
Abstract
Introduction: To make percutaneous access easier in PCNL, we developed Automated Needle Targeting with X-ray (ANT-X).
Method: ANT-X uses an image registration software with a closed loop feedback system to autoalign the puncture needle to the desired calyx using the bullseye technique. We tried percutaneous punctures on a live pig model and compared the results with free-hand technique. We then performed our first PCNL in a human subject with the aid of ANT-X. Our patient was a 48 year-old gentleman with a 1.4cm left lower pole stone.
Results: Initial results for live animal trial showed radiation exposure for robot-assisted arm during puncture was reduced by 26% compared to the free-hand technique (8.2mGy vs 11.2mGy). In the human trial, obtaining percutaneous access was successful at first attempt.
Conclusion: ANT-X system can help surgeons feel confident and potentially reduce complications, hence enabling more surgeons to adopt this procedure.
Introduction
Percutaneous Nephrolithotomy (PCNL) is a minimally-invasive surgery used for treatment of large renal stones. However, difficult punctures can lead to complications such as bleeding, pneumo/hemothorax, injuries to surrounding organs and failure of access.
In addition, not all general urologists are comfortable with establishing percutaneous access by themselves. Sometimes, access may be performed by an interventional radiologist. Unfortunately, access by radiologists may be less ideal for stone clearance 1 .
Over the last decade, there have been many developments to improve PCNL outcomes with better imaging techniques and automated systems for targeting 2 .
Two main promising technology models with potential for improving outcomes of percutaneous access are computer-assisted navigation systems and automated robots.
Computer-assisted navigation systems such as that developed by Rassweiler et al in 2012 3 , enables the surgeon to visualize the relation of calyceal anatomy to surgical instruments by placing radio-opaque markers on patient and surgical instruments and superimposing them on the 3D-reconstructed preoperative computed tomography (CT) images. This helps surgeons obtain access more efficiently but it does not adjust for real-time position of the kidneys during respiratory movements, hence automated devices may offer an advantage.
From as early as 1997, Cadeddu, Stoianovici, et al. from URobotics Laboratory at Johns Hopkins (JH) Medical Institutions have developed the PAKY-RCM system 4-5 . The team successfully reported the feasibility of their system in a clinical trial with 23 patients who underwent PCNL with the PAKY-RCM system in 2002 6 .
In another project by JH URobotics, Pollock et al. in 2010 7 showed that their automated device, AcuBot, perform better at percutaneous ablative targeting than computer-assisted navigation system or manual operation. The AutoBot, mounted on a CT scanner, processes the CT images to enable automatic needle alignment. The surgeon then drives the needle using a remote joystick.
While these systems potentially improve the outcome of percutaneous access, they are expensive, bulky and complex to set up which limited their widespread use in clinical setting.
Therefore, we aimed to develop a system that is accurate and efficient in achieving percutaneous needle placement; yet compact and user-friendly, so that its use can be employed in clinical practice by general urologists who want to perform PCNLs.
In this paper, we present our device, ANT-X (Automated Needle Targeting with X-ray) to add to the armamentarium for percutaneous renal access.
Methods
The engineers from NDR Medical Pte. Ltd. designed and built the ANT-X system. All funding for this project was supported by NDR Medical Pte. Ltd.
