
Abstract
Introduction:
Ureteral colic has a lifetime prevalence of 10%–15% and is one of the most common emergency urologic presentations. Current European Association of Urology recommends conservative management for “small” (<6 mm) ureteral stones if active removal is not indicated. It is important to understand the natural history of ureteral stone disease to help counsel patients with regard to their likelihood of stone passage and anticipated time frame with which they could be safely observed. We aimed to conduct a systematic review to better establish the natural history of stone expulsion.
Methodology:
Literature search was performed using Cochrane and PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines. Outcome measures were patient and stone demographics, expulsion rates, expulsion times, and side effect of the medication. A cumulative analysis, with subgroup analysis, was performed on stone location and size. The results were depicted as percentages and an intention-to-treat basis was used.
Results:
The literature search identified 70 studies and a total of 6642 patients, with a median age of 46 and range of 18–74 years. Overall, 64% of patients successfully passed their stones spontaneously. About 49% of upper ureteral stones, 58% of midureteral stones, and 68% of distal ureteral stones passed spontaneously. Almost 75% of stones <5 mm and 62% of stones ≥5 mm passed spontaneously. The average time to stone expulsion was about 17 days (range 6–29 days). Nearly 5% of participants required rehospitalization due to a deterioration of their condition and only about 1% of patients experienced side effects from analgesia provided.
Conclusion:
We believe this current review is the largest study for the evaluation of natural history of ureteral stones. The evidence suggests that ureteral stones will pass without intervention in 64% of patients, however, this varies from nearly 50%–75% depending on the size and location, in the span of 1–4 weeks.
Introduction
U
Ureteral stone has a lifetime prevalence of 10%–15% and is one of the most common urologic presentations in the emergency department. 3,4 Patients experience severe flank pain radiating to the groin because of sudden obstruction of the ureter, with associated risks of hydronephrosis, renal damage, infection of the urinary tract, and severe sepsis. 5
Ureteral stones can be managed by different modalities; expectant management with spontaneous passage of the stone, with or without medical expulsive therapy as an adjuvant. 6 Those that fail to pass stones spontaneously will require more invasive options.
In the absence of infection, severe obstruction, renal impairment, and uncontrollable pain, expectant management of spontaneous stone passage is preferred, as long as the passage is likely in a reasonable time frame. 7,8 There is no clear consensus of recommendations for expectant management of ureteral stones either by the American Urological Association (AUA) or by the European Association of Urology (EAU), mainly due to studies with insufficient supporting data. However, current AUA guideline recommends trial of spontaneous passage for ≤10 mm stone 9 and EAU recommends the same management for “small” ureteral stones referring to ≤6 mm stones, if active removal is not indicated. 10
It is extremely important to understand the natural history of ureteral stone disease especially to recognize the cohort of patients and their stone characteristics, who would expel the stone spontaneously and also to understand the time frame they can be safely observed with least undesirable complications.
However, current literature lacks high-level evidence on spontaneous passage rates. Therefore, we aimed to conduct a systematic review of all randomized trials to better establish an evidence-based natural history of stone expulsion, which can aid management of ureteral stones. In addition, we will look at all studies that specifically researched the natural history of stone expulsion.
Methodology
Search strategy
The systematic review of the literature was performed using Cochrane and PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines.
11,12
The search strategy included the following databases: The U.S. National Library of Medicine's life science database (MEDLINE) (1980–August 2017), EMBASE (1980–August 2017), Cochrane Central Register of Controlled Trials—CENTRAL (in The Cochrane Library—2017), CINAHL (1980–August 2017),
Search terms used in conjunction with each other included: “urolithiasis,” “urinary calculi,” “renal calculi,” “ureteric calculi,” “urinary stones,” and “randomized controlled trial.”
