
Abstract
Purpose:
Ultrasound (US) guidance during renal access and mass biopsy reduces radiation exposure, but can be technically challenging. A needle guidance system might simplify these procedures. The purpose of this randomized crossover trial was to compare conventional and computer-assisted US needle guidance systems for renal access and mass biopsy.
Materials and Methods:
Seventy-one subjects were randomized to perform renal access or mass biopsy on a phantom using conventional and computer-assisted US guidance in a crossover study design. The primary outcome was success rate including subgroup analysis by experience level. Secondary outcomes included total procedure time, time to hit target, number of course corrections, and total punctures. In addition, subjective preferences of participants were also collected.
Results:
Procedure success rate was higher with the computer-assisted US than with conventional US for both novice (98.0% (48/49) vs 81.6% (40/49); p < 0.001) and experienced US users (100% (22/22) vs 81.8% (18/22); p < 0.001). Computer-assisted US significantly shortened the total procedure time (94.0 seconds vs 192.9 seconds; p ≤ 0.001), time required to hit the target (62.5 seconds vs 121.6 seconds; p ≤ 0.001), and the number of course corrections (0.56 vs 2.89; p < 0.001) compared with conventional US. Computer-assisted US did not significantly reduce the number of needle punctures (1.75 vs 2.39; p = 0.132). Seventy-three percent of subjects preferred the computer-assisted US system.
Conclusion:
A computer-assisted needle guidance system increases effective US targeting for renal access and mass biopsy for novice and experienced users.
Introduction
I
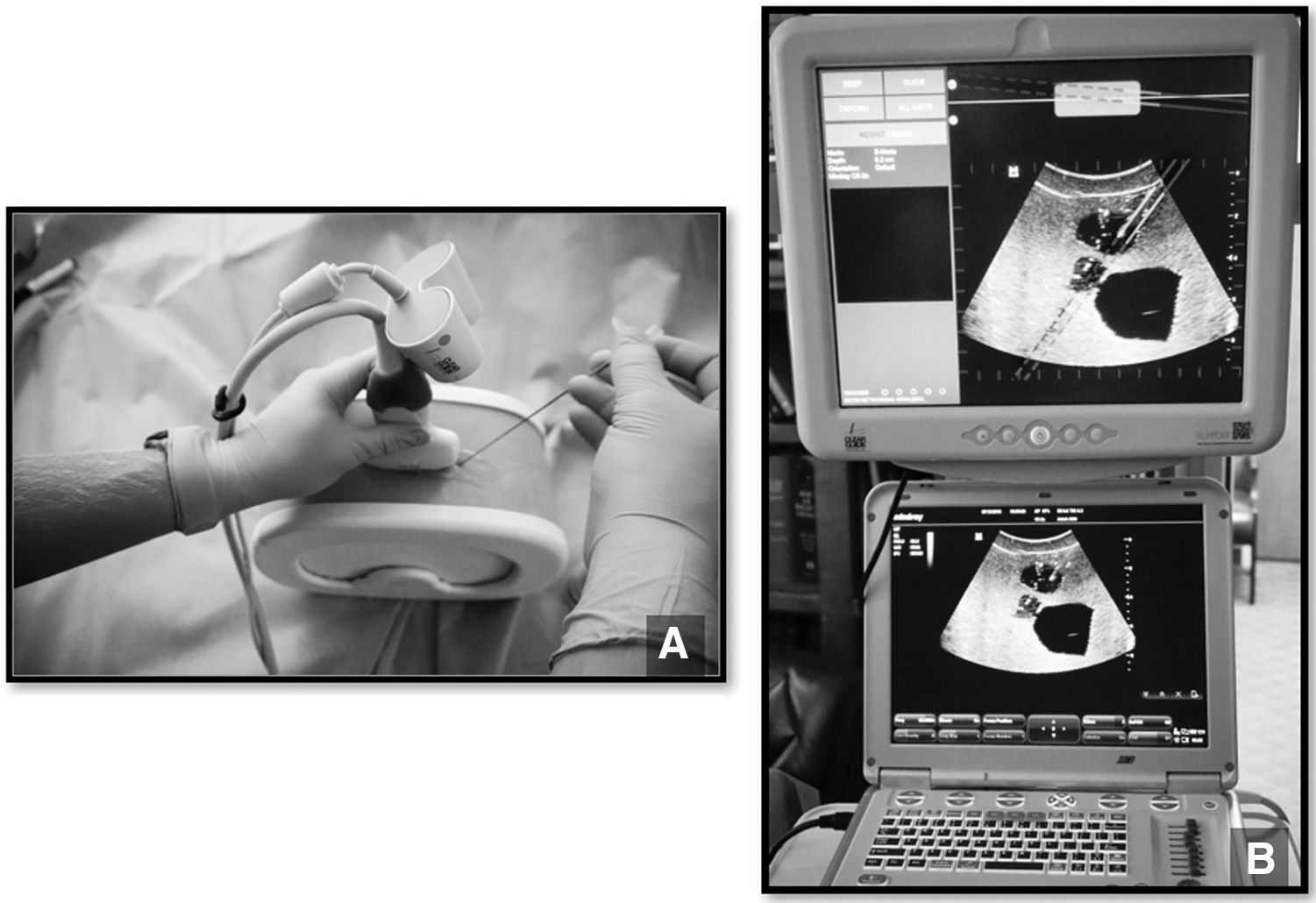