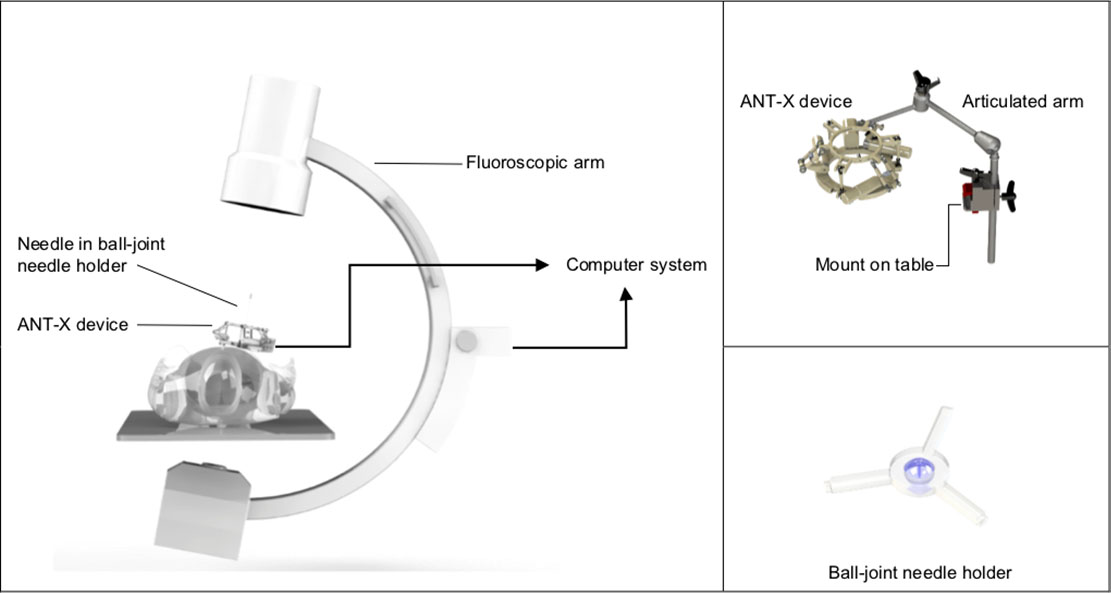
The ANT-X system is for use in prone PCNL with fluoroscopic imaging using the bullseye technique. The system consists of a single-use ball-joint needle holder placed within the ANT-X device with an articulated arm, mounted on the operating table. The ANT-X device and the fluoroscopic arm are connected to the computer system to form a close-loop feedback system (Figure 1). The ANT-X device with the articulated arm can be sterilized in a standard autoclave machine after each use.
Set up of ANT-X system
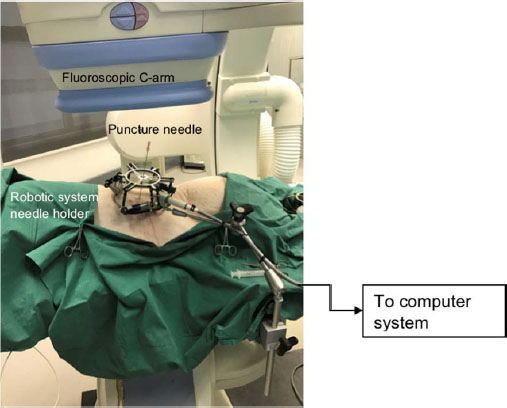
Set up of porcine model trial
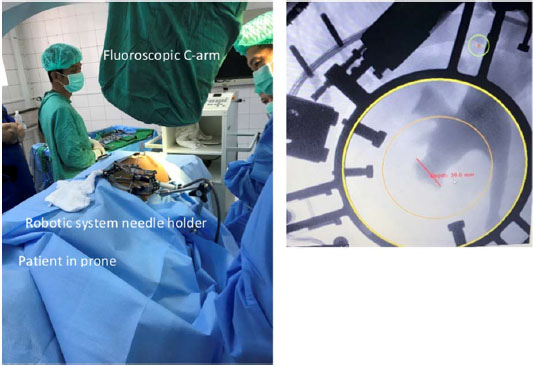
Set up of first human patient PCNL using ANT-X (left); Picture of renal collecting system on ANT-X targeting software (right)
ANT-X works on the following principles: The collecting system is lit up via retrograde pyelogram and the surgeon chooses the appropriate calyx for entry by placing a skin stab incision over the area. The needle holder ring is positioned in close proximity to the point of entry. The needle is inserted into the needle holder and pivoted on the incision site. Fluoroscopic images are obtained by the C-arm at 30 degrees and imported to the system using DICOM or any other video output methods deployed by the common C-arms available in the market. ANT-X integrates the images with the real-time position of the needle mounted on the device by using transformative projection
1
. The needle is automatically aligned for puncture into the chosen calyx based on the correlation of these coordinates Once auto-alignment is completed, the needle holder keeps the needle angle stable as the surgeon advances the needle into the calyx. Fluoroscopy with C-arm at 0 degree is used to gauge the depth of puncture.
The prototype was developed by first testing on a gelatin model to optimize accuracy. (See Table 1 for variables tested and results). We developed our system to perform autoalignment within 15s with less than 2mm margin of error.