Medical Subject Headings (MeSH) phrases included: - ((“Calculi”[Mesh] OR “Urinary Calculi”[Mesh] OR “Kidney Calculi”[Mesh]) AND “Randomized Controlled Trial” [Publication Type]) - ((“Adrenergic Alpha-Antagonists”[Mesh]) AND “Urinary Calculi”[Mesh]) AND “Randomized Controlled Trial” [Publication Type])) - ((“Calcium Channel Blockers”[Mesh]) AND “Urinary Calculi”[Mesh]) AND “Randomized Controlled Trial” [Publication Type]))
Study selection
All languages were included if data were extractable, also references of searched articles were evaluated for further studies for potential inclusion. Authors were contacted wherever the data were not available or not clear, to be able to adequately assess inclusion of their study. If data were not extractable, provided, or clarified, the study was excluded.
Four reviewers (S.Y., T.A., O.A, and B.S.) identified studies that appeared to fit the inclusion criteria for full review. Four reviewers (S.Y., T.A., B.S., and O.A.) independently selected studies for inclusion. Disagreement between the authors in study inclusion was resolved by consensus.
Data extraction
Data of each included study were independently extracted initially by three authors (S.Y., T.A., and P.J.) after which a senior author (O.A.) extracted the data independently and cross checked each data extraction to ensure quality assurance of data across the board.
All studies comparing a treatment modality to a placebo were included. Published trials on adult patients of placebo arms of stone expulsions and all studies looking at the natural history of stone expulsions were included. We excluded studies on children or stone management studies that did not include a nontreatment arm, that is, trials of extracorporeal shockwave lithotripsy, ureteroscopy, or percutaneous nephrolithotomy in isolation, with no placebo nontreatment group. We extracted data of the placebo arms of trials, where no medical expulsive therapy or surgical treatment has been carried out, to be able to determine the natural course of stone expulsion and cumulatively analyzed these with that of studies reporting the natural history.
The following variables were extracted from each study: patient and stone demographics, expulsion rates, expulsion times, and side effect of the medication. The data of each study were grouped into a meta-analysis, in an intention-to-treat basis.
Statistical analysis and quality assessment
