
Abstract
Introduction:
Thiazides and citrate prevent kidney stones and improve bone mineral density (BMD). The objective of this study was to opportunistically utilize the noncontrast CT (NCCT) scan used for stone detection to identify those with low BMD and follow the impact of potassium citrate and thiazides on longitudinal BMD measurements.
Materials and Methods:
A retrospective analysis was performed on 299 kidney stone patients treated with thiazides and/or potassium citrate for a minimum of 1 year. For each patient, BMD was estimated at L1 with CT attenuation measured in HU. A level of 160 HU was chosen to distinguish normal from low BMD. Pairwise t-test was used to compare the continuous outcomes before and after treatment for the whole cohort and the low BMD subgroup. Linear regression was performed to find if any association exists between the duration of follow-up and the changes in HU. A matched pair t-test was performed to compare among the medications used and the impact of their doses on the HU outcomes.
Results:
Patients with low BMD (HU <160) comprised (n = 186, 62.2%) the cohort. A total of 16.1% normalized after 1 year of treatment and 68% had an increase in HU. The mean change in HU was 8.6 (p = 0.0001). Linear regression demonstrated no association between the duration of treatment and the HU changes (p = 0.64). Hydrochlorothiazide (HCTZ) 50 mg was more effective at improving BMD (HU +19.7, p = 0.04) compared with 25 mg (+2.9) or 12.5 mg (HU +6.4). Majority of the low BMD subgroup were either postmenopausal women (n = 88) or men with age older than 60 (n = 74) and both showed a significant increase in HU (3.125, 10.731), p-value (0.0453, 0.0007), respectively.
Conclusion:
Stone health and bone health are synergistic. The impact of thiazides and citrates on BMD can be monitored opportunistically with the NCCT scan.
Introduction
N
The American Urological Association (AUA) guidelines, for the medical management of kidney stones, state that in addition to high fluid intake and dietary recommendations, thiazides and potassium citrate must be offered to patients with recurrent calcium stones. 15 However, besides being effective in the treatment of calcium stones, thiazides and alkaline citrate therapy can confer an additional benefit on bone mineral density (BMD), by slowing down bone loss and increasing bone mineralization. 15,16 In kidney stone formers associated with osteoporosis/osteopenia, thiazides can play a role in reducing the adverse effects of prolonged treatment with calcium supplements plus vitamin D that can increase the risk of nephrolithiasis. 8 Thus, in the context of multicomorbidities and polypharmacy, the medical therapy for kidney stones could have a positive impact on improving bone mineralization, optimizing patient treatment, and reducing unnecessary drug use.
In the same manner, imaging methods can be optimized, to reduce costs and radiation exposure. BMD, traditionally quantified by dual-energy X-ray absorptiometry (DEXA), 17 can also be evaluated by abdominal CT scan with acceptable sensitivity and specificity. 18 –21 Aside from its value in stone management, CT imaging is a valuable tool for assessing BMD since it carries no additional cost to the patient, does not require additional equipment, and no additional radiation exposure. Therefore, the aim of the present study was to evaluate the impact of potassium citrate and thiazide treatment for stone prevention on longitudinal BMD measurements from opportunistic CT scans, and correlate the doses of thiazides/potassium citrate with bone mineralization changes.
Materials and Methods
Study participants
Institutional review board approval was obtained to conduct a retrospective analysis of 299 kidney stone patients treated with thiazides and/or potassium citrate for stone prevention at our institution between August 2012 and August 2017. Subjects included in the study had a baseline CT imaging before the start of treatment and a 1-year follow-up CT study. All CT scans were done at Cleveland Clinic using low-dose protocol. Individuals with primary hyperparathyroidism, inflammatory bowel disease, renal tubular acidosis, long-term corticosteroid or bisphosphonate use, postmenopausal women on hormone replacement therapy (HRT), and prostate cancer patients on androgen deprivation therapy were excluded. Postmenopausal status was defined as female participants at age 50 and older. HRT was defined as the current use of estrogen pills/combination pills or estrogen patches/combination patches. Data on vitamin D and calcium supplement use were also obtained.
Data collection and measurements
Variables extracted from the registry included age, gender, body mass index (BMI), medical comorbidities (hypertension, diabetes, or coronary artery disease), predominate stone composition (>50%), alcohol and tobacco use, and any surgical treatment (URS, PCNL, cystolitholapaxy, or SWL). Pre- and post-treatment serum chemistry studies were also extracted and correlated with changes in BMD.
