
Abstract
Purpose:
Neutrophil gelatinase-associated lipocalin (NGAL) levels in the serum and urine are predictive biomarkers of acute kidney injury with correlation to complication and survival in major surgery. Salivary levels of NGAL during acute renal colic may reflect the degree of renal injury as it appears in different compartments encompassing body response in time perspective. Our aim is to evaluate and examine the feasibility and correlation of salivary NGAL with serum and urine levels in acute renal colic event.
Materials and Methods:
A prospective controlled study of all patients presenting to the emergency room with acute renal colic event diagnosed with single ureteral stone obstruction by noncontrast CT. Saliva, urine, and blood samples were collected in patients and a control group during the first morning of admission.
Results:
The study groups consisted of 44 patients and 13 controls, mean age 47 ± 15 years, body mass index 29 ± 6, mean stone size 6 ± 4 mm, mean creatinine levels 1.3 ± 0.7 mg/dL, mean white blood count 10,900 ± 3100 counts per field, and C-reactive protein 29 ± 55. Serum (190 ± 120 ng/mL vs 81 ± 24; p < 0.001) and predominantly salivary (474 ± 185 vs 328 ± 134 ng/mL; p < 0.05) NGAL levels were significantly elevated in patients compared with controls.
Conclusions:
Salivary NGAL sampling is feasible during the acute phase of renal colic. High levels of salivary NGAL are observed in a single sampling during acute ureteral stone obstruction and may advance clinical decision-making.
Introduction
R
Acute kidney injury (AKI) is not an uncommon complication of urolithiasis, with various studies reporting a 40%–75% association of AKI with sepsis. 6 Mortality can be associated with delay in diagnosis. 6 Early detection of AKI is of great importance to facilitate adequate decision to escalate or de-escalate monitoring of therapy.
Early diagnosis of AKI remains challenging because it relies on imperfect parameters, such as serum creatinine, which may only rise up to 2 days after kidney injury 7 and is influenced by systemic nonrenal factors. 8 New-generation renal biomarkers available today may affect clinical practice. 9
Neutrophil gelatinase-associated lipocalin (NGAL) is among the top unregulated genes of the lipocalin family in damaged kidney, which is expressed in serum and urine during tubular injury. 10 It is a small-sized protein filtered freely into the urine and any tubular damage in the proximal limb of the loop of Henle, or the collecting ducts, can be detected in urine within 2–4 hours. 10 –13
The diagnostic accuracy of NGAL in AKI is particularly in critically ill patients in the intensive care unit (ICU), following coronary angiographic catheterization with contrast media-induced AKI, cardiac surgery, kidney transplantation, 14 –16 and in hydronephrosis and ureteral stones. 17 –19
NGAL is expressed also in a variety of human tissues, including salivary glands. 19,20 A number of significant advantages over the assessment of serum samples have resulted in a steadily increasing interest in salivary sampling. Salivary sampling of cortisol has become an invaluable tool for both basic scientists and clinicians with reproducible results. 21 We proposed to investigate the role of salivary NGAL in acute renal colic. To the best of our knowledge, there are no data regarding salivary NGAL levels in AKI among patients admitted with acute renal colic secondary to an obstructing ureteral stone.
Materials and Methods
We conducted a prospective case–control study. All patients were referred with renal colic to the ER, diagnosed by noncontrast CT with ureteral obstruction due to a single ureteral stone; only patients admitted to the urology department were included in the study. Fifty-three consecutive patients were enrolled. The control group consisted of 14 healthy volunteers.
The study protocol was approved by the local ethics committee. Patients provided written informed consent. Epidemiologic and clinical data were recorded, and included patient age, sex, medication used, and the presence of coexisting clinical conditions. Urologic anamnesis included onset of symptoms, previous episodes of renal colic, history of ureterolithiasis, and previously performed procedures. Time to diagnosis, time to intervention, type of management, numbers of auxiliary procedures, and conservative monitoring were recorded.
