
Abstract
Objectives:
To determine the accuracy of the surgeon's impression as to the stone-free rate at the end of percutaneous nephrolithotomy (PCNL), and to evaluate predictors for inaccurate estimation.
Materials and Methods:
A prospective study conducted between 2010 and 2015. Surgeon's impression, categorized as “insignificant residual fragments (RFs)” (<4 mm) or “significant RF” (>4 mm), was recorded at the end of PCNL, and was compared with postoperative imaging results, using CT or a combination of US and kidney, ureter, and bladder radiograph for radiolucent and radio-opaque stones, respectively. The association between missed significant RF and the patient and operative variables was evaluated with univariable and multivariable logistic regression analysis.
Results:
The study cohort included 312 patients. Significant RFs were found in 75 (24%) patients, comprising all 22 patients in whom RFs were suspected (100%) and 53 patients who were considered stone free (18.6%). The sensitivity, specificity, and positive and negative predictive value of the surgeon's estimation for the absence of significant RFs were 100%, 39%, 0.83, and 1 for radiopaque stones, and 100%, 12.5%, 0.75, and 1 for radiolucent stones. On multivariate analysis, multiple stones (OR = 4, 95% CI: 1.85–8.7, p < 0.001) and cumulative stone size (OR = 1.04, 95% CI: 1.02–1.1, p = 0.005) were independent predictors for missed RFs.
Conclusion:
In approximately fifth of the patients undergoing PCNL, the surgeon's impression of “insignificant RF” may be inaccurate. Stone size and number were independently associated with higher miss rate. These data should be shared with the patients when the postoperative drainage method and the option for an auxiliary procedure are discussed.
Introduction
P
The purpose of this study was to assess how accurate the surgeon's judgment (based on fluoroscopy and nephroscopy) is to the stone-free status at the end of PCNL and to find predictors for inaccurate estimation.
Patients and Methods
After obtaining approval from the institutional ethics committee, patients who underwent PCNL between January 2010 and July 2015 were included in this prospective study. The surgeon's impression of residual stones status was recorded immediately at the end of each procedure, and was categorized as “insignificant residual stones” (<4 mm), or “significant residual stones” (>4 mm). The following variables were also recorded: age, gender, BMI, stone side, number of stones and cumulative stone size, the presence of complete or partial staghorn stone, stone radiolucency and composition, the type of access (infracostal or supracostal), and operative time.
Two surgeons (D.L. and R.H.) performed all PCNLs. PCNL was performed as previously described. 9,10 After disintegration and removal of the main stone burden using rigid nephroscopy and ultrasonic lithotripsy, flexible nephroscopy is routinely performed. Contrast is injected in an antegrade manner to delineate the anatomy of the collecting system, and to ensure the inspection of each calix. Finally, if the ureter is capacious, proximal antegrade ureteroscopy is performed with the nephroscope. Otherwise, contrast is injected down to the ureter to rule out any filling defects. At the end of the procedure, all patients received a nephrostomy tube, a ureteral stent, or both.
Stone-free status was assessed before discharge by abdominal kidney, ureter, and bladder radiograph (KUB) in patients with radiopaque stones, or by CT for radiolucent stones, as determined by the surgeon. Treatment options were discussed with every patient who was found to have significant residual stones and a decision for conservative treatment or a secondary procedure was taken according to the patient's preference.
All the postoperative imaging studies were reviewed by a senior radiologist (A.C.) blinded to the patient data. Maximal size of an individual residual fragment (RF) was determined by measuring the diameter of the largest RF. The study's primary endpoint was missed significant stones, defined as an RF larger than 4 mm.
Statistical Analysis
Continuous variables were described as median and interquartile range. Categorical variables were described as number and percent. Because of the higher sensitivity of noncontrast computed tomography (NCCT) to detect small fragments compared to a KUB, the sensitivity, specificity, and positive and negative predictive value of the surgeon to detect residual stones were calculated separately for radiopaque and radiolucent stones. The association between missed significant stones ≥4 mm and the patient and operative variables was evaluated with univariable and multivariable logistic regressions, from which patients in whom the surgeon's impression was of significant RFs were excluded. All statistical analyses were two sided. Data were analyzed with SPSS Statistics, version 21.0 (IBM Corp., Armonk, NY). A p-value <0.05 was considered statistically significant.