The data of the placebo arms of each trial were extracted to represent the natural history of stones. We divided each subcategory into an overall expulsion rate, stones in the upper, middle, or lower ureter, and stones <5 mm and >5 mm. The results were depicted as percentages and an intention-to-treat basis was used.
We included all studies looking at the natural history of stone expulsion rates as well as randomized control trials (RCTs) as these studies are more controlled and more reliable that no intervention was done for the placebo arm and the results are more likely to represent the true natural history of stone expulsion. An assessment of the methodologic quality of the RCT was conducted in line with the Cochrane handbook. 12
Results
Literature search
The literature search identified 876 studies, of which 697 were excluded due to nonrelevance based on titles and 179 excluded due to nonrelevance based on the abstracts (Fig. 1). Full articles were evaluated in 91 studies, of which 22 studies were excluded due to not meeting inclusion criteria. The remaining 70 studies were included that reported on the spontaneous passage of ureteral stones without any medical or surgical intervention (Fig. 1). 8,13 –81
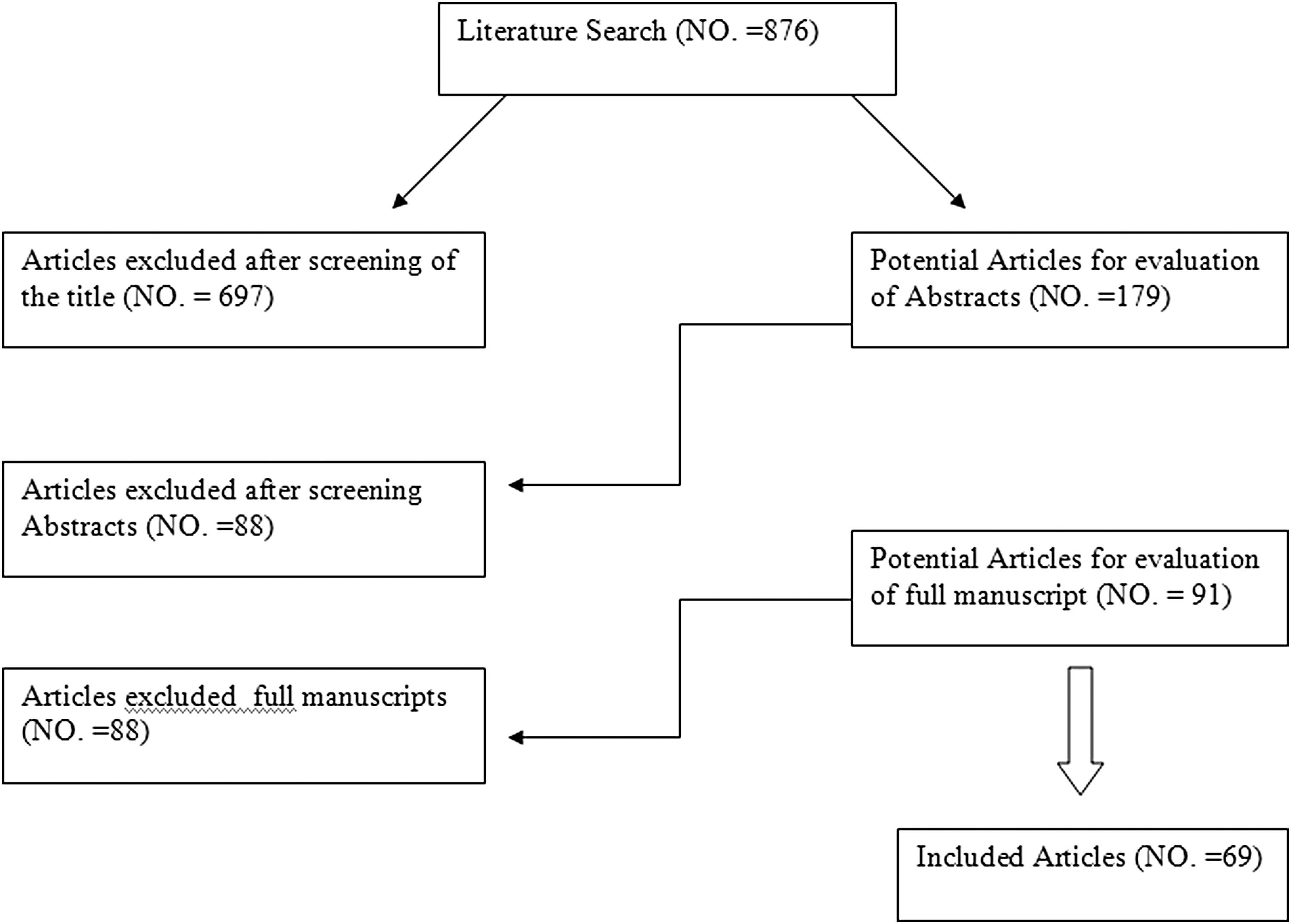
Flowchart for article selection process of the review.
Characteristics of the included studies
The trials span over three decades from 1994 with the latest in 2017. While the natural history articles spanned from 1977 to 2017. We were unable to obtain full articles before this date to analyze, therefore excluded. There were a total of 6642 patients conservatively treated. The age range was between 17 and 74 years. All the natural history studies looked at stone expulsion with no intervention. Table 1 depicts the patient and stone demographics.
F = female; IQR = interquartile range; M = male; n/a = not available; SD = standard deviation.
All the RCTs reported on the spontaneous stone passage rates with no intervention. Regarding stone location within the ureter, 15 studies reported on upper tract stones, 10 on middle ureteral stones, and 65 on distal ureteral stones. Nine studies reported on more than one location. 24,38,40,42,44,47,55 65,69 Sixteen studies reported on stones <5 mm, 29,33,34,39,40,44,46,48,55,69,75 –77,79 –81 while 19 reported on stones >5 mm. 22,24,29,30,33,35,39,40,44,48,55,57,60,69,75 –77,79,81 Twelve of the studies reported on stones in the distal ureter and >5 mm, 22,24,29,30,35,48,57,60,75 –77,81 while no other studies were found that data could be extracted for stones combining locality and stone size.