Bone mineral density
BMD was measured in a standardized manner with CT attenuation measured in HU, at baseline and after 1-year treatment with potassium citrate and/or thiazides. BMD was estimated by placing an oval region of interest on an area of vertebral body trabecular bone at the level of L1 with CT attenuation expressed in HU (Fig. 1). Based on previously published data, a threshold for a balanced sensitivity (73.9%) and specificity (70.6%) of 160 HU was chosen to distinguish normal from low BMD (osteopenia/osteoporosis). Patients with low BMD were identified and the changes in HU were analyzed.
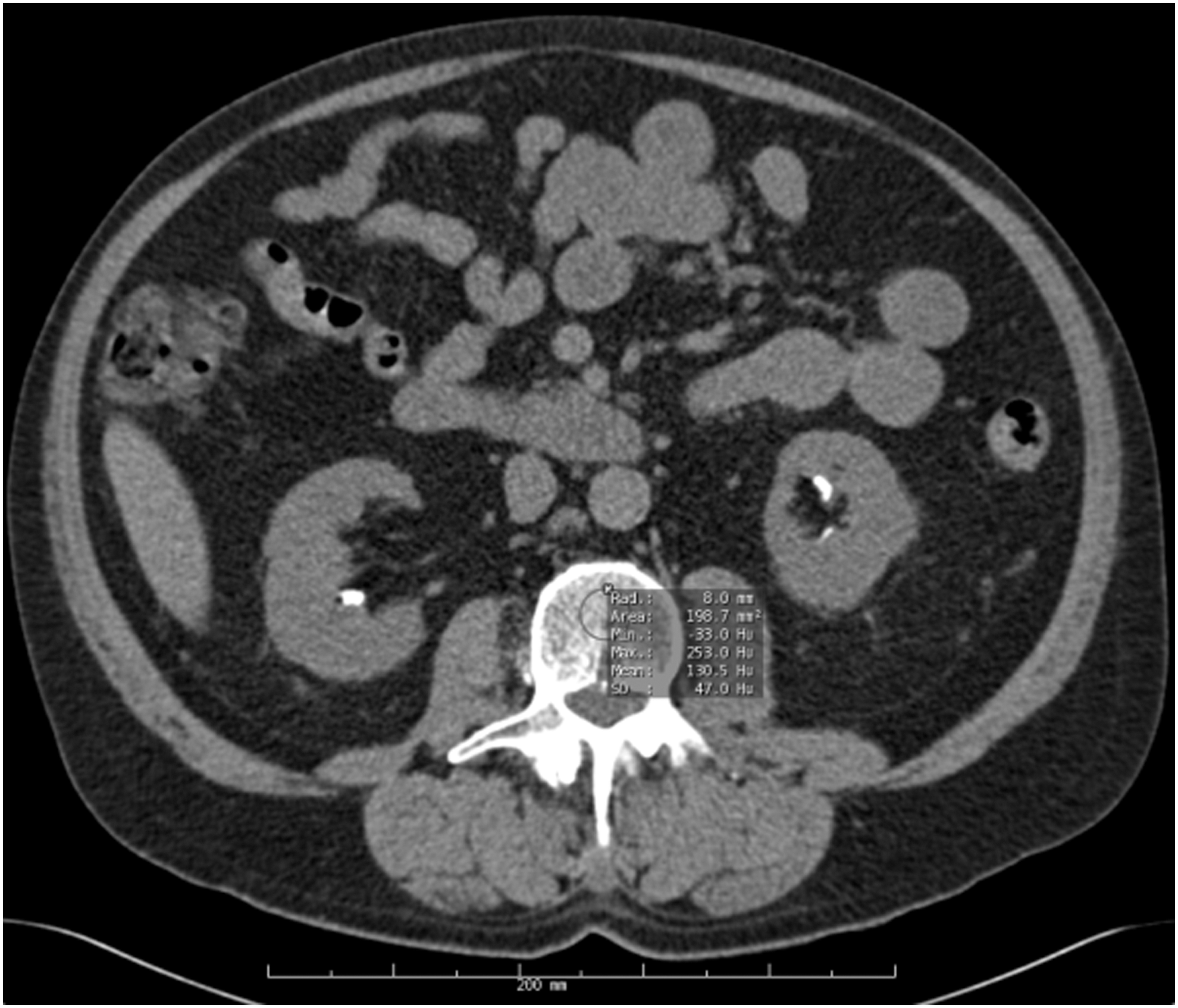
NCCT scan done for kidney stones can be used to estimate BMD by using imaging software with oval region of interest on an area of vertebral body trabecular bone at the first lumbar vertebra. CT attenuation is measured in HU. In the figure it shows low BMD (mean HU = 130.5). Based on previously published data, a threshold for a balanced sensitivity (73.9%) and specificity (70.6%) of 160 HU was chosen to distinguish normal from low BMD (osteopenia/osteoporosis). BMD = bone mineral density; NCCT = noncontrast CT.
