
Abstract
Purpose:
The holmium YAG (Ho:YAG) laser penetration depth (PD) of 0.4 mm has been widely described. Nonetheless, in physics, this concept refers to the tissue thickness at which 90% of the energy has been absorbed and not to the incision depth (ID) that the laser can achieve in tissue. The aim of this study is to evaluate the ablation efficiency of Ho:YAG laser on soft tissue.
Materials and Methods:
With an automated robotic arm, systematic fissures were performed on flat veal kidney specimens. Broad setting spectrums from 2.5 to 80 W, short and long pulse, were tested with 272 and 365 μm laser fibers. Experiments were repeated three times. Two pathologists in a blinded manner measured the width, depth, and coagulation area with electronic microscopy.
Results:
The overall mean ID was 2 mm (0.25–4.39) and the mean width was 1 mm (0.3–3.1). The mean coagulation thickness was 0.48 mm (0.25–1.73). The higher the frequency and energy, the deeper and wider was the incision p < 0.001. No differences were observed regarding the fiber diameter. The pulse length did not affect the ID, although the mean width was greater with short pulse p = 0.04. The outer mean coagulation was increased by increasing energy but not by increasing frequency p > 0.119.
Conclusions:
The overall mean ID was significantly higher than the theoretical 0.4 mm PD described for Ho:YAG laser. The energy, frequency, and pulse length had individual effects regarding ID, incision width, and coagulation. The ID should be specified in accordance with the laser's power output and should not be confused with the physics of PD concept.
Introduction
T
Technological improvements have provided >120 W Ho:YAG machines with the possibility of adjusting a wide variety of parameters, including the pulsed energy in Joules (J), the pulsed frequency in Hertz (Hz), and the pulse lengths (short and long), 2,8,9 although only a few recent studies have mentions of pulse length recommending settings for soft tissue ablation. 10 –13
To date, only limited energy settings and fiber diameters have been tested in nonsystematic studies. 14,15 To our knowledge, no information has been published regarding the effect of Ho:YAG laser on soft tissue when using all the available settings and laser–fiber combinations. Also, there are no data regarding the individual effect of each of these parameters during ablation.
The purpose of this study was, therefore, to assess the ablation efficiency of the Ho:YAG laser in soft tissue at diverse pulse energies, frequencies, and pulse lengths and with different laser fibers.
Materials and Methods
Veal kidneys were chosen by their multilocular anatomy and the convenience to obtain flat and comparable samples of soft tissue.