To facilitate the adoption of US, electromagnetic (EM) guidance has been developed, which improves needle accuracy, decreases the number of needle sticks, and assists novice learning compared with conventional US. EM guidance, however, requires special needles, external sensors, and/or unique US machines. 11 –13 An alternative to EM guidance is a novel computer-assisted stereoscopic camera system that attaches to the US probe and displays the needle trajectory on the US monitor (Fig. 1A, B). This computer-assisted camera works with any US system and needle combination. 13 The dual lens camera optically tracks the external portion of the needle and projects the internal trajectory of the needle on a real-time US image.
The purpose of this randomized controlled trial was to compare conventional US and computer-assisted US guidance for renal access and mass biopsy. We hypothesize that computer-assisted US can improve the ease of use, accuracy, and functionality of US-guided procedures.
Materials and Methods
Seventy-one subjects were enrolled in this IRB-approved study over a 3-day period during an Ultrafest event at Loma Linda University. Each subject attempted a needle-guided procedure using both a conventional US system and a computer-assisted US system in a randomized manner. Before initiation of the study, all subjects were oriented with a standardized 3-minute training with both modalities followed by 3 minutes of practice. After training, each subject was randomized through a random number generator to begin with one modality, targeting a specific structure in his or her assigned phantom (Computerized Imaging Reference Systems [CIRS], Norfolk, VA). After completing the trial using one US modality, participants were crossed over to the other modality and attempted to target the same structure (Fig. 2).
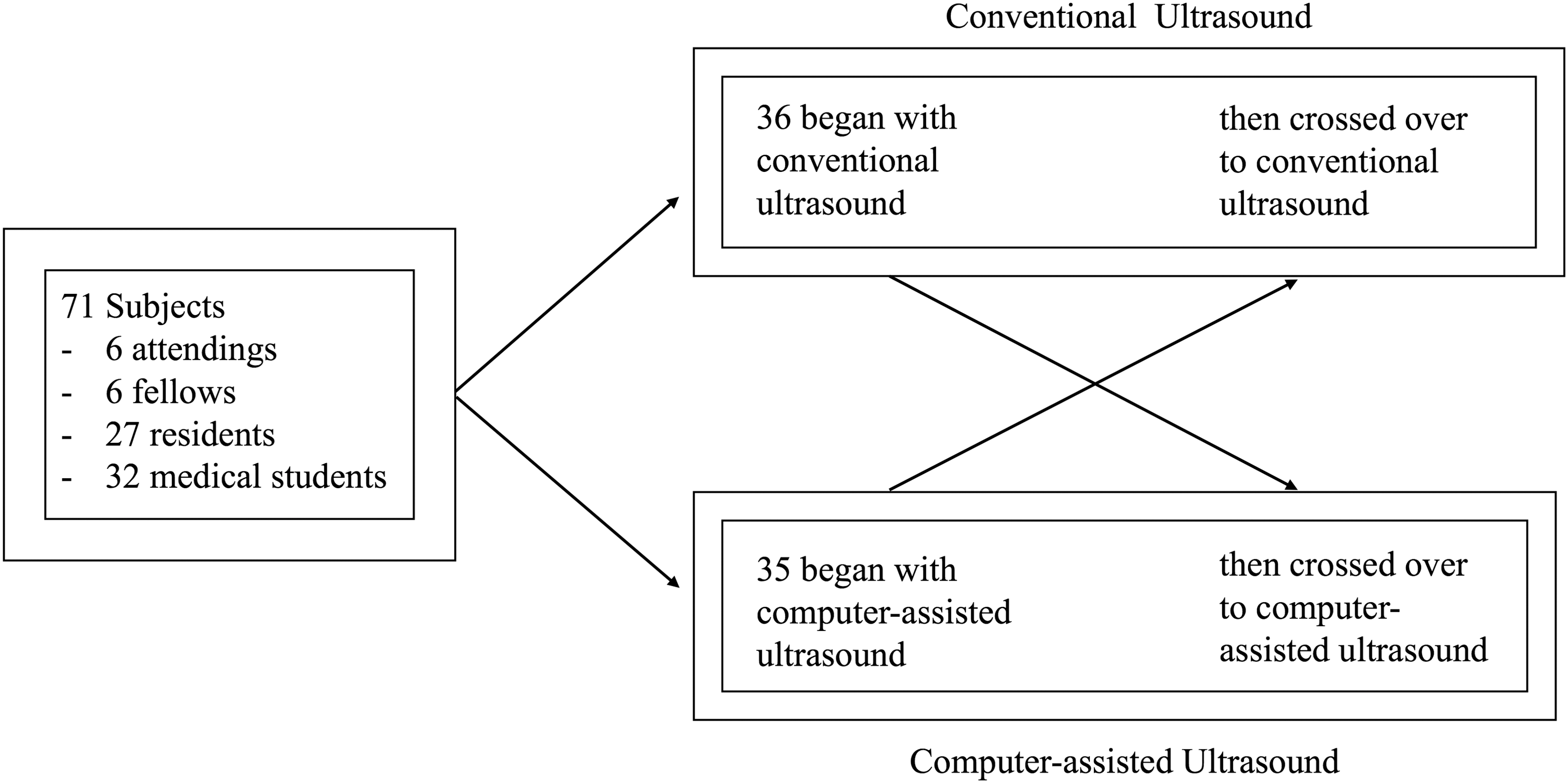
Methods flowchart.
The target within the first phantom was a mass at a depth of 5.9 cm (Fig. 3A). The target in the second phantom was a model renal calix at a depth of 6.3 cm (Fig. 3B). Subjects used a generic 17-gauge, 152 mm needle with 1 cm demarcations. The computer-assisted system used in this study included a dual lens camera and core processing unit (Clear Guide ONE; Clear Guide Medical, Baltimore, MD) connected to a curved array transducer probe at 5 MHz and a Mindray M7 portable US unit (Mindray Medical International Limited, Mahwah, NJ). Conventional needle guidance utilized either the Mindray US or a SonoSite Edge II US with a curved array transducer probe at 5 MHz (Fujifilm SonoSite, Inc., Bothwell, WA).