Venous blood and urine samples were obtained from each patient at admission. Routine laboratory blood examinations included serum creatinine and electrolytes as markers to assess kidney function, C-reactive protein (CRP), and white blood count (WBC) as markers for an infectious process, coagulation profile, and aspartate transaminase and alanine transaminase as markers for liver function. Additional blood, urine, and saliva samples for the analysis of NGAL were collected at 07:00 following admission and stored at −80°C until further processing. Patients collected their saliva sample by a Salivette® device after receiving instructions that included not to eat or drink, or brush or floss teeth before collecting the saliva sample. Ureteral obstruction was classified as follows: (1) hydroureteronephrosis proximal to the ureteral stone, divided into three levels, mild, moderate, or severe; (2) perinephric stranding, defined as appearance of edema within the fat of the perirenal space divided into two levels of severity, mild or moderate to severe; and (3) the presence or absence of urinoma.
To rule out other causes that may influence NGAL levels, we excluded all the patients with preexisting chronic kidney disease, use of nephrotoxic drugs, congestive heart failure, recent cardiac catheterization, recent ICU admission, acute infection, diabetes mellitus, malignancy and obesity (body mass index >30 kg/m2), and immunocompromised patients. Serum (blood-bNGAL), salivary (sNGAL), and urinary (uNGAL) levels were evaluated using commercially available research-based enzyme-linked immunosorbent assay (ELISA); Human Lipocalin-2/NGAL Quantikine ELISA Kit test.
Statistical analysis
Data were statistically analyzed with SPSS (version 20; IBM, Armonk, NY). Before analysis, residuals were tested for normal distribution (Shapiro–Wilk test) and equality of variance (Levene's test). Nonparametric tests were used where appropriate. Group comparisons were calculated using the Student's independent t-test (parametric) and the Mann–Whitney U test (nonparametric), or Pearson's chi-squared test for categorical variables. Pearson correlation was used to assess the associations between continuous variables. According to the underlying hypotheses, a two-tailed test was performed. The significance level was set to p = 0.05. Values are given as means ± standard deviations. Locally weighted scatterplot smoothing was used to generate smooth lines exhibiting a nonparametric relationship between variables.
Results
A total of 53 patients diagnosed with a solitary ureteral stone obstruction and 14 healthy volunteers as a control group were enrolled in the study. Forty-four patients and 13 controls were included in the final analysis after excluding 10 cases due to technical concerns related to insufficient samples (Fig. 1). The average age was 46 ± 14 and 34 ± 6 years, and 41 and 6 men in the study and control groups, respectively. The clinical data of the patients are listed in Table 1.

Study design (technical issues; insufficient sampling/inappropriate transfer or storage, laboratory error*).
CRP = C-reactive protein.
In the study group, a significant increase in salivary NGAL levels was observed compared with individuals in the control group (474 ± 185 ng/mL vs 328 ± 134 ng/mL, p < 0.01). Blood NGAL levels as well as urinary NGAL levels were significantly increased in colic patients compared with the control group (190 ± 120 ng/mL vs 81 ± 24 ng/mL, p < 0.001 and 20 ± 22 ng/mL vs 9 ± 11 ng/mL, p < 0.05, respectively) (Table 2).
A statistically significant positive correlation was found between serum NGAL and salivary NGAL (p = 0.022), and serum NGAL and urinary NGAL (p = 0.042). A significant correlation between salivary and urinary NGAL was not detected.
Creatinine was measured at two points. The first sample was collected at admission and the second sample was collected the following day, at 07:00. Mean serum creatinine was 1.3 ± 0.7 mg/dL and 1.4 ± 0.5 mg/dL at admission and the following morning, respectively.
A highly significant correlation was observed between serum NGAL and creatinine level (p < 0.0001), and salivary NGAL and creatinine (p = 0.05), at admission.
We divided the AKI severity into three grades according to serum creatinine levels. Creatinine levels between 1.2 and 1.5 mg/dL, 1.5–2 mg/dL, and above 2 mg/dL were considered as mild, moderate, and severe AKI, respectively. A positive correlation was detected between serum NGAL elevation and AKI severity (Fig. 2).