To perform a systematic experiment, an automated robotic arm was employed to hold the firing fiber laser in contact with the specimen, moving transversely along the renal cortex in a straight axis at a continuous velocity of 3 mm/s, creating a 15-mm fissure on the kidney surface. Kidneys were submerged in 0.9% saline at room temperature to activate the laser (Fig. 1).
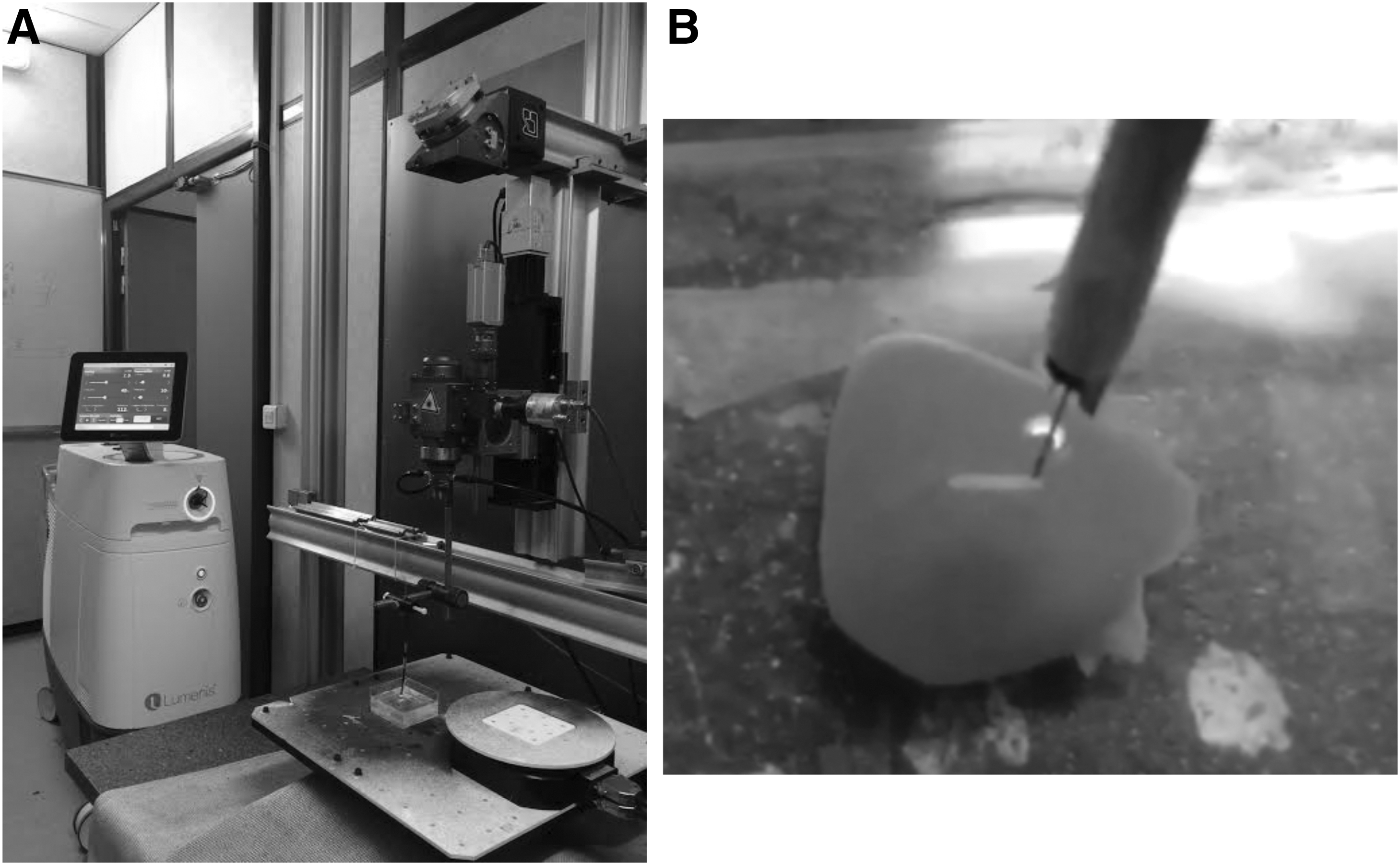
Experiment setting.
The Lumenis®-Pulse™ 120-W Ho:YAG laser (Lumenis Ltd., Israel) was used. The settings used covered a broad spectrum from 2.5 to 80 W and included high and low energy and frequency combinations and long and short pulses in accordance with the laser's capabilities (Table 1). Small 272-μm and large 365-μm laser fibers were used. For each test, the tips of the fibers were cleaved with ceramic scissors to avoid bias due to fiber degradation. All the settings and laser fibers were paired and two tests were performed per setting.
All the settings and laser fiber sizes were paired and independently tested.
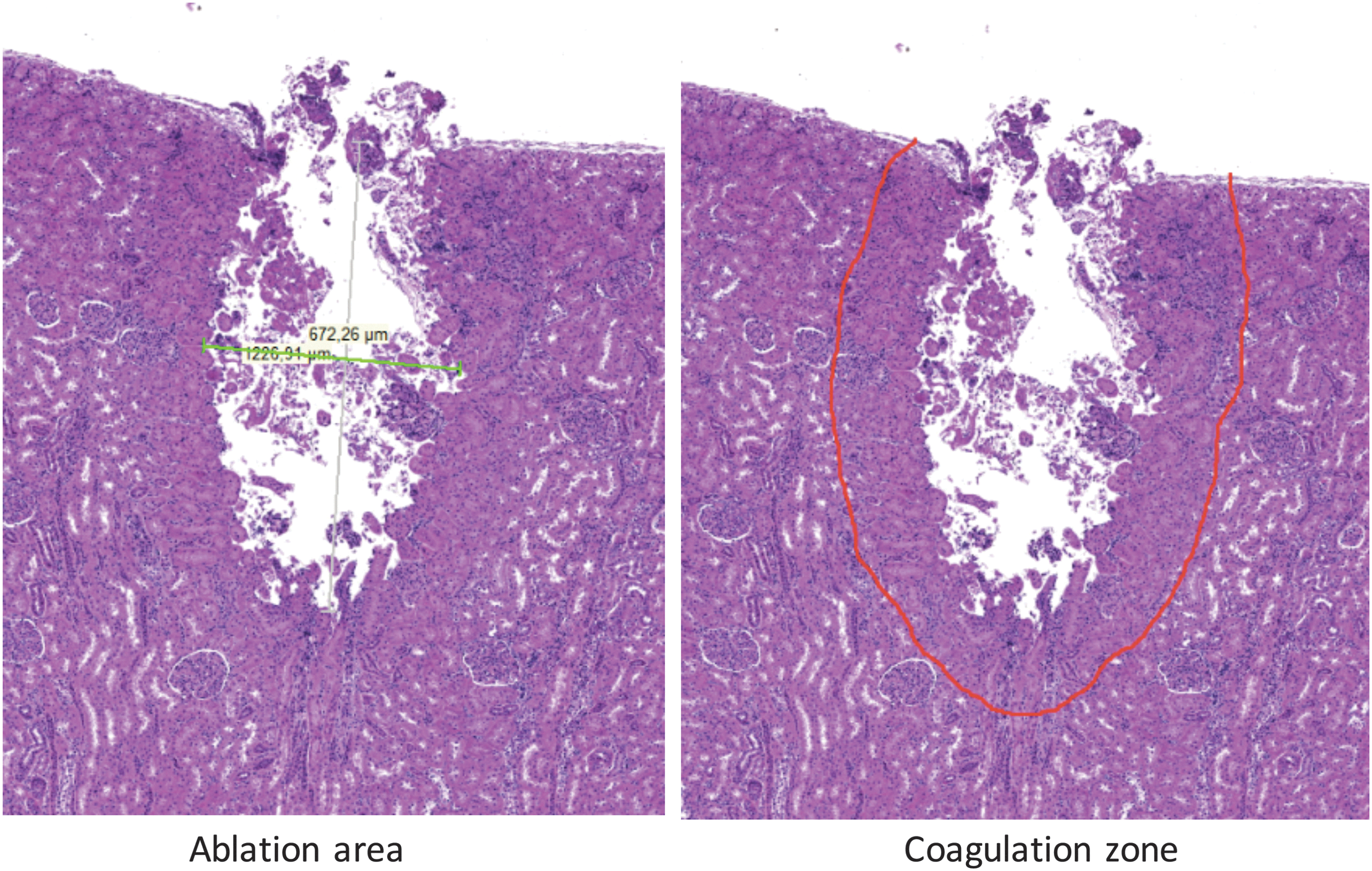
The specimens were collected, cataloged, and conserved in 0.4% formaldehyde. The fissures in each specimen were sliced into more than five 3-mm pieces, embedded in paraffin blocks, and stained with hematoxylin–eosin. Two pathologists measured separately, in a blinded manner, the width, depth, and area of laser penetration with electronic microscopy (Leica-DM4-M™, Leica®). In addition, the grade of thermocoagulation was measured in each specimen (Figs. 2 and 3).
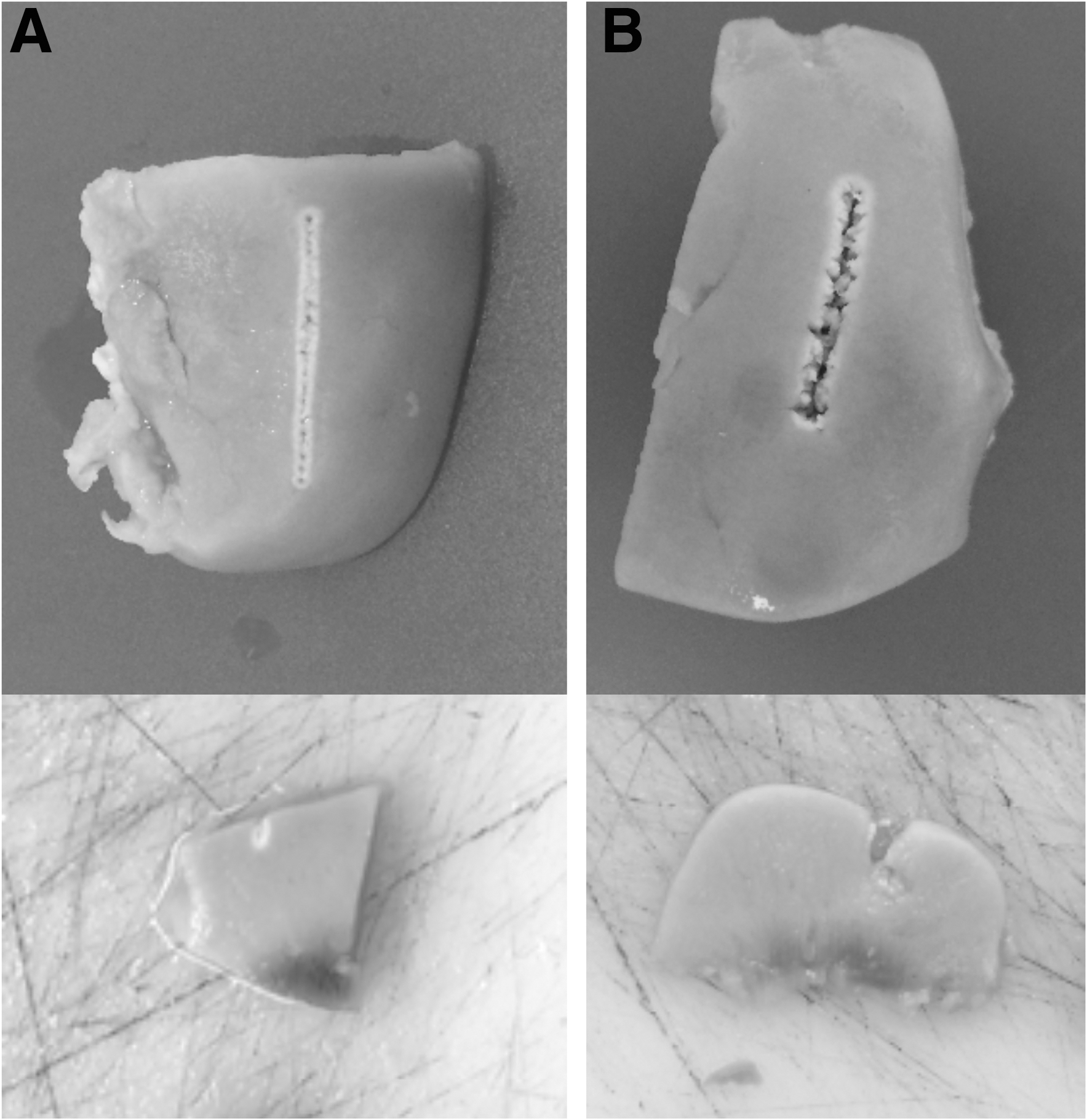