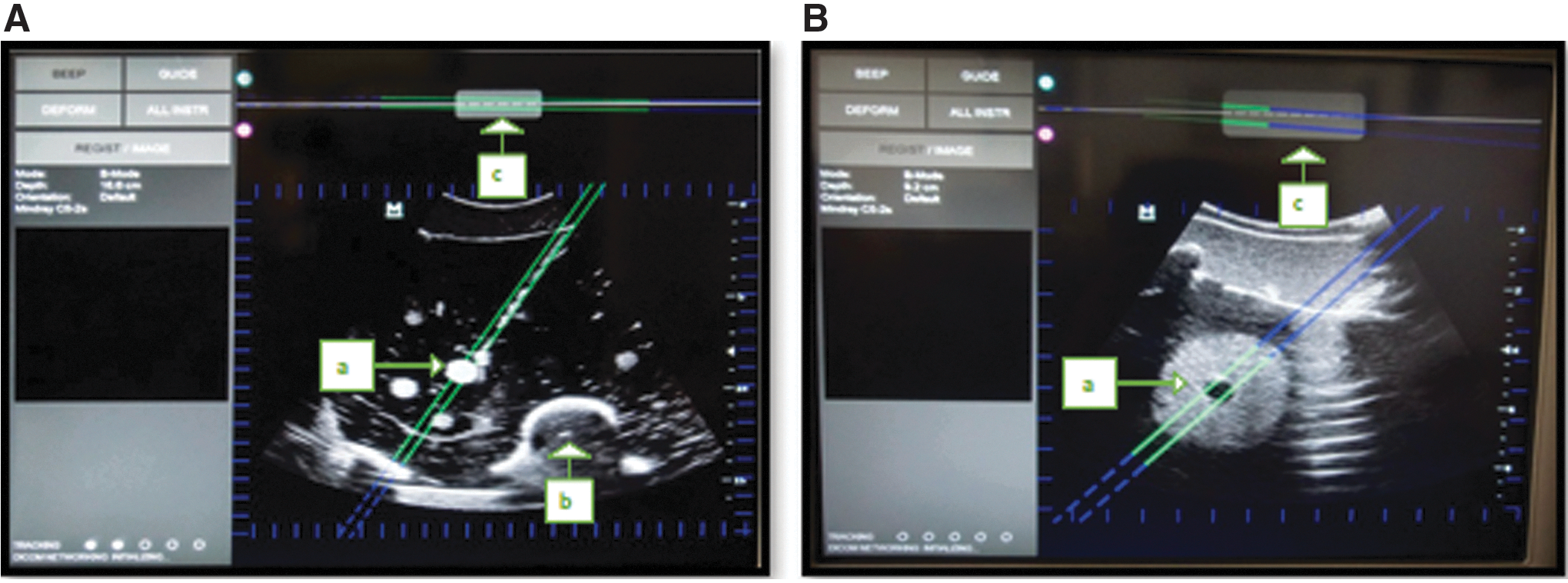
The computer-assisted US functions by overlaying guidance lines on the real-time US image. The guidance lines change color to indicate the position of the needle. Green lines indicate that the needle is projected to pass through the plane of the US beam, whereas blue lines project the needle's path outside of the beam. A figure at the top of the screen represents a top-down view of the US probe and the needle's projection in relation to it (Fig. 3).
Effective penetration of the target was determined by an objective observer through a clear plastic window in the phantom that was covered during subject trials. The primary endpoint was success rate in reaching the target within 5 minutes. Trials lasting more than 5 minutes were recorded as failures. Secondary endpoints included total procedure time, time to hit the target, number of course corrections, and number of needle punctures.
Additional subgroup analysis by experience level was performed. An effective trial was defined as penetrating the designated target within 5 minutes of US probe contact. Total time was calculated from US probe contact with the phantom until reaching the target. Time to hit the target was recorded from skin puncture until target penetration. A course correction was reported if the needle was backed out more than 1 cm to adjust the angle of penetration. Additional punctures were defined as complete removal of the needle from the phantom and subsequent reinsertion.
Demographics of participants and their preferences between the two US modalities were collected. Subjects were further divided according to US exposure into experienced (>20 procedures) and novice practitioners (≤20 procedures). 10 Continuous and categorical variables were analyzed using the IBM SPSS software (Version 22, Armonk, NY), with p < 0.05 considered significant, employing the paired Student's t-test and the chi-square test, respectively.