Results of gelatin model experiment to determine accuracy and speed of automation
We then performed trials in a live pig. We compared the results of percutaneous punctures using ANT-X with free-hand punctures performed by a fellowship-trained surgeon. Data on fluoroscopic time, radiation dose, puncture time and total time for procedure were recorded for each of the five attempts for robot-assisted and free-hand punctures. The results are discussed in the next section.
With the success of the animal trial, we performed our first attempt on a human subject using the ANT-X system in Myanmar after obtaining ethics approval from the Myanmar Medical Association.
Our patient is a 48 year-old gentleman who had a 1.4cm left lower pole renal stone with mild hydronephrosis. We performed the PCNL as per standard but with the ANT-X system to aid the alignment of our puncture. We report the results in the next section.
Results
A total of 10 procedures were performed on the single porcine model: 5 robot-assisted punctures and 5 unassisted with results as shown in Table 2.
Results of robot-assisted punctures vs free-hand technique in a live porcine model
Overall, there was comparable procedural time for both robot-assisted and free-hand punctures (3.15min vs 3.01min; p = 0.587) even though this included setting up the ANT-X equipment and auto-alignment timing.
The radiation exposure for robot-assisted arm during puncture was reduced by 26% as compared to the free-hand technique (8.2mGy vs 11.2mGy, p = 0.54). While this did not reach statistical significance, there may be clinically significant reductions in radiation. Further research may prove this potential benefit.
In the human trial, obtaining percutaneous access was successful at first attempt. Time to access (needle on skin to efflux of urine) was 3min 3s, out of which automated alignment by ANT-X took 32s. Patient was suspended from respiration for 40s. Total dose of X-ray for needle alignment and puncture was 3mGy over 45s. X-ray dose during the puncture was 1mGy over 20s. Efflux of urine was clear upon entry into the collecting system and patient had successful stone clearance.
Role in Endourology
In this report, we attempt to address the feasibility of the ANT-X system in attaining percutaneous renal access with this proof of concept study and its first successful human trial.
While a larger clinical trial is being planned to further assess the safety and benefits of this device, based on initial tests, ANT-X is a promising adjunct to PCNL.
ANT-X lessens the learning curve of percutaneous access as it reduces the need for surgeon's visualization of the calyceal system and the needle alignment. It also improves efficiency as there is less dependence on human skills during the procedure.
The improved accuracy can translate to decreased operative room (OR) time and fewer complications leading to shorter hospital stay and less need for additional treatment, thus, saving cost. Furthermore, if more urologists can use this device to perform PCNLs in a single setting, this will reduce the need for a separate procedure by radiologists to place percutaneous access, hence reducing healthcare cost from this additional radiological procedure.
While there is additional cost in the purchase of ANT-X and its maintenance, cost reductions from decreased OR time, complications, etc. are expected to outweigh the cost of using ANT-X.
Another benefit of ANT-X is that automated alignment can reduce the need for repeated fluoroscopy during targeting hence possibly reducing radiation exposure for both the patients and the healthcare team in the long run.
Lastly, ANT-X carries out automated needle targeting and positioning but ultimately, the puncture is still controlled by the surgeon whereas previously designed automated devices such as PAKY-RCM system, require the need to remotely control the needle trajectory. Hence, our device mimics closely a standard PCNL operation and it will be easier for urologists to adopt its use. ANT-X is also designed to be more compact and user-friendly with minimal device set-up.
However, as promising as ANT-X is, we acknowledge that the results are still too early for conclusion and there are some limitations of our device -
1. Respiratory movement during puncture
Kidneys movement during respiration makes targeting challenging. ANT-X is able to complete the alignment in less than 1minute of respiratory suspension. However, if any rib gets in the way of needle trajectory, requiring readjustment, respiration needs to be resumed and the process of alignment needs to be restarted, hence potentially prolonging overall surgical time.
2. Limited to prone technique with fluoroscopic imaging
In the recent years, some endourologists have been more interested in supine or ultrasound-guided punctures but our device is suited for prone PCNLs with fluoroscopic-guidance.
More work is underway to improve the device. While ANT-X is still being tested in its infancy, there are potential benefits that this device can contribute to the domain of endourology with its potential for a more efficient percutaneous access, making good outcomes reproducible and enabling more urologists to adopt PCNL.