Specimen samples.
Specimen at pathological analysis.
Statistical analysis was performed using the SPSS software-21.0 (IBM-Corp. 2012, NY). t-Tests, analysis of variance, and Pearson's correlations were used to measure variations and linear correlations between variables.
Results
All the settings and laser fibers were combined, with performance of a total of 160 tests. The incisions had a predominantly triangular shape. The overall mean ID was 2 mm (0.25–4.39) and the mean width was 1 mm (0.3–3.1); the mean area was 1.6 mm2 (0.1–9.8). Lateral to the incision, a necrosis/coagulation zone was seen, with a mean thickness of 0.48 mm (0.25–1.73).
The higher the frequency and energy (and thus the power), the deeper and wider was the incision: p < 0.01 and p < 0.008, respectively.
Low-energy and low-frequency settings showed depth lengths of 0.75 mm (0.34–1.1) and 1.77 mm (1.07–3.18) for 0.5 J and 5 Hz and 1 J and 10 Hz, respectively, with mean width diameter of 0.82 mm (0.45–1.2) and 0.96 mm (0.37–1.19), respectively.
High-energy and high-frequency settings showed depth lengths of 2.5 mm (1.5–4.03) for 1.5 J and 30 Hz and 2.9 mm (1.21–4.39) for 2 J and 40 Hz and a mean width diameter of 1.3 mm (0.78–1.79) and 1.48 mm (1.05–1.6), respectively.
The pulse length did not affect the ID, although the mean width with the short pulse was greater than that with the long pulse (1.1 mm vs 0.9 mm, respectively, p = 0.04) (Figs. 4 and 5).