Results
Of the 71 subjects, 6 were attending physicians, 6 were fellows, 27 were residents, and 32 were medical students. Thirty-six subjects started their trial with conventional US, whereas 35 started with the computer-assisted US system. Each of the 71 subjects performed 2 trials, 1 trial with each US modality, for a total of 142 trials (Fig. 2). Ninety-two trials were conducted on the mass biopsy phantom and 50 trials were conducted on the renal access phantom.
The overall success rate was significantly higher with computer-assisted US than with conventional US (98.6% (70/71) vs 81.7% (58/71); p < 0.001). The 13 subjects who failed included 4 medical students, 7 residents, and 2 fellows. The success rate was significantly higher with computer-assisted US than with conventional US for both novice (98.0% (48/49) vs 81.6% (40/49); p < 0.001) and experienced US users (100% (22/22) vs 81.8% (18/22); p < 0.001), respectively (Table 1).
Bold type indicates statistically significant variables.
US = ultrasound.
Mass biopsy phantom
There was no significant difference in the success rate on the mass biopsy phantom between computer-assisted US and conventional US (100% (46/46) vs 95.7% (44/46); p = 0.151) (Table 2). The mean total time was similar for both US modalities (74.5 seconds vs 93.7 seconds; p = 0.102). However, the mean time to hit the target was significantly shorter for computer-assisted US (47.0 seconds vs 89.4 seconds; p < 0.001). The computer-assisted US system also resulted in fewer course corrections (0.52 vs 2.78; p < 0.001). There was no significant difference in the mean number of punctures to hit the target between computer-assisted and conventional US trials (1.76 vs 2.54; p = 0.154).
Bold type indicates statistically significant variables.
Total time for novice and experienced practitioners was also compared.