Results
Three hundred and twelve patients underwent PCNL during the study period. Patient and operative characteristics stratified by RF status are summarized in Table 1. The study group included 290 patients who were categorized by the surgeon at the end of the procedure as “no or insignificant residual fragments,” and 22 (7%) patients categorized as “significant residual fragments.” Postoperative imaging studies revealed that 75 (24%) patients had an RF >4 mm; these included all the patients in whom RFs were suspected and 53 (18.2%) patients who were considered stone free at the end of PCNL. Figure 1 shows a flowchart of the study cohort. The sensitivity, specificity, and positive and negative predictive value of the surgeon's estimation for the absence of significant RFs were 100%, 39%, 0.83, and 1 for radiopaque stones, and 100%, 12.5%, 0.75, and 1 for radiolucent stones, using KUB and CT for postoperative imaging, respectively, as shown in Table 2.
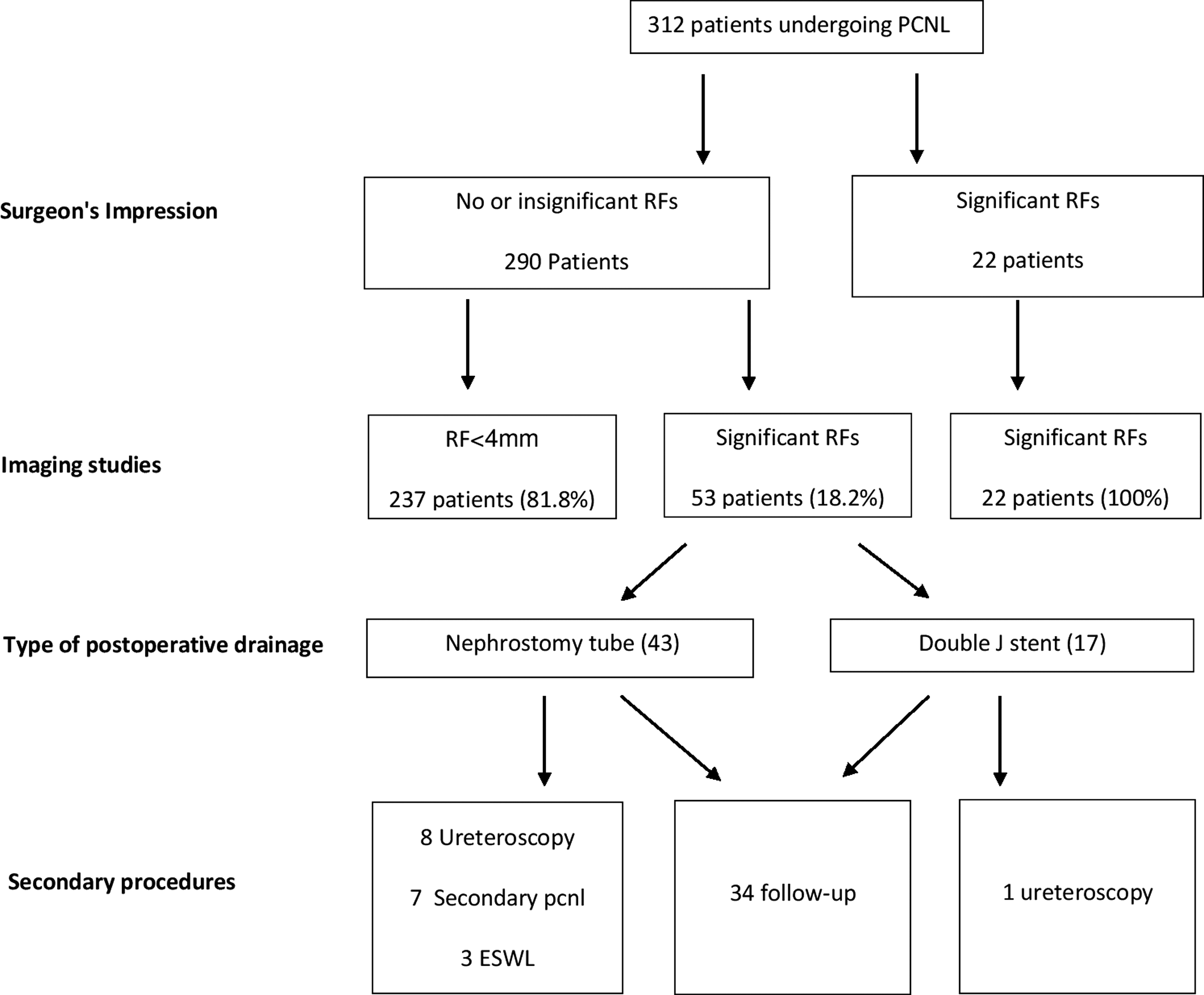
A flowchart of the study cohort.