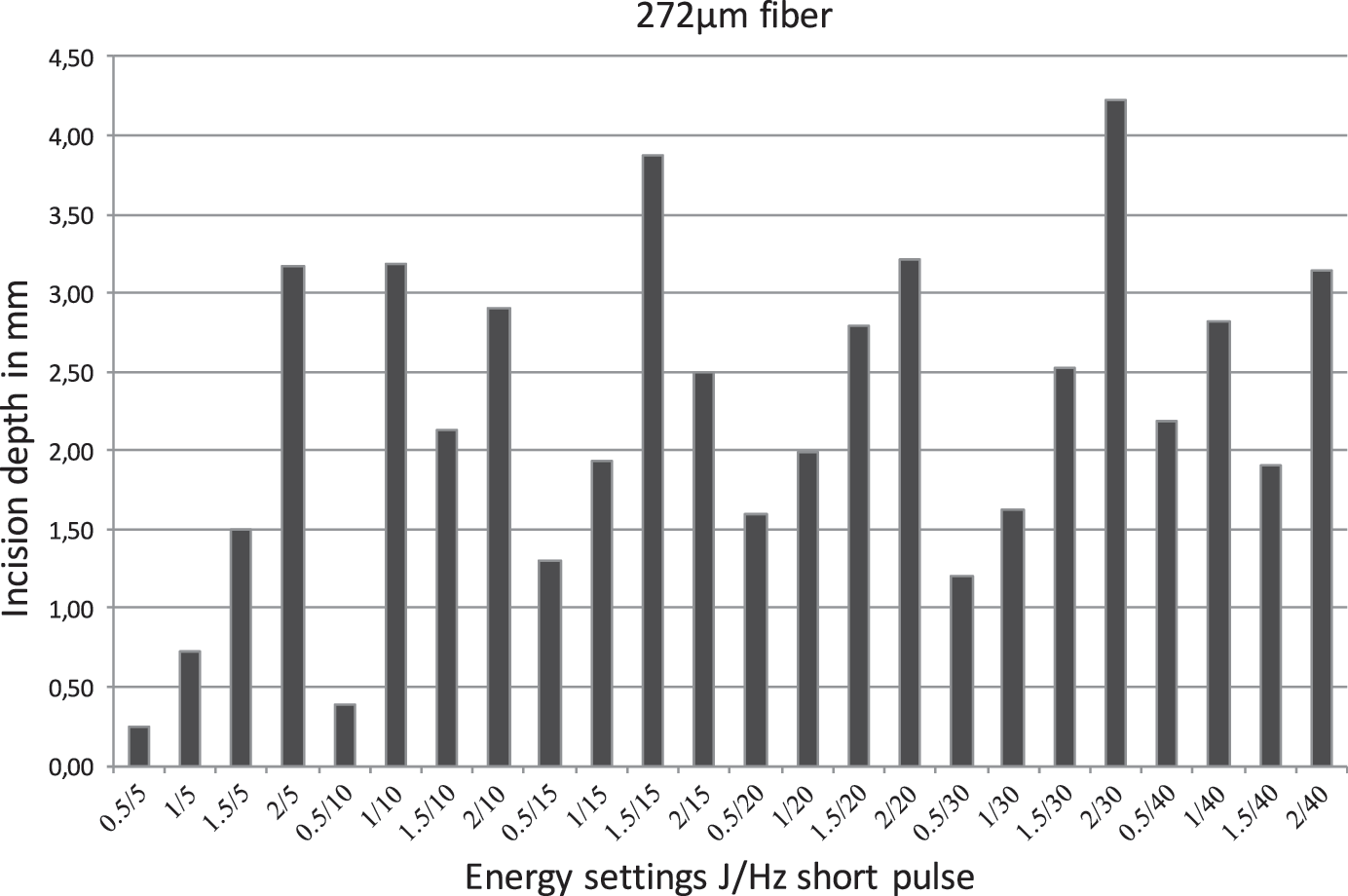
Incision depth combining different energy settings with a short pulse and a laser fiber size of 272 μm.
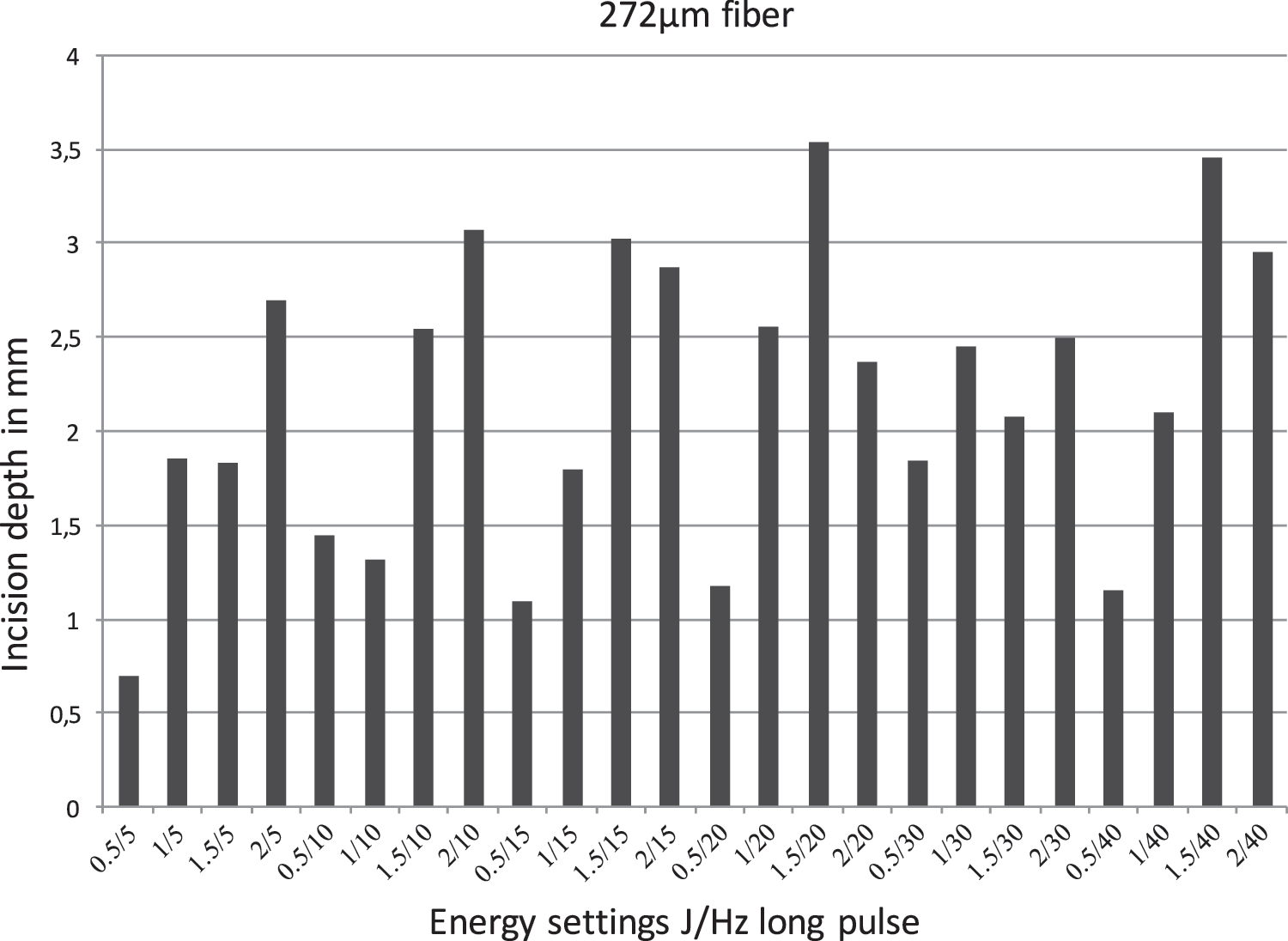
Incision depth combining different energy settings with a long pulse and a laser fiber size of 272 μm.
No significant differences in ID or width were observed in relation to fiber diameter.
The outer mean coagulation depth was 0.48 mm (0.25–1.73); this depth was increased by increasing energy (p = 0.01) but not by increasing frequency (p = 0.119), pulse length (p = 0.29), or fiber diameter (p = 0.67).
Discussion
The Ho:YAG laser has proven to be efficient for the treatment of diverse soft tissue pathologies such as prostate hyperplasia, upper tract urothelial carcinomas, and urinary strictures. 1,7 It is a pulsed laser with a wavelength of 2100 to 2140 nm that allows coagulation and vaporation–incision. Thus, it is a controlled energy source that is absorbed in water within 0.4 mm (defining the PD), making it a safe alternative among lasers in endourology. 2,7,13
Nonetheless, to our knowledge, there is no ex vivo or in vitro evaluations of the efficacy of the Ho:YAG laser in soft tissue that have considered all possible setting combinations with small and large fibers. The literature contains only one study on this topic: Johnson et al. 15 performed 10 incisions in 2 renal models by hand and in air (not under water as in endoscopy) in a contact manner. Their results showed that combining 0.5–1.5 J and 5–20 Hz (10 W) with a 400-μm fiber resulted in a mean ID of 0.4 mm (0.1–0.65 mm). In contrast to the work by Johnson et al., 15 in this study, the mean overall ID was shown to be significantly higher, at 2 mm (0.25–4.39). These differences may be attributable to the use of large and small fibers, the inclusion of long and short pulses in the experiment, the broader overall power spectrum (2.5–80 W), and the use of an automated system underwater that allows lower energy dispersion.
