
Abstract
Background:
To describe the clinical characteristics, infectious and kidney function patterns, and overall outcomes in a cohort of patients with staghorn calculi treated conservatively.
Methods:
Staghorn calculi treated nonoperatively between January 2009 and January 2017 were identified. A retrospective analysis was completed.
Results:
Twenty-nine patients were identified with a median age of 74 years (interquartile range [IQR] 61–81). Mean follow-up was 24 months. Fifty-nine percent (17/29) had complete staghorn calculi with 6/29 (21%) bilateral. Mean body mass index was 29.4 (IQR 24.8–31.7). Of the 29 patients, 14 were treated conservatively due to comorbidities, 12 refused treatments, and 3 were due to aberrant anatomy. The age-adjusted Charlson Comorbidity Index (CCI) score demonstrated 8 patients in our cohort with a CCI of <3, 11 patients with a CCI of 4 or 5, 7 patients with a CCI of 6 or 7, and 3 patients with a CCI of >8. Overall, kidney function remained stable for 19/29 patients (66%) and the glomerular filtration rate decreased by <10% for 4/29 (14%), by 10%–29% for 2/29 (7%), and >30% for 4/29 patients (14%) over the study period. None of the study patients required hemodialysis. No patients in the cohort developed an abscess, nor were any patients on daily prophylactic antibiotics. There was only one related admission for a complication during the study; this was for pyelonephritis. There were two deaths during the study period. One death was an unrelated cardiac death and the other was from urosepsis; this patient had been noncompliant with follow-up.
Conclusions:
Outcomes for patients treated conservatively were reasonable in this select group. There is a need for future prospective studies to show whether conservative treatment of these patients is safe.
Introduction
S
Data in the literature regarding the sequelae of conservative management are limited, but this information is critical to the decision-making process for symptom-free patients with poor reserve and high surgical risk. Surgical treatment of staghorn calculi has been the mainstay of treatment based on studies dating back to the 1970s, which showed a >50% death rate from renal failure over a 17-year study period. 1 Reports of conservative therapy show high rates of nephrectomy and an increase in associated morbidity and mortality rates; the most common causes of death are chronic kidney failure and urosepsis, with reported mortality rates ranging from 9% to 47%. 2,3 However, two studies have challenged that paradigm and concluded that conservative management could be safe in select patients with appropriate monitoring. 3,4 Both studies were small and do not account for patient comorbidities; our study adds to this body of data.
We reviewed our institutional experience over the past 10 years to describe the clinical characteristics, infectious and kidney function patterns, and overall outcomes in patients with staghorn calculi managed nonoperatively.
Methods
Study population
Using a Boolean search (keyword-based text search using logical operators such as AND, OR, and NOT) of outpatient office visits within the electronic medical record, we identified patients diagnosed with having staghorn calculi seen by one of four surgeons at our institution between January 2007 and January 2017. All patients had confirmed CT radiographic diagnosis of partial or complete staghorn calculi. The diagnosis was made by one of the abdominal radiologists at our institution, all of which have both gastrointestinal and genitourinary specialized training. The authors of the study verified the diagnosis by also reviewing the images. We then selected patients in this group who had been treated conservatively.
Outcomes
Patient demographics, comorbidities, medical management, laterality, presenting symptoms, metabolic evaluation, urine culture data, renal function over time, treatment, morbidities, and outcomes, including overall survival (OS), were evaluated upon retrospective review of the electronic medical record. Patients managed conservatively did not have antibiotics, ureteral stents, ureteroscopy, nephrostomy tubes, or any other surgical stone procedure. They were followed with basic metabolic panels plus renal ultrasound or CT scan (based on surgeon preference) every 6–12 months. Recommendations for oral medications such as potassium citrate, increased fluid intake, and optimization of 24-hour urine parameters were advised to all patients. Patients treated with conservative management were not on prophylactic antibiotics. The estimated glomerular filtration rate (GFR) was calculated using the Modification of Diet in Renal Disease study equation. Dialysis rates were also calculated. OS was recorded from the date of radiographic diagnosis. Dates of death were obtained from the medical record and a search of public death records.