PPV = positive predictive value; NPV = negative predictive value.
IQR = interquartile range; BMI = body mass index.
On univariate logistic regression analysis, using a p-value of 0.004 to account for multiple testing, multiple stones (OR = 4.83, 95% CI: 2.1–6.37, p < 0.001), cumulative stone size (OR = 1.07, 95% CI: 1.04–1.11, p < 0.001), and operative time (OR = 1.02, 95% CI: 1.01–1.025, p < 0.001) were associated with significant residual stones. On multivariate logistic regression analysis adjusted for these variables, only multiple stones (OR = 4.95, 95% CI: 2.52–9.71, p < 0.001) and cumulative stone size (OR = 1.07, 95% CI: 1.03–1.11, p = 0.005) remained significant predictors for significant residual stones, whereas operative time (OR = 1.02, 95% CI: 1–1.02, p = 0.131) did not, as shown in Table 3.
Secondary procedures were performed in 19 (6.5%) patients, and included ureteroscopy (9 patients), secondary PCNL (7 patients), and SWL in 3 patients. Nephrostomy tube was present in 18 (8.7%) patients before the secondary intervention, whereas 1 patient (0.7%) had a stent (p = 0.005). Seventeen patients (89.4%) were stone free at the end of the secondary procedures. Median RF size in the remaining 34 patients who were kept on follow-up only, was 5 mm. 4,8
Discussion
In this study, we assessed the surgeon's estimation regarding the stone-free status at the end of PCNL, and evaluated predictors for inaccurate estimation. The positive predictive value for an accurate stone-free impression was 0.83 and 0.75 for radiopaque and radiolucent stones, respectively. Missed RFs were associated with larger stone burden and longer operative time.
The decision on whether to place a nephrostomy tube at the end of the PCNL depends on several factors, of which, perhaps the most important, is the surgeon's estimation of the presence or absence of RFs. Despite meticulous intraoperative evaluation with fluoroscopic imaging and nephroscopy, significant RFs are found in 12% to 60% of the patients after PCNL. 3,11,12 For the purpose of an informed preoperative consultation as to the pros and cons of alternative postoperative drainage methods and optional secondary procedures, the accuracy of the surgeon's impression in determining the stone-free status should be discussed. However, the data on which this discussion is based are limited. Portis and colleagues performed a prospective study on 39 renal units undergoing PCNL. After endoscopic inspection, RFs larger than 2 mm were found in 9 of 34 (26.5%) cases who were considered stone free. 13 In a larger study of 236 patients, in whom the surgeons reported no residual stones, 66 (28%) patients had RFs as detected by postoperative CT. However, flexible nephroscopy was not utilized in this study. 14 This study group is the largest series assessing the surgeon's judgment as to the stone-free status at the end of PCNL based on fluoroscopy and extensive nephroscopy. We found that in nearly fifth of the patients in whom the surgeon assumed that a stone-free status was achieved, significant fragments were detected. The negative predictive value of surgeon's estimation for the absence of RF was 1, similar to other studies, reporting a sensitivity and positive predictive value of 97.1% and 0.93 for the presence of RFs. 14 Therefore, the surgeon's estimation is incredibly accurate in predicting the presence of residual stones, rather than their absence, and should be regarded accordingly.