Regarding stone lithotripsy, it is known that increasing energy and using short pulses will provide greater ablative laser effects, whereas frequency affects only the timing, not the ablation itself. Also small fiber diameters can be used without compromising the ablation. 2,9 In this study, we observed similar effects as for stone lithotripsy as higher energy achieved wider and deeper tissue fissures and the fiber diameter did not modify the efficiency. In contrast, in soft tissue, higher frequency also produced wider and deeper tissue fissures. These findings are similar to those obtained in studies using neodymium:YAG, argon, and thulium:YAG lasers, which showed that the ablation volume increased with higher power output despite the theoretical PD of the lasers (1 cm, 1 mm, and 0.4 mm, respectively). 3,8,9,16 Furthermore, the PD of a laser is a theoretical physics concept that does not necessarily correlate with its effect on human tissue. This concept refers to the tissue thickness at which 90% of the energy has been absorbed and must not be confused with the direct laser effect on the tissue, which varies according to the power output. 8
A short pulse length generated wider incisions as short pulses work with rapid release of compressed energy making it more ablative than long pulses, which release energy over a longer period, with reduced intensity. 2 The wider incisions with the short pulse may result from the lateral diffusion of energy over an initially wide surface area. Subsequently, the width decreases as the energy is absorbed and the temperature reduces. 17 This also explains the predominantly triangular shapes of the incisions.
For treatment of upper urinary tract urothelial carcinoma (UTUC) and stenosis, a range of setting combinations have been described: 0.5–1.0 J and 5–10 Hz. 12,13 Recently some authors have included the pulse length in the setting combinations, recommending long pulse, low energy, and low frequency for coagulation and short pulse and higher energy and frequency for ablation. 10 This study showed that this range gives mean depth lengths from 0.75 to 1.77 mm for 0.5 J and 5 Hz and 1 J and 10 Hz, respectively, with a maximum depth in the latter case of 3.18 mm.
Some authors have proposed empirical settings of 1.5–2 J and 25–50 Hz for prostate enucleation. 18 For these settings, our study showed a mean depth length of 0.7 mm; for 0.5 J and 5 Hz, mean depth length was 0.39 mm and for 1 J and 10 Hz, mean depth length was 3.18 mm.
The continuity of the thermal effect created a coagulation zone underneath the incision. 9 Theoretically this could be considered as the “real” penetration of the laser (and not the ID itself) as it is the maximum reach of the laser. This also shows the capacity of the laser to decrease bleeding, better achieved with long pulse, low energy, and low frequency. 10 In this study, the coagulation zone increased with greater energy; nonetheless, it did not increase with greater frequency or in response to changes in the pulse length or fiber diameter. The shallow penetration of a low-energy setting may make vascular lesions less likely. Pulsed energy may be the key component in avoiding vascular lesions, as the pulse length did not appear to affect the coagulation layer.