Cumulative analysis results
Stone passage
Overall, 64.4% of patients effectively passed their stones without any medical or surgical interventions (Table 2).
Dividing the stones in locality: 49.1% of upper ureteral stones, 58.1% of middle ureteral stones, and 68.1% of distal ureteral stones passed spontaneously (Table 2).
Groups based on size: 75.3% of stones <5 mm passed spontaneously irrespective of location as opposed to 61.6% of stones >5 mm that passed spontaneously (Table 2).
Requiring rehospitalization
Nearly 5% required rehospitalization due to worsening of their condition, that is, pain not controlled by analgesics or developed a sepsis (162/3035).
Side effects
Only 1% of patients experienced side effects from analgesia provided (31/2745). These included nausea and vomiting, being the most common, other side effects included headaches, dizziness, rhinitis, fatigue, hypotension, diarrhea, and heartburn.
Methodologic quality assessment
All the studies were reported as randomized controlled studies, ergo considered high-quality studies. Figure 2 depicts the summary of the quality assessment based on the reviewing author's judgment of risks of bias for each included study. Of the 63 trials, only 12 had no risk of bias to note. 17,30,32,33,37,54,55,62,65 –67,81
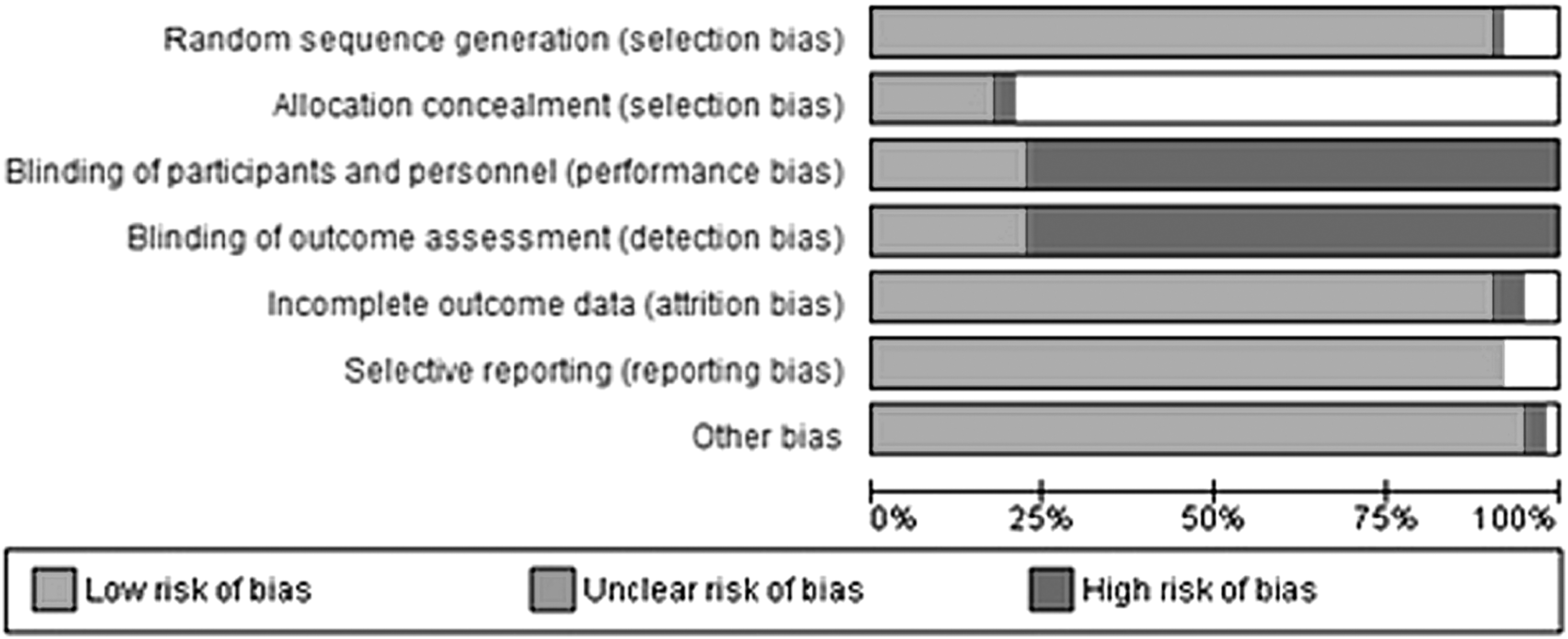
Risk of bias graph: review authors' judgments about each risk of bias item presented as percentages across all included studies.