Thiazides and potassium citrate
Information regarding the use of thiazides, potassium citrate, or both was obtained, as well as the different doses taken by each patient. The effect on BMD for each medication and for each dose was expressed in HU and investigated.
Statistical analyses
Means, standard deviations, and frequencies were used as descriptive statistics. Pairwise t-test was used to compare the continuous outcomes before and after treatment for the whole cohort, and the low BMD subgroup. Linear regression was performed to find the factors associated with BMD HU change and to show if any association exists between the duration of follow-up and the change in the HU for the whole cohort as well as the low BMD subgroup. Matched paired t-test was performed to compare the effect of both medications and their different doses on the HU outcomes. A p-value <0.05 was considered statistically significant. All statistical analyses were conducted in R 3.4.1.
Results
The baseline characteristics of the patients are shown (Table 1). In this cohort of 299 patients, the mean age was 62 ± 15.3 and males comprised 152 (50.8%). The mean BMI was 32 ± 7.77 kg/m2. From all patients, 81 (27%) did not undergo a surgical stone procedure. Calcium oxalate was the most predominant stone composition comprising 55.7%. The number of patients using vitamin D and/or calcium supplements was (n = 114, 38.13%), with calcium plus vitamin D (n = 63, 21.07%), vitamin D only (n = 47, 15.71%), and calcium only (n = 4, 1.34%).
BMI = body mass index; CAD = coronary artery disease; PCNL = percutaneous nephrolithotomy; SD = standard deviation; SWL = extracorporeal shock wave lithotripsy.
The mean HU on CT after treatment was higher compared with before treatment (152 ± 62 vs 146 ± 56.9, p = 0.0005) (Fig. 2). From the total cohort, 197 (65.9%) had an increase in HU from baseline after treatment. In the patients with low baseline BMD (<160 HU; n = 186, 62.2%), 16% normalized BMD (≥160 HU) after treatment and 68.3% in total had an increase in HU (p = 0.0001) (Fig. 3). The majority of the low BMD subgroup were either postmenopausal women (n = 88, 47.31%) or men older than 60 (n = 74, 39.8%) and both showed a significant increase in HU (+3.125; +10.731), p-value (0.0453, 0.0007), respectively. Premenopausal women were more likely to see increases in BMD with a mean change in HU (+49.5, p = 0.023) as were men younger than 60 with a mean change in HU (+14.8, p = 0.0115) (Table 2).

Scattered plot graph comparing between the mean HU measured by CT, pre- and post-treatment with thiazides and/or potassium citrate. The post-treatment HU is generally higher. The change in HU ranged between −62.1 and 152.1, with a mean of 8.6 (p = 0.0001) and 95% CI (4.81–12.37). CI = confidence interval.

Comparison between the number of patients with low and normal BMD before and after treatment with thiazides and/or potassium citrate. Patients with low BMD (HU <160) comprised (n = 186, 62.2%) the cohort. A total of 16.1% normalized after 1 year of treatment and 68% had an increase in HU.
BMD = bone mineral density.
The effect on the HU outcomes by each thiazide and/or potassium citrate with their different doses is shown (Table 3). Hydrochlorothiazide 50 mg/day was more effective at improving BMD compared with 25 or 12.5 mg (HU +19.7, +2.9, and +6.4, respectively, p = 0.04). Also, potassium citrate 20 mEq was more effective at improving BMD compared with the other doses (HU +12.2, p = 0.004). Citrate single therapy showed a better effect on BMD (HU +8.355, p = 0.003) than thiazide only (HU +5.522) or both combined (HU +0.735). A linear regression analysis for the pre- and post-treatment serum chemistries did not show any association with HU changes, except for serum calcium, a marginal predictor for HU change (p = 0.039).