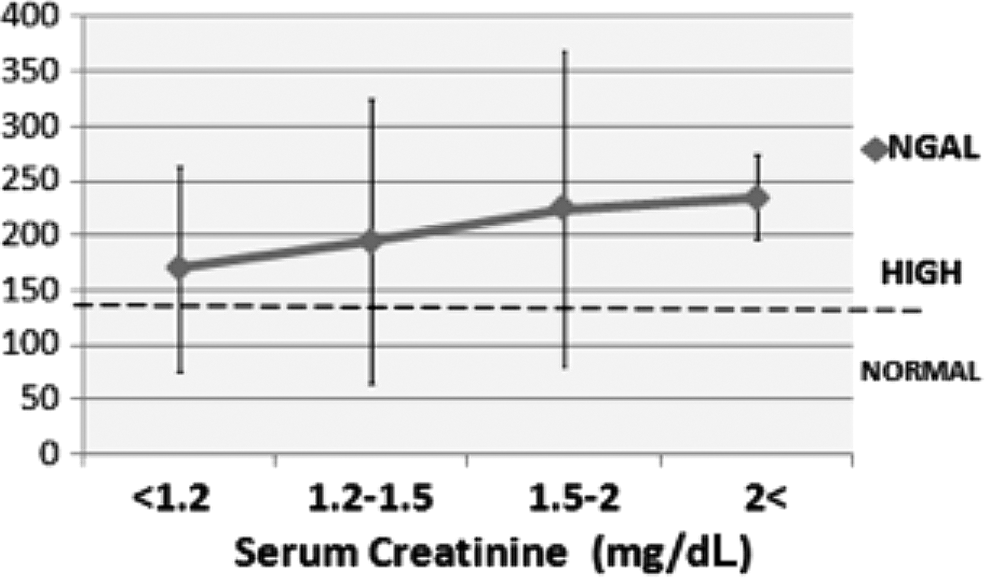
Serum NGAL and AKI levels. AKI = acute kidney injury; NGAL = neutrophil gelatinase-associated lipocalin.
Figure 3 shows the association between serum urine and salivary NGAL and AKI severity according to creatinine levels in the two groups.
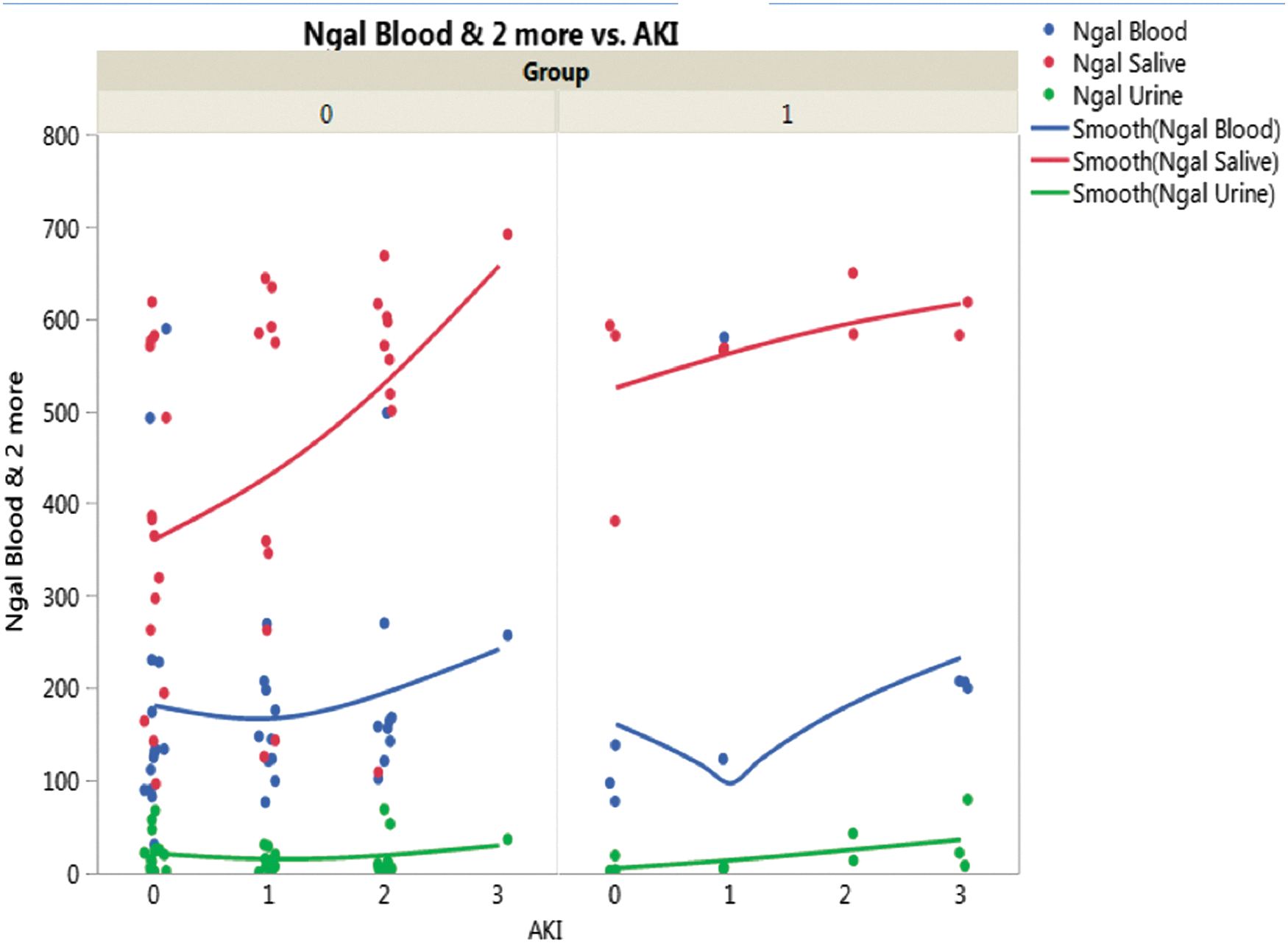
Serum, urine, and salivary NGAL and AKI levels.
No association was found between degree of hydronephrosis, stranding severity, presence of perinephric urinoma, and, any NGAL levels, or, between NGAL levels and different stone parameters. Urgent procedure (drainage with Double-J stent, percutaneous nephrostomy, and primary ureteroscopy) within 1 week from diagnosis was performed in 55% of patients. The remaining 45% of patients were managed conservatively. Significant difference in creatinine levels was observed between these two groups (1.5 ± 0.6 mg/dL vs 1.2 ± 0.3 mg/dL, p < 0.05). We calculated the ratio of NGAL/serum creatinine value in all samples separately: urine (96 ± 40 vs 94 ± 41, p = 0.23), serum (125 ± 112 vs 157 ± 120, p = 0.23), and saliva (334 ± 159 vs 409 ± 134, p < 0.05); a significance was found only in saliva NGAL/creatinine ratio between the patients who underwent an urgent intervention and those who were managed conservatively. However, no difference was found in NGAL levels between both groups. Also, no associations between WBC, CRP, and NGAL levels were found.
Discussion
Although creatinine is a marginally satisfactory biomarker of renal function, it is a notably poor biomarker of acute changes in renal function. This is largely because it takes days after a change in renal function before creatinine fully re-equilibrates. As such, the therapeutic opportunity to intervene and prevent kidney injury has often come and gone by the time we see the creatinine rise. Therefore, other markers of AKI are highly warranted. NGAL is one of such biomarkers that have been