Renal access
The success rate of trials using the renal access phantom was significantly greater using computer-assisted US than using conventional US (96% (24/25) vs 56% (14/25); p < 0.001) (Table 2). The mean total time (114.6 seconds vs 179.5 seconds; p = 0.020) and time to hit the target (78.1 seconds vs 175.9 seconds; p = 0.001) were significantly faster for participants using computer-assisted US. The number of course corrections was also significantly lower for computer-assisted US than for conventional US (0.40 vs 3.36; p = 0.001). There was no significant difference in the number of punctures between the two US modalities (1.64 vs 1.76; p = 0.622).
Combined data set
Pooled data from both phantoms showed that computer-assisted US significantly shortened the total procedure time (94.0 seconds vs 192.9 seconds; p ≤ 0.001) and the time required to hit the target (62.5 seconds vs 121.6 seconds; p ≤ 0.001) compared with conventional US. Computer-assisted US also significantly reduced the number of course corrections needed compared with conventional US (0.56 vs 2.89; p < 0.001). There was no significance when comparing the number of punctures (1.75 vs 2.39; p = 0.132) between the two US modalities (Table 2).
Novice subjects were significantly faster with computer-assisted US than with conventional US in both total time (76.0 seconds vs 198.7 seconds; p < 0.001) and time to hit the target (50.7 seconds vs 124.5 seconds; p < 0.001). Experienced subjects trended toward lower total time using computer-assisted US (125.7 seconds vs 165.9 seconds; p = 0.087) (Table 2). However, their time to hit the target was similar to that of conventional US (83.5 seconds vs 107.9 seconds; p = 0.282). Computer-assisted US use significantly reduced the number of course corrections compared with conventional US use in both novice (0.62 vs 3.62; p ≤ 0.001) and experienced US users (0.45 vs 1.91; p = 0.007). The number of punctures trended toward a reduction with computer-assisted vs conventional US in novices (1.79 vs 2.92; p = 0.081), but was similar in experienced users (1.77 v. 1.54; p = 0.381).
Overall, 73.2% (52/71) of participants preferred computer-assisted US needle guidance to conventional US. Novice subjects overwhelmingly preferred the computer-assisted US system to conventional US (92% (45/49) to 8% (4/49)). Although most experienced practitioners (68% (15/22)) preferred conventional US, 32% (7/22) stated that they preferred the computer-assisted US system.
Discussion
The most common applications in urology that could benefit from percutaneous US needle guidance include renal access for PCNL and mass biopsy. As the incidence of nephrolithiasis increases globally and in the United States, radiation exposure for patients also increases. Patients with large stones receive radiation exposure during diagnosis because of CT imaging, during treatment from fluoroscopy, and during imaging employed for follow-up. 14,15 In addition, the urologic surgeon and operating room staff also experience potential risks from radiation as the caseload of PCNLs is increasing. 16
US guidance has been recommended as one strategy for decreasing the radiation exposure during renal access. 17 However, conventional US-directed renal access has not been widely embraced by urologists in the United States because of a steep learning curve. 17,18 One unique challenge limiting the adoption of US-guided renal access is difficulty in observing the needle tip, particularly when out of plane. Failure to accurately observe the needle tip risks over-advancement of the needle and injury to surrounding structures. 19
Currently, only 11% to 27% of urologists acquire their own renal access during PCNL. 20,21 The explanation for this low percentage is multifactorial, including the technical complexity of the procedure and the limited number of PCNLs performed by most urologists. These factors prevent them from ascending the learning curve that can result in increased operative time associated with obtaining the access. Furthermore, reimbursements do not typically compensate surgeons adequately for the additional operative time. 18 Despite its inherent challenges, US has been effectively employed by skilled surgeons for renal access during PCNL, and US use may only add a few minutes to the operative time. 6,8,22 Our results indicate that a computer-assisted needle tracking device reduces the time required for renal access, potentially reducing the learning curve and motivating urologists with less US experience to obtain their own renal access during PCNLs. 18
Renal mass biopsy is commonly performed by interventional radiology under US or CT guidance. Urologists have typically played a limited role in this because of lack of familiarity with US or lack of access to real-time CT. Mass biopsy was not historically favored for diagnosing small renal masses, given its low negative predictive value and potential for complications such as hemorrhage or pneumothorax. 23 However, more recent guidelines have suggested more frequent use of biopsy when assessing renal masses, given its improved predictive value, and its use has expanded to about 30% of patients diagnosed with renal cell carcinoma in recent years. 24
US guidance has been recommended instead of CT because of decreased risk of vascular injury and eliminating exposure to radiation, similar to the benefits derived from using US in PCNL. 25 A computer-assisted US needle guidance system could improve targeting accuracy and reduce failure rate.