One trial did not have appropriate randomization. 50 We found that the blinding was the main differential aspect of the quality assessment between the studies. Only 14 had adequate blinding. 13,17,22,23,30,33,37,53,55,62,65 –67,81 Furthermore, concealment was not mentioned in many of the trials with 50 not mentioning how they concealed their study, giving an unclear decision on concealment; 2 trials made no attempts at concealment, 49,71 while 11 trials had adequate concealment. 17,30,32,33,37,54,45,62,65,66,81 Three studies had incomplete outcomes reporting bias. 47,49,50 Two other studies had other risk of bias. 19,60
Regarding the natural history studies, these were of low evidence as they were all cohort retrospective or prospective studies, however, each study meticulously delineated its methodology protocol and did not have any evidence of selection or reporting bias, and no missing data.
Discussion
Although it is demonstrated in various studies that small ureteral stones pass spontaneously, 8 urologists are frequently challenged with the decision of whether to observe a stone in expectation of spontaneous passage or to intervene surgically. 82 Studies have also demonstrated that spontaneous passage of ureteral stone is size and location dependent. 66,71 The more the distal the stone is in the ureter, the greater is the probability of spontaneous passage. In addition, smaller stones are prone to pass quickly when compared with larger stones. 8
We investigated the outcome of ureteral stones in 6642 patients treated by expectant management. The incidence of spontaneous passage relating both stone size and location was determined from these collated studies. The rate of spontaneous passage for stones <5 mm was 75% compared with 62% for those >5 mm, irrespective of their position in the ureter at the time of presentation. While stones discovered in the distal third of the ureter had a spontaneous passage rate of 68%, compared with the middle third of 58%, and the proximal third of 49%, with a low complication rate.
Stones expulsion rates
Consideration of various factors is essential to determine the optimal treatment for patients with ureteral stone. Canadian Urological Association guidelines divide these factors broadly into four categories, namely (1) stone factors consisting of location, size, composition, and presence and duration of obstruction; (2) clinical factors consisting of symptom severity, patient's expectations, associated infection, obesity, coagulopathy, hypertension, and solitary kidney; (3) anatomic factors such as horseshoe kidney, ureteropelvic junction obstruction, and renal ectopia; and (4) technical factors of availability of equipment, expertise, and cost. The guideline also emphasizes the selection of any modality of treatment to be based on achieving maximal stone clearance with minimal morbidity to the patient. 7
Various studies have demonstrated spontaneous stone passage rate in relation to the stone size; Ueno et al. in 1977 showed spontaneous passage rates of 38% and 1.2% in stones <4 mm and >6 mm, 80 Hubner et al. in 1993 reported a cumulative analysis of the literature, which showed 57% spontaneous passage of stones <4 mm, 35% in those with 4–6 mm stones, and only 8% in those with stones >6 mm. 76 Coll and colleagues demonstrated a close relationship of stone size and spontaneous passage. They reported that stone sizes of 1, 4, 7, and 10 mm had spontaneous passage rate of 87%, 72%, 47%, and 27%, respectively. 75
The locations of stones also have been well recognized as an important factor in the spontaneous expulsion rate. In 1991, Morse and colleagues demonstrated a spontaneous stone passage rate of 71% from the distal, 46% from the middle, and 22% from the proximal ureter. 77 Hubner et al. showed spontaneous passage in 38% of stones located in the distal third of the ureter, compared with 15% in the middle third and 18% of stones in the proximal third. 66 In a retrospective radiologically followed study using unenhanced CT scan, Coll et al. reported spontaneous stone passage rate of 75% in distal ureter, 60% for middle ureteral stones, and 48% for stones in the proximal ureter. 75 Sfoungaristos and colleagues noted spontaneous passage of 50% distal ureteral stones, including stones in Vesico Ureteric Junction and 90% passage rate for middle ureteral stones. 69
All these studies highlighted how there are discrepancies in the percentages of stone expulsion across the board.