investigated during recent years. Because of its small size, NGAL is freely filtered by the glomerulus but almost completely reabsorbed in the proximal tubule. As a result, in the absence of AKI, plasma NGAL is strongly correlated with serum creatinine, but little is present in the urine, which was also reflected in the present data (healthy controls). During AKI, factors such as increased local distal nephron production of NGAL and decreased proximal tubular reabsorption of filtered NGAL result in a substantial increase in urine NGAL levels. 20 –25
In response to AKI, renal tubular production of NGAL substantially increases, contributing to high levels of NGAL detectable in the urine of animals and humans with acute tubular necrosis. 23,24 In contrast, mean urine NGAL levels increase 15-fold within 2 hours and by 25-fold at 4 and 6 hours after cardiopulmonary bypass. 24 In our study population, 40% of the patients with markedly elevated serum NGAL and 20% of those with elevated salivary NGAL levels were found to have normal serum creatinine levels at same time.
NGAL may be useful in differentiating prerenal disease from intrinsic renal injury. 26 In a mouse strain with a gene for bioluminescence and fluorescence inserted into the NGAL gene, imaging after ischemia/reperfusion demonstrated illumination of specific cells in the distal nephron, indicating NGAL production at the site of injury. No NGAL illumination was seen following maneuvers that lead to significant prerenal disease. 27
NGAL has been thought to reduce injury by inhibiting apoptosis and has been reported to upregulate heme oxygenase-1, which preserves proximal tubule N-cadherin and subsequently inhibits cell death, while creatinine may not reflect the apoptosis injury. 28 Elevated levels of NGAL have been reported also during urinary tract infection (UTI), 29 which makes NGAL a sensitive marker for intervention in reciprocal conditions.