The benefits of conventional US are primarily realized by experienced users because of the learning curve in recognizing relevant anatomy while maintaining observation of the needle. 26 A computer-assisted US system expands these benefits to novice users by tracking and displaying the needle's position even when the needle is out of the US plane. Computer-assisted US has already shown promise in other disciplines such as anesthesia and emergency medicine. 27 –29
This is the first study to show that a computer-assisted system can aid both novice and experienced US practitioners in renal access and mass biopsy. While decreasing the time needed for novice subjects to hit a target, this computer-assisted system also leads to shorter needle penetration times and fewer course corrections. Finer needle control may potentially reduce the risk of damaging nearby vasculature and organs during a PCNL or mass biopsy. 17,25,30 However, these potential advantages would need to be confirmed in either an animal model or future clinical trials.
The majority (92% (45/49)) of novice users preferred computer-assisted US. Although experienced users preferred conventional US (68% (15/22)), one-third of experienced users (32% (7/22)) still found computer-assisted US preferable to conventional US and experienced users also had a higher success rate when using the computer-assisted system. With increased exposure to the computer-assisted US system, its potential benefits may become more apparent and the number of physicians preferring it may increase.
There are currently several other tracking systems available to aid in US-guided access that have shown efficacy in reducing radiation during urologic procedures. Lima and colleagues employed an EM needle guidance system for US in 10 patients and effectively obtained renal access on their first attempt without X-ray exposure. 31 Li and colleagues found that EM needle guidance significantly shortened the time for effective renal puncture, enabled fewer puncture attempts, and reduced complications during PCNL. 30,32
Although our study reports similar benefits, the computer-assisted system studied here has several advantages over an EM paradigm. 30 EM systems are complex, have a long setup time, and require specialized equipment including a dedicated US machine. 13 In contrast, this computer-assisted system is ergonomic and flexible. The camera occupies minimal space on the US probe (Fig. 1A, B) and does not require an external transmitter arm, making a complicated PCNL operating room environment easier to navigate. A one-time calibration also means that no additional time is wasted with setup after the first use. The stereoscopic camera attaches to any US machine and captures most needles, unlike the specialized machine and needles required for EM systems. This may make the computer-assisted system a more affordable and flexible alternative, with the commercial list price of $29,500 for a computer and probe attachment that can be added to any existing US system.
One limitation to our study was the fact that simulated ribs and vertebrae in the renal access phantom made needle guidance more difficult when compared with the mass biopsy phantom, which had no simulated ribs and was, therefore, a simpler model. This was addressed by having each subject use only one phantom for the entirety of the experiment, subsequently acting as his or her own control. With an improved renal access simulation and a larger population, we speculate that differences between conventional and stereoscopic needle guidance would become more apparent. Even so, the phantom still demonstrated that the computer-assisted system resulted in significantly fewer failures than did conventional needle guidance.
Our model was designed to replicate mass biopsy and renal access in the operating room where respirations can be suspended. As such, the models did not incorporate respiratory excursion or lungs. These factors could be tested in future studies. In addition, the use of US is limited in obese patients, and this represents one further barrier to adoption of US technology in the United States, where obesity rates are currently 36.5%. 33
Another limitation of the computer-assisted US system is that needles smaller than 20-gauge may deflect inside the patient creating a discrepancy between the projected and actual needle path. Trajectory mapping is also less accurate if the camera's view of the needle is obstructed, for example, by fingers on the needle shaft or fluid on the camera's sterile cover. In addition, the stereoscopic system is a two-dimensional solution to a three-dimensional (3D) problem. Although the computer overlay does contribute information regarding the z-axis using solid and dotted lines, it is not a 3D solution (Fig. 3). A final limitation is that many subjects lacked experience with one or both of the US modalities and only had 3 minutes of training followed by 3 minutes of practice time before the trials began. However, this allowed us to assess how rapidly these skills could be acquired by novice US practitioners.
Conclusion
This computer-assisted stereoscopic US needle guidance system significantly increased success rates for both novice and experienced US users. It also decreased total procedure time, time to hit the target, and number of course corrections. Novice users overwhelming preferred computer-assisted US as well as one-third of experienced users. Further analysis of the potential benefits of computer-assisted US needle guidance would be beneficial and may increase the use of US by urologists for renal mass biopsy or PCNL access.
Footnotes
Author Disclosure Statement
Clear Guide Medical provided a demonstration model of the product for use during the trial but provided no funding or compensation.