The Charlson Comorbidity Index (CCI) was used to outline the mortality risk in patients with several comorbidities. CCI scores were calculated using an online calculator, 5 which has been previously validated in patients undergoing percutaneous nephrolithotomy. 6,7 As used in other studies, four comorbidity groups were established based on the 25th, 50th, and 75th percentile ranking of comorbidity scores: low (score of ≤3), moderate (score of 4 or 5), high (score of 6 or 7), and very high (score ≥8). 8
We defined urosepsis as any patient meeting at least two systemic inflammatory response syndrome criteria (tachycardia, temperature >38 or <36, tachypnea, or white blood cells >12) with an established urinary tract infection (UTI). UTI was defined as >100,000 colony-forming units of one species on urine culture. Urinalysis and urine cultures were only obtained for patients with symptoms. Staghorn-related death was any documented death from associated urosepsis or kidney failure. As done in other series, 3 we defined progressive kidney failure as any decline in GFR >30% during the course of treatment as this would represent a clinically significant change in renal function. The urologists who authored the article categorized each staghorn as either partial or complete. Partial staghorn calculi were defined as any branched renal stone extending into at least two calices. Complete staghorn was defined as any stone occupying virtually all of the collecting system.
Statistical analyses
Descriptive statistics were performed by calculating frequencies of categorical variables and the median and interquartile range (IQR) for continuous variables. Analyses were performed using SPSS software, version 20 (IBM Corp., Armonk, NY). The University of Pittsburgh institutional review board approved the study (PRO16050495).
Results
Of 176 patients identified, we treated 29 patients (16%) conservatively during the study period; 16 were male. The median age was 74 years (IQR 61–81). Each patient was followed for a mean of 24 months (standard deviation = 29.8 months). Complete staghorn calculi were seen in 17/29 (59%) and 6/29 (21%) were bilateral. The mean body mass index for the cohort was 29.4.
Of the 29 patients in the study, there were two groups: 17 were treated conservatively due to comorbidities (14) or aberrant anatomy (3) and 12 patients refused treatments. Additionally, two of the patients had advanced age and three were on anticoagulation. The age-adjusted CCI scores were calculated for each patient. In the total cohort, there were 8 patients with a CCI of <3, 11 patients with a CCI of 4 or 5, 7 patients with a CCI of 6 or 7, and 3 patients with a CCI >8 (Fig. 1). Many of those patients with a low CCI were in the group that refused treatment; in this group, there were eight patients with a CCI <3, five patients with a CCI of 4 or 5, two patients with a CCI of 6 or 7, and only one patient with a CCI >8. The estimated 2-year OS rate for each group based on the score was as follows: scores <3 were 95%, scores 4 and 5 were 80%, scores 6 and 7 were 55%, and scores >8 were 35%. Age was included in this score (Table 1).