NGAL has three isoforms: most of the synthesized NGAL is monomeric (25 kDa) or dimeric (45 kDa) and only a small fraction is heterodimeric (135 kDa—complexed with gelatinase). 30 Human renal tubular cells produce mainly the monomeric form, which was reflected by a predominance of the monomeric form in urine from patients with AKI, and neutrophils produce the dimeric form in patients with UTIs. 30 In our study, a total NGAL assay was used, which has a cross-reaction between the monomeric and dimeric form, as in the vast majority of published studies with NGAL.
Salivary sampling is increasingly used in clinical and scientific studies. 31 Saliva has many advantages over blood: it is a noninvasive, easily obtained, and painless procedure; collection does not demand highly trained personnel; samples are safer to handle with low or negligible rates of HIV transmission; and it is easier to ship and store. 32
It has been shown that there is an association between salivary and serum creatinine levels. 33 A positive correlation has been observed between serum and salivary urea and creatinine. 34
Urbschat et al. 18 showed a positive correlation between urinary NGAL, serum NGAL, and serum creatinine. In our study, in addition to the positive correlation with salivary NGAL, serum NGAL levels in the renal colic group were twice as (200%) high as the levels in the control group. It seems to be obvious that salivary NGAL reflects plasma NGAL; we found a significant correlation between plasma NGAL and urine NGAL. The correlation between salivary NGAL and urinary NGAL was not significant. We suggest a different reflection of systemic response in different body compartments that may encompass a time perspective. Aardal-Eriksson and colleagues 35 demonstrated a delayed salivary cortisol level compared with serum level in response to stress. Salivary NGAL levels may delay equilibrium long after urinary NGAL vanished. We measured salivary NGAL levels in the morning following admission, as such may represent a dynamic change in the course of the disease.
Salivary NGAL levels were elevated compared with control levels (130%). Interestingly, the absolute mean value of salivary NGAL was more than twice as high as the serum NGAL (470 vs 190 ng/mL). This is due to the nature of lipocalins, which are typically small extracellular proteins, in contrast to creatinine with the relative nonpolar nature that results in an incomplete permeability. 32
An expected finding in our study was higher WBC and CRP levels associated with increased NGAL. This seems to limit the value of NGAL as a tool for renal function assessing. We found that a statistically significant correlation was only found with salivary NGAL. No difference was found in NGAL levels between the patients who underwent urgent procedure vs patients who were managed conservatively, meanwhile significant difference was observed in creatinine levels. This may be due to a bias based on our tendency to drain patients with elevated creatinine. Interestingly, when we calculated the ratio of salivary NGAL\creatinine, significantly lower values were observed in the patients who underwent an urgent intervention compared with conservatively managed patients. This finding implies that this ratio may be used as an outcome predictive tool in the future.
Our study limitations are the small groups and hospitalized patients. In addition, we did not record NGAL levels at follow-up visits, however, our intension was to focus on the feasibly of a single noninvasive sampling during acute event, which may comprise time perspective. The definition of healthy people in the control group was based on anamnesis only, no creatinine test or further evaluation was performed, which may be considered as a limitation of the study.
This noninvasive single-sampling technique may make the difference in the management of ureteral stones. It may aid in the decision for intervention management and, in addition, it may facilitate identification of high-risk patients regarding medication adjustment and prevention of iatrogenic events.
Conclusions
Salivary NGAL sampling is feasible during the acute phase of renal colic. High levels of salivary NGAL were observed in a single sampling during acute ureteral stone obstruction, and correlated with serum creatinine, leukocytosis, and CRP. The serum creatinine level underestimates the actual AKI, while NGAL is a more sensitive and reliable biomarker in the case of renal colic secondary to obstructing ureterolithiasis. Further investigation is recommended to evaluate NGAL levels after stone treatment and at multiple intervals following the renal colic episode.
Footnotes
Author Disclosure Statement
No competing financial interests exist.