The cutoff for RFs is noteworthy, as there is no clear definition for what would be considered “clinically insignificant stone fragments (CIRF).” In fact, many CIRF may not be as insignificant as we would like to believe. Streem and colleagues 15 were among the first to show that more than 40% of patients with RF <5 mm after SWL became symptomatic or required intervention when followed for an average of 26 months. Likewise, in a more recent study, Raman and colleagues 16 followed 42 patients with RF after PCNL. During a median follow-up of 41 months, 18 patients (43%) experienced a stone-related event, 11 of which required a secondary surgical procedure. They indicated that fragments as small as 2 mm can result in stone-related events. When treating infected stones, any RF should be removed, regardless of its size, as it was estimated that the risk for stone recurrence is almost quadrupled when RFs are present. 17 Thus, any remaining RF merits a discussion with the patient as to the pros and cons of follow-up vs auxiliary procedure.
The method to measure RF also deserves a comment, as one may argue that cumulative size of all fragments is more important than maximal size of a single one. Indeed, several studies have noted that even the presence of small, “insignificant” residual stones increases the rate of stone formation after SWL or PCNL, but are not associated with complications or reintervention. 18 –20 It is our opinion that RFs pose a bigger concern if they are unlikely to pass spontaneously, as reflected by their individual size.
In which patients is the surgeon more likely to miss an RF? Our results confirm the intuitive thinking that with increasing stone burden and number, the likelihood of a missed RF is higher. For example, among 47 patients with one or two stones smaller than 20 mm, only 1 (2.1%) patient had a missed RF, whereas 29 of 89 (32.6%) patients with five stones or more, and 15 of 62 (24.2%) patients with stone size >30 mm, had significant RFs. Multivariate analysis showed that higher cumulative stone size and the number of stones are independent predictors for missing RF. Operative time was associated with a missed RF on univariate, but not on multivariate analysis, possibly, since operative time is a surrogate for stone burden and complexity. However, it may also be affected by body habitus, accurate access positioning, surgeon's experience, collecting system configuration, and intraoperative bleeding, which in turn, may actually increase the risk for RFs. Upper pole access was associated with a missed RF with a p-value of 0.04, but it was not statistically significant when a corrected p-value was used. Similarly to operative time, the decision to perform upper pole access may indicate that a larger stone burden has been treated, and statistically, may result from collinearity with stone size. Furthermore, it is generally acceptable that upper pole approach allows better stone clearance, and therefore, it is unlikely to decrease the SFR. 12,17 Finally, stone composition, as well as radiolucency, were not associated with the remaining RF, probably attributable to the small number of patients within this group, but also, owing to our systematic utilization of flexible nephroscopy and mapping of the collecting system to ensure that all calices were inspected, thus, possibly eliminating the role of fluoroscopy in detecting stones.
The practical conclusion from these results is that placing a nephrostomy tube in patients with a large stone burden is a better alternative than a tubeless approach as it would allow a secondary PCNL if required.
Our study is not without limitation. First, the postoperative imaging modality is suboptimal as many small RFs are not detected with KUB. However, the sensitivity of KUB for the detection of clinically significant RFs is 85.7% in comparison to CT, and, accounting for the reduced radiation exposure, the combination of KUB and ultrasound is in real-life practice. 18 Finally, we did not incorporate in our prospective data base a stone score such as the Guy's score, 19 which could also be incorporated as a predictor for missed RFs. However, we can probably assume that with a higher grade score, the chances of missed RFs are higher and in fact, the ratio of tubeless PCNL in these patients is significantly lower. 20
Conclusion
In approximately fifth of the patients undergoing PCNL, the surgeon's impression of “insignificant residual fragments” may be inaccurate, whereas the surgeon's impression of significant RFs is highly predictive. Stone size and number are associated with inaccurate estimation, and these data should be discussed preoperatively with the patient in the context of postoperative drainage method and the option for an auxiliary procedure.
Footnotes
Author Disclosure Statement
No competing financial interests exist.