Timing of stone passage
Although the natural history of these stone studies gave a rough idea of the rates of spontaneous stone passage, evidence from RCTs has shown heterogenic results. The cumulative analysis in this review has yielded a more precise account of spontaneous stone passages. However, there remains a great disparity in the time to stone passage between all studies, with a wide range from 1 to 4 weeks. Canadian Urological Association (CUA) and EAU guidelines recommend 90% of chance of spontaneous passage of stones <5 mm within 40 days. 7,10 This review has found that the majority of stone expulsions were within 4 weeks, with an average of about 17 days.
Nonetheless, this was limited by the fact that all the studies included had limited their follow-up period to this range, with no longer follow-up periods. This was largely based on patient safety. Ergo it can be deemed safe practice to consider treatment of a stone if it has not passed after 4 weeks.
Safety
The rate of complications has been shown to have a direct relation to the duration of symptoms. Twenty percent of patients have complications if symptoms are >4 weeks when compared with 7%, if symptoms are <4 weeks in duration. 66 The current study revealed that only 5% required readmission, out of which only 1.1% had minor side effects in relation to the analgesia used.
Implications for practice
Reasonably easy accessibility of equipment (shockwave lithotripsy, semirigid, and flexible ureteroscopes), an increase in the number of trained endourologists, and patient expectations have not only expanded the indications for intervention for ureteral stone but also have spawned a significant increase in the ureteroscopic procedure in the last 10 years. 1,8 Unfortunately, all forms of procedures do come with certain risks.
Observation or expectant management of stone, until stone expels, is one of commonest management options for ureteral stone and appears attractive as it avoids invasive procedure, however, is associated with ambiguity and uncertainty, pain, potential loss of renal function, and, most importantly, for many, loss of work and family commitments. 70
The continuously debated topic of assisting stone expulsion with medical therapy adds an added question. As shown, α-blockers, specifically tamsulosin, can increase stone expulsion rates of stones in the distal ureter and of those >5 mm. Overall, can increase stone expulsion rates by at least 14%. 6,83 –85
Furthermore, the cost/benefit of conservatively managed stones can also sway the decision to avoid treatment. In the United States, it is reported that expectant (observation) management of ureteral stones has a $1200 cost advantage for distal ureteral stones and a $400 cost for proximal ureteral stones. 86
We believe that the current study is the largest cohort evaluation of natural history of ureteral stones and redefines the rate of passage of stones in relation to the size and location compared with previously published literature and current international urolithiasis guidelines. This also briefly gives an idea on the complication rate involved during the observation for ureteral stones.
Conclusion
Expectant management has an undeniable role in the treatment of ureteral stone patients. The outcome is largely determined on the stone size and location of the stone. Most ureteral stones <5 mm, especially those located in the middle and distal ureter, will pass spontaneously. Hence, it is acceptable for the urologist to observe for spontaneous stone passage for a period of time. Appropriate follow-up of these patients is obligatory to avoid complications. If spontaneous passage does not occur within a 4-week period, intervention is recommended. More importantly, this information helps to reduce patients' anxiety and supports them to make an evidence-based informed decision about conservative management as opposed to invasive treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.