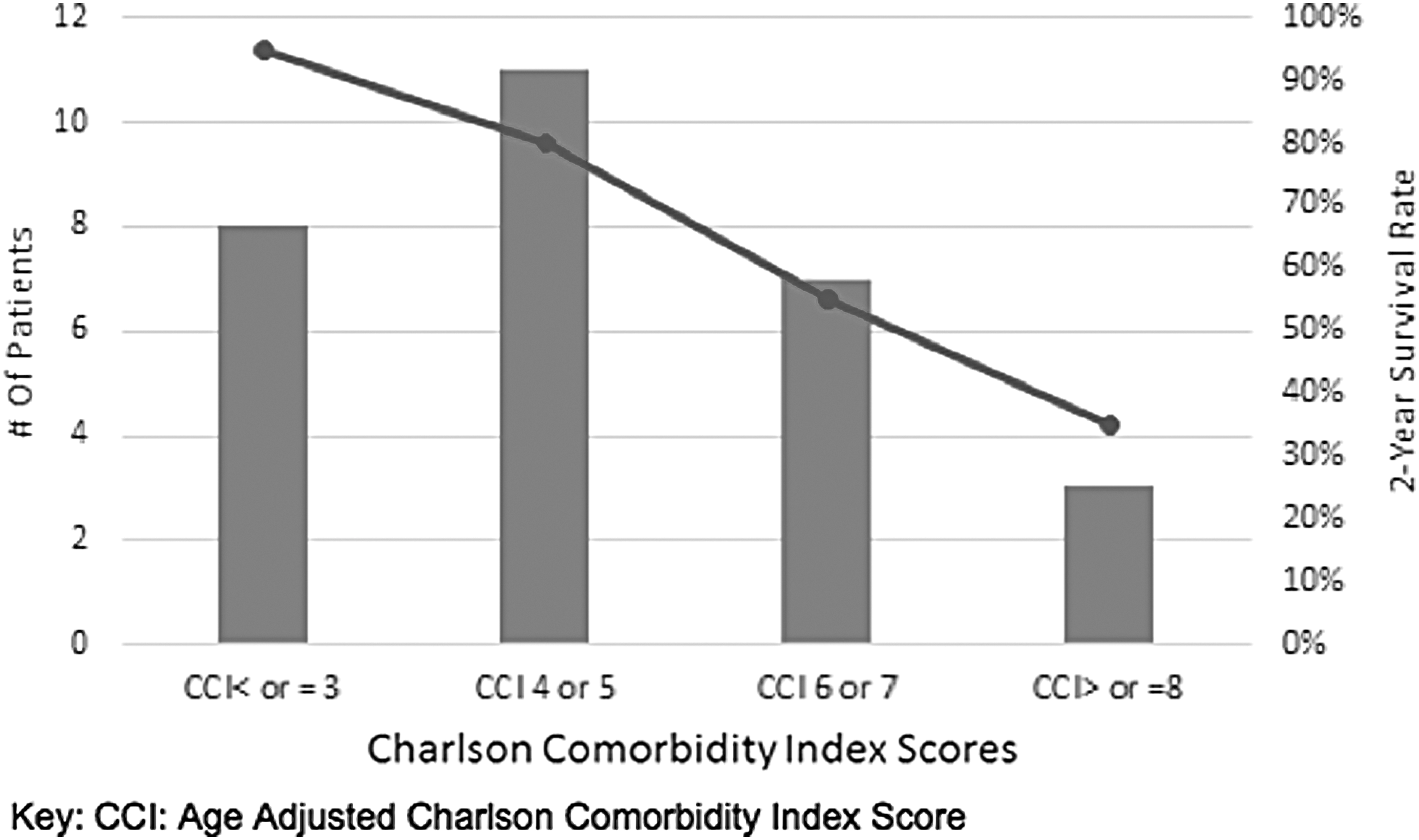
Patient groups based on age-adjusted Charlson Comorbidity Index scores.
Regarding age, for each decade >40, a score of 1 was added to the comorbidity score.
To evaluate renal deterioration, the GFR level was followed for each patient during the study period. The GFR stayed the same or improved for 19/29 patients (66%), GFR decreased by <10% for 4/29 (14%), by 10%–29% for 2/29 (7%), and by ≥30% for 4/29 patients (14%) (Fig. 2). While 28/29 (97%) patients were provided a prescription for a 24-hour urine test, only 16 patients (55%) completed it. Of the 16 completed studies, 7 (44%) had low volume, 7 (44%) had hypocitraturia, 4 (25%) had hyperoxaluria, and 4 (25%) had hypercalciuria.

Change in renal function of patients managed conservatively.
All patients were asymptomatic at presentation and patient complaints were minor during the study period, but included bladder infection (21%), gross hematuria (17%), and flank pain (7%). In the cohort, there were two patients who experienced clinical pyelonephritis. One of those patients was admitted to the hospital for antibiotic treatment. This represented the only related hospital admission in the group. No one developed a renal or perinephric abscess. During the study period, none of the patients were placed on hemodialysis. There were two documented deaths during the study period. One death was unrelated and the other was due to urosepsis in a noncompliant patient who had been recommended to undergo surgical treatment. OS was 100 months (95% confidence interval [CI] 89–110) with disease-specific survival of 104 months (95% CI 91–111).
Evaluating patients with unilateral and bilateral stone groups separately, there was no statistically significant difference between patient-reported symptoms (4% vs 17% pain, 22% vs 0% hematuria, and 22% vs 17% UTI, respectively) and rates of renal failure progression (17% vs 0%, respectively). However, OS in the unilateral stone group was 103 months vs 87 months in the bilateral stone group (95% CI 56–119). Similarly, disease-specific survival for the unilateral and bilateral groups was 103 months (95% CI 93–113) and 88 months (95% CI 89–110), respectively.
Discussion
Staghorn calculi are large renal stones that remain a treatment challenge especially in patients of advanced age or those with poor surgical candidacy due to high frailty. While treatment is advised in all eligible patients due to risks of recurrent infection, urosepsis, and kidney failure, some patients may benefit from conservative management. We document reasonable short-term success caring for a small cohort of patients conservatively.