A baseline 24 hours urine collection was performed in 110 (37%) patients and hypercalcuria was present in 32 (29%). Low BMD was found in 50% (16) of hypercalciuric patients, and 12.5% normalized BMD after treatment. In the normocalciuric patients, low BMD was found in 57% (45) and 15% normalized after treatment. Both hypercalciuric and normocalciuric patients with low BMD had significant increase in HU after treatment (p = 0.017, p = 0.02), respectively.
The mean follow-up for the whole cohort and low BMD group was 552 and 533 days, respectively, as all patients had a minimum of 1-year follow-up. Linear regression models demonstrated no association between the duration of treatment and the HU changes in both the cohort (p = 0.64) and low BMD subgroup (p = 0.61).
Discussion
Opportunistic imaging with noncontrast CT (NCCT) obtained for the diagnosis and management of stone disease offers the opportunity to identify those patients with low BMD, and monitor response to medical therapy. NCCT scan obtained for nephrolithiasis can be used as a valuable tool for assessing BMD since it carries no additional cost to the patient, does not require additional equipment, and avoids additional radiation exposure associated with standard DEXA studies used for screening of BMD. NCCT does not completely replace DEXA for BMD screening, but rather be used opportunistically to evaluate BMD in patients with CT images available and with no DEXA performed before. In our study, we observed the effect of drugs on BMD with treatment. Previous studies show the effects of each drug were observed in the first 6 to 12 months, but thereafter remain stable 20 ; a finding confirmed in our patients as duration of treatment beyond 1 year did not impact outcomes.
Several population-based studies have highlighted a rising prevalence and incidence of nephrolithiasis over the last several decades, affecting nearly 10.6% of men and 7% of women in the United States. 1 The National Health and Nutrition Examination Survey (NHANES) demonstrated an increase in the prevalence of kidney stones from 3.1% in young adults to 19.1% in males and 9.4% in females, between 60 and 69 years of age. 22 Aside from the aging of kidney stone formers, a clear association with age-related diseases has been established. Obesity, 1,3 hypertension, 4,23 diabetes, 5,23 metabolic syndrome, 24 chronic kidney disease, 6 and osteopenia/osteoporosis 7 have all been linked to urinary stone disease. NHANES III included data on BMD and demonstrated that kidney stones were significantly associated with lower BMD and risk of fractures. 25 In fact, 50% of idiopathic renal stone patients with recurrent calcium stones have osteopenia while the osteoporosis rate can reach 30%. 7 –9 In accordance with these tendencies, our cohort was represented by geriatric patients (mean age of 62) and with comorbidities related to metabolic syndrome. Hypertension and diabetes were identified in 82% and 41.8% of the cohort, respectively, and the mean BMI was 32 mg/kg2 (Table 1).
Given the rising tide of kidney stone formers aging and age-related diseases, polypharmacy has become a current concern in this group. 10 Medications that are not indicated, not effective, or constitute a therapeutic duplication would be considered polypharmacy. 10,26 The negative health effects of taking multiple medications are the increased risk of adverse drug event, drug interaction, and medication nonadherence. 10 Moreover, polypharmacy increases healthcare costs to both patients and the healthcare system. 13,14 This highlights the negative consequences associated with polypharmacy and points for innovative interventions to reduce unnecessary drug use and improve patient care. For recurrent stone formers, aside from high fluid intake and dietary recommendations, the pharmacologic therapy with thiazides and potassium citrate remains a strong recommendation by the AUA guidelines. 27 Besides being effective in the treatment of calcium stones, an additional benefit has been observed on BMD. Thiazides not only slow down bone loss but also enhance bone mineralization. Therefore, thiazides can benefit both kidney stones and low BMD, reduce the number of medications, and optimize patient care.
