R); that is, the flow rate is proportional to the irrigation pressure divided by the resistance. In our study, the irrigation pump pressure serves as the source of potential energy that creates flow. Since the diameter of objects placed in the ureteroscope's working channel is constant, flow is subject to a constant resistance. Therefore, our results (Figs. 1 and 2) reflect the natural physical laws that govern fluid dynamic properties of endoscopic irrigation systems.
In our study, the HP experienced an early rapid decline in irrigation flow rate regardless of working channel occupancy, which manifests clinically as reduced visualization and the need for a circulating nurse to frequently reinflate the HP to maintain pressure in the device and optimize irrigant flow. Fatigue has been described as a limiting factor for HP systems. 18 Indeed, a study by Proietti and colleagues highlighted a disadvantage to the use of manually operated irrigation systems. 5 The authors used an in vitro kidney model to study the impact of varying user strength on the pressure generated by commercially available hand- and foot-operated irrigation pumps. They found that the strength and experience of the assistant operating a manual irrigation device significantly influenced the space-occupying pressure during ureteroscopy. Alternative manual irrigation systems (e.g., the foot-pump) have been studied during ureteroscopy, yet they still require HP irrigation pressure to be maintained by auxiliary personnel, and consequentially, may result in high renal pelvic pressure (RPP). 15 Lechevallier et al. reported that the use of the ENDO FMS (Fluid Management System®; Future Medical Systems USA, Glen Burnie, MD), an automated irrigation system, reduced mean operative time by 32% when using a rigid ureteroscope and by 53% when using a flexible ureteroscope. 6 This device was a multipurpose tool not specifically designed for urologic procedures and unfortunately is no longer commercially available.
This study identified a marked underestimation of the pressure of irrigation delivered to the flexible ureteroscope compared to that inferred from the pressure gauge on the HP itself. Before the initiation of flow (i.e., t = 0 minutes), the discrepancy in irrigation pressure with use of the HP was nearly 10 times that of the E.A.S.I. pump at a setting of 150 mm Hg, and 4 times that of the E.A.S.I. pump at a setting of 200 mm Hg. Furthermore, the discrepancy in irrigation pressure was significantly greater with instrumentation in the working channel when using the HP (32–79 mm Hg) compared to the E.A.S.I. pump (8–25 mm Hg). Although higher irrigation pressure improves flow and may enhance visualization, a higher irrigation pressure can also give rise to increased RPP, resulting in venous, lymphatic, and/or sinus backflow, and the attendant risk of postoperative fever and urosepsis. 20,21
A solution with respect to preventing high RPP is the use of the ureteral access sheath, which has been found to significantly reduce intrapelvic pressures during ureteroscopy when using a manual pump irrigation system. 22 In this regard, the work of Deng et al. is of note as they developed a ureteral access sheath with the ability to monitor intrarenal pressures during ureteroscopy. In their experience with 90 patients, they were able to maintain RPP under 20 mm Hg with favorable optics, minimal complications, and a high stone-free rate at day 1 (90%) and day 30 (95.6%). 10
At this time, a pressure sensitive device on the tip of the ureteroscope capable of transmitting pressures wirelessly to an automated intelligent pump, which could then immediately respond to RPP approaching 30 mm Hg by downregulating the irrigation pressure, would be most beneficial. The development of an intelligent automated pump would greatly decrease the workload in the operating room while making ureteroscopic procedures safer by protecting both the renal pelvis and the calyces from excessive intraoperative pressures.
There are limitations inherent in modeling and understanding the flow characteristics of HP irrigation. Specifically, irrigation flow and pressure in our model was created with a one-time inflation of the HP device, whereas the clinical use of a HP requires frequent reinflation to maintain the desired flow and visualization. The decision for a single inflation of the HP device per trial was intended to standardize the experiment, as the time interval to maintain the pressure of the HP varies greatly in clinical practice. Furthermore, elevated irrigation pressures likely recur beyond the initial 5 minutes of ureteroscopy each time the HP is reinflated. Our decision to limit the highest HP pressure setting to 200 mm Hg was due to the E.A.S.I. pump's software restriction of a maximum manual irrigation pressure setting of 200 mm Hg; however, the HP is capable of a compression pressure in excess of 300 mm Hg. Thus, our in vitro study does not replicate the exact operating room conditions. In addition, one could argue that an artificial kidney model would provide an insightful in vitro study of endoscopic irrigation systems; however, we selected an experimental method that could be easily replicated and is not subject to model variation. Moreover, although we found significant differences in the line pressure between the two pump devices during the first 5 minutes of irrigation, significant differences in the corresponding flow rates of irrigation may have been measured with a powered study. Another limitation was the absence of any pressure measuring device in the renal pelvis. This would have been of interest as one could then have correlated the pressure of inflow with the resulting intrapelvic pressure. However, our experiment studied antegrade flow through the ureteroscope produced by manual and automated irrigation systems. Lastly, we used a ureteroscope with a working channel of 3.6F, which is also used in single-channel flexible ureteroscopes manufactured by Olympus, Karl Storz, Richard Wolf, and Boston Scientific. 23,24 Therefore, the unreliability of the HP system and its rapid decline in flow, regardless of the state of the working channel, can be extrapolated to the clinical use of other contemporary single working channel flexible ureteroscopes.
Conclusion
The flow rate of irrigation through a flexible ureteroscope via the HP and the E.A.S.I. pump systems is similar irrespective of the working channel occupancy at pressure settings of 150 and 200 mm Hg during the first 5 minutes of irrigation. However, after this brief time interval, HP flow falls precipitously necessitating attention to the device to maintain optimal pressure. In addition, irrigant pressure at the level of the ureteroscopic inflow port is subject to significant variability when utilizing the HP compared to the E.A.S.I. pump irrigation system.
Footnotes
Acknowledgment
Experimental design and physics analysis: George Coutrakon PhD.
Author Disclosure Statement
No competing financial interests exist.