Literature supporting surgical management of this condition is robust, often citing the risks (including mortality) associated with the natural history of staghorn calculi. 1 –3,9 –12 Staghorn calculi are thought to damage the kidney through obstruction, recurrent infections, chronic inflammation, and fibrosis. 13 Renal decline in these patients has been reported from 14% to 50%. 1,3 These data have led to the 2016 American Urological Association guideline recommending surgical removal of staghorn stones if associated comorbidities do not preclude treatment. 14 However, in high-risk patients, it is paramount to analyze the cost and benefit of treatment with procedural risks in mind such as sepsis, bleeding, renal colic, cardiothoracic events, and even death. 7,15,16 These procedures are often long and multiple with early complication rates up to 50% in some series, 16 especially in patients with a high CCI score. 7
Based on CCI scores calculated for our cohort, 10/29 (34%) had a 2-year survival estimate of 55% or less. We followed patients for a mean of 24 months, so these results are particularly valuable for those patients who have limited life expectancy. Kidney function was monitored by GFR levels, and fortunately, few patients had decline in renal function. Clinically stable renal function was seen in 83% of patients, with only 4/29 (14%) demonstrating a declining GFR by ≥30% in the study period. Less than a third of patients endorsed a complaint such as UTI, gross hematuria, or flank pain. There was only one related hospital admission in this group and it was for pyelonephritis. There were two deaths during the study and one was attributed to urosepsis. Notably, this patient was in the group that refused treatment despite receiving recommendations for surgical removal, highlighting that conservative management is not appropriate for everybody. The patient also had bilateral staghorn calculi, poor health, was lost to follow-up, and presented in florid sepsis, which ultimately caused his demise. This patient outcome also underscores the importance of close follow-up if put on a conservative management pathway. Although 97% of patients were provided a prescription for a 24-hour urine test, only 16 (55%) completed it. No patients went on to surgery during the study period.
Few studies in the literature have looked at a conservative approach in select patients. 4 Deutsch and Subramonian 3 looked at 22 patients and showed a 14% progressive renal failure rate and a 9% dialysis rate, but concluded that conservative management is probably safer than previously thought. Fortunately, none of our patients went on to require hemodialysis; however, our progressive renal failure rate was also 14%.
Prior studies have determined that bilateral calculi or staghorn calculi of solitary kidneys are more strongly associated with long-term complications. 3 This is likely to be true; however, we did not demonstrate these trends in our study. None of the patients included in our study had a solitary kidney. We did not find any statistically significant differences in renal failure rates or symptoms between groups, but we did find a difference in OS between groups. Patients with unilateral stone disease had an OS of 103 months (95% CI 93–110) vs 89 months (95% CI 56–119) with bilateral stone disease.
The findings of this study must be considered in the context of several limitations. Given the rarity of conservative management of this disease, our series is limited to a small number of patients. Patients were only followed for a mean of 24 months and thus may not capture the time frame required to demonstrate clinically significant decline in renal function or morbidity. However, many patients unfit for surgery have limited life expectancy, so a 2-year follow-up may be relevant to this group. Given that the reason behind conservative management is variable among these patients, our cohort is heterogeneous. These patients were also treated at a large academic center, limiting the generalizability to other populations. However, we feel that these findings add to a paucity of data regarding the natural history of conservative treatment of this population.
Given that the mechanism for renal decline begins with inflammation from recurrent infections, 13 management of infections (and infection stones) is important. We did not have stone composition data for the majority of patients since they were treated conservatively; this information could change the treatment approach as infections and metabolic-based stones are likely to have different outcomes.
Despite these limitations, our experience adds to the current body of literature describing this rare management approach. Although surgical treatment of staghorn stones is clearly the standard of care when possible, it may be safe (or in some cases, safer) to manage select patients nonoperatively with few complications or readmissions. Future efforts should focus on developing a more standardized follow-up and treatment plan for patients in this subgroup. Further prospective studies with more longitudinal follow-up are warranted to examine both the benefits and risks of conservative management in this population.
Conclusions
Outcomes for patients treated conservatively were reasonable in this select group. There is a need for future prospective studies to show whether conservative treatment of these patients is safe.
Footnotes
Author Disclosure Statement
No competing financial interests exist.