A number of mechanisms have been proposed to explain the positive effects of thiazides on BMD. The hypocalciuric effect of thiazides results in a positive calcium balance that in turn may suppress parathyroid hormone (PTH) and decrease bone resorption with a result of improving BMD. The magnitude of this effect on bone density has been shown to be similar to that obtained with vitamin D and calcium supplementation, without the associated increased risk of lithiasis. 7,8 Furthermore, thiazides can play a role in reducing the adverse effects of prolonged treatment with calcium plus vitamin. 9 Potassium citrate therapy also should be offered to patients with recurrent calcium stones since randomized control trials (RCTs) have demonstrated that potassium citrate is associated with reduced risk of recurrent calcium stones in patients with hypocitraturia. 28,29 Potassium citrate also prevents bone loss by providing an alkali load that buffers the bone resorbing effect of acid excess 15 and, maybe, also by a reduction of PTH secretion, as citraturia is inversely correlated with PTH.
As in previous studies, our results confirmed the positive effect of thiazides and/or potassium citrate on bone mineralization. After a mean period of 552 days for the whole cohort and 533 days for the low BMD subgroup, 65.9% and 68.3%, respectively, had an increase in BMD evaluated by an opportunistic CT scan (Fig. 2). In addition, 16% of the low BMD subgroup had their BMD normalized after treatment (Fig. 3). The majority of patients with low BMD are either postmenopausal females older than 50 (47.31%) or men older than 60 (39.8%), (Table 2). Hormonal changes are common in these age groups of both genders, effecting bone mineralization. Our results showed an improvement in the BMD with an increase in HU that reflects the positive and synergetic effect of thiazides and potassium citrate on these particular age groups, by simultaneously treating their stones and improving their age-related bone health. It is shown, especially for women with history of kidney stones or hypertension, that thiazides can provide a further option in the prevention of postmenopausal bone loss. 20 Treatment strategies that include age, stone disease, low BMD, and hormonal status can be further studied in RCTs to come up with the best balance in medications to combat bone loss with less cost and side effects.
DEXA is the gold standard method for measuring BMD, by estimating BMD at two skeletal sites that have a higher risk of osteoporotic fractures (lumbar spine and proximal femur) with acceptable accuracy, precision, and low radiation. 17,30 However, BMD can also be evaluated by abdominal CT scan with acceptable sensitivity and specificity. 18 –21 Based on previously published data, a threshold for a balanced sensitivity (73.9%) and specificity (70.6%) of 160 HU was chosen to distinguish normal from low BMD (osteopenia/osteoporosis). 18 In accordance with practices to reduce unnecessary drug use and costs related to healthcare, the rational use of image methods becomes an important issue, especially in regard to radiation exposure, to both patients and healthcare providers. In this study, taking this relevant point in consideration, we evaluated the impact of thiazides and potassium citrate on BMD using an opportunistic CT scan.
Besides investigating the role of thiazides and/or potassium citrate on BMD, we correlated the different doses of the medications with changes in BMD expressed by HU. The analysis revealed that different doses of thiazide and potassium citrate have a different effect on BMD. We found that hydrochlorothiazide 50 mg had the best effect in improving BMD compared with the other thiazide doses. Also, we found that potassium citrate 20 mEq was more effective in improving BMD than the other doses, and using potassium citrate only had a better effect on BMD compared with thiazide only or both combined (Table 3). We postulate that potassium citrate has a relatively better effect by exerting an alkali load, which buffers the endogenous acid production that inhibits bone resorption and improves bone mass by its hypocalciuric effect and a sustained stimulation of osteoblast activity. 15
This is the first study to demonstrate the benefits of thiazides and/or potassium citrate on BMD evaluated by an opportunistic CT scan. Furthermore, it points out for medical practices to consider the use of innovative interventions to reduce unnecessary drug use and radiation exposure in correlated medical conditions such as stone disease and low BMD. However, several limitations regarding our study warrant mentioning. First, the diagnoses of low BMD were based solely on CT findings and were not confirmed with the gold standard DEXA scan. However, HU parameters were used based on prior studies that confirmed a good balance of sensitivity and specificity compared with the DEXA scan. Second, only one-third of our patients had a baseline 24-hour urine collection. Also, being a retrospective study, the dose-specific effect of thiazide on BMD could have been effected by other cofounders such as hypertension that was found in 82% of the cohort.
Conclusions
Stone health and bone health are synergistic. Opportunistic treatment of low BMD with stone prevention approaches, by incorporating thiazides and citrates, can be also monitored opportunistically with the NCCT scan.
Footnotes
Author Disclosure Statement
No competing financial interests exist.