Capillaries in the ureter are just below the urothelium at the lamina propria. The muscular layer starts 0.1 to 0.2 mm from the lumen and the first vascular structures are seen at 0.4 mm. The adventitia starts 0.6 to 0.7 mm from the lumen containing big periureteral vessels (Fig. 6). This shows how easily vascular structures can be reached even with low energy and long pulse.
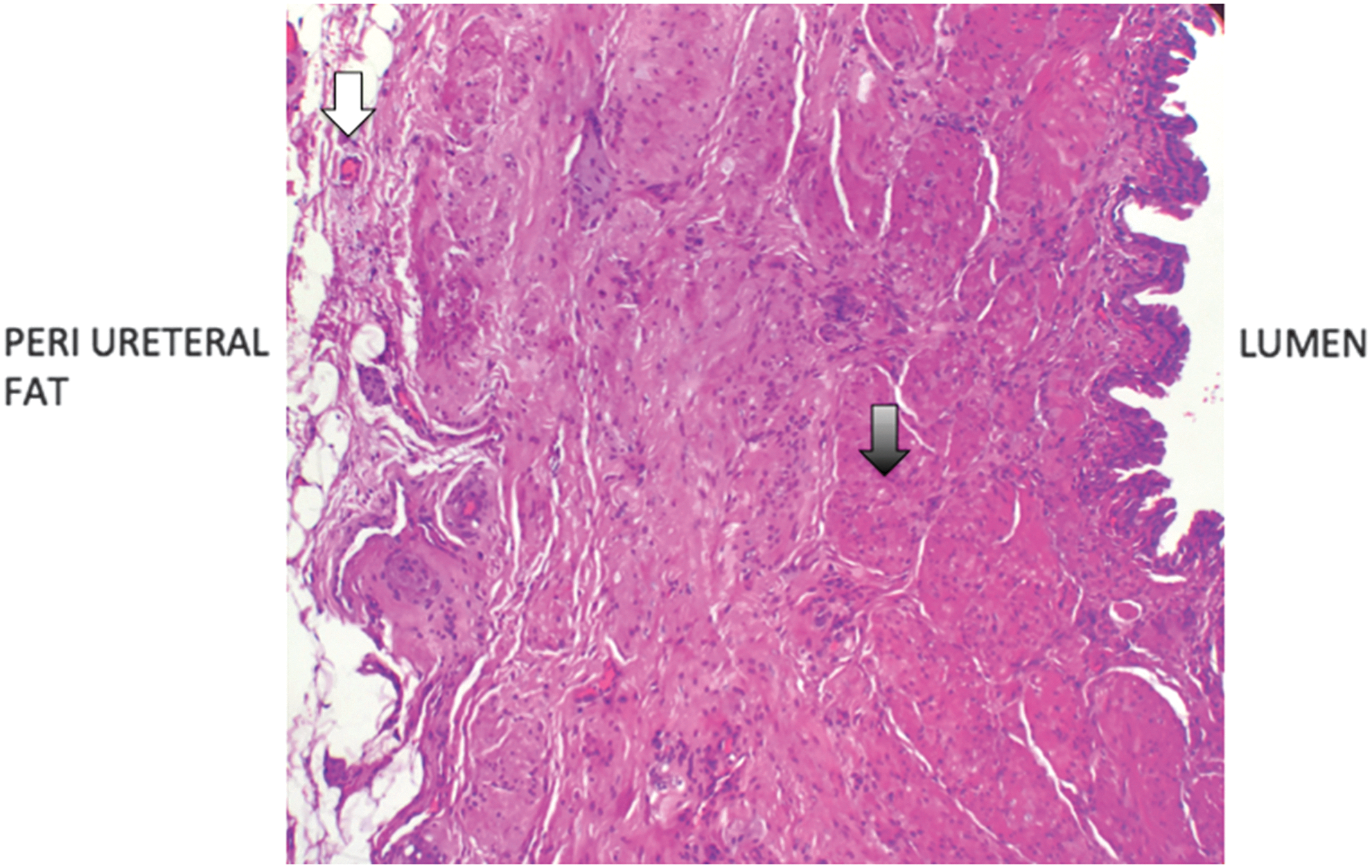
Ureteral histology slide. Capillaries are just below the urothelium at the lamina propria. The first vascular structures are seen at 0.4 mm from the lumen (black arrow) in the muscular layer. Larger periureteral vessels start to appear at 0.6 to 0.7 mm from the lumen (white arrow).
To our knowledge, this is the first systematic study to test all the possible Ho:YAG laser settings and fibers of different diameters. A clear understanding of laser effect on soft tissue offers a good basis for improving our surgical efficiency and safety. The concept of a 0.4-mm PD should be revised and the ID specified according to the setting used. Moreover, it should not be confused with the physics of PD concept: naming it the “incision depth” would be a good option to avoid confusion. The Ho:YAG laser has been shown to be a safe laser although the “shallow” PDs described in the literature should not be underestimated as it has been shown that the theoretical PD can be exceeded simply by increasing the power output of the laser. The broad range of penetrations in this experiment (0.25–4.39 mm) shows that the laser could easily become unsafe. Finally the real penetration definition may include the coagulation zone that shows the maximum reach of the laser.
For a clinical recommendation, a safe technique to treat upper urinary tract tumors and ureteral stenosis and ablate soft tissue consists in activating the laser before contact with the tissue and adopting a careful approach until the desired effect has been achieved, thereby avoiding deep unwanted incisions. If coagulation is necessary, it should be applied only in the desired area and with a noncontact mode. Use of 10 W (1 J and 10 Hz and short pulse) for the distal end of a papillary tumor may represent a good approach, although 2.5 W (0.5 J and 5 Hz and long pulse) may be more suitable in the base, creating narrow incisions. For ureteroscopy, the use of a small fiber will not decrease the efficiency and will maintain good deflection and irrigation. The same effect can be translated to prostate ablation, wherein the contact mode has been used for incisions and the noncontact mode for coagulation, avoiding deep incisions. 18
The limitations of this study include the in vitro scenario and the use of only renal cortex. Also fibers >500 μm were not used. Finally, the perfusion of live tissue might have an effect on heat absorption and may vary the effects when extrapolating the results.
Conclusion
The overall mean ID of a wide variety of Ho:YAG laser settings (2.5–80 W) was 2 mm, the mean width, 1 mm, and the outer mean coagulation depth, 0.48 mm. The higher the frequency and energy, the greater was the ID and the fissures width. The short pulse increased the incision's width but not the ID. Only energy affected the coagulation zone. The incisions were not affected by the fiber diameter. The ID was significantly higher than the theoretical 0.4-mm PD described in the literature. The ID should be specified in accordance with the laser's power output and should not be confused with the physics of PD concept.
Footnotes
Author Disclosure Statement
No competing financial interests exist.