
Abstract
Objective:
To evaluate the clinical value of endoscopic fibrin glue (FG) application therapy in treating hemorrhagic radiation cystitis (HRC).
Patients and Methods:
This is a single-cohort, prospective pilot study. We collected data from patients with HRC who were treated at our urology unit from May 2014 to December 2016. Patients with grade ≥2 HRC for whom conventional therapy and transurethral endoscopic electrocoagulation had failed were treated with endoscopic intravesical FG. The mean follow-up was 26.2 ± 9.78 months. Our analysis included data on patient demographics, pelvic malignancies, radiotherapy regimens, total dose of radiation received, time of onset and severity of hematuria, and previous intravesical management. Following FG intervention, patients' clinical status was defined as: (1) clinical response; absence of dysuria, urgency, and frequency; discontinuation of analgesic medication; and Foley catheter removal, but with ongoing hematuria grade <2; (2) complete response, clinical response, and no further hematuria; or (3) no response, no clinical response, and sustained hematuria.
Results:
A total of 20 patients (12 women and 8 men; mean age, 69 ± 7.5 years) were treated with 12 mL FG intravesically, using endoscopic application. Of the 20 patients, 16 (80%) had a complete response and 4 (20%) had a clinical response. In the case of four patients (20%), treatment was carried out twice. Mean hospital stay was 6 ± 2.5 days. The intervention showed good tolerability in all patients. No major adverse events were reported. Bladder spasms were the only minor adverse events reported in six patients (30%).
Conclusion:
Application of FG is an effective, practical, affordable, and repeatable procedure for the treatment of grade ≥2 HRC.
Introduction
Hemorrhagic cystitis (HC) could be defined by the presence of hematuria and lower urinary tract symptoms (mainly filling phase symptoms and dysuria) and is one of the most challenging clinical entities in urology. 1 Hemorrhagic radiation cystitis (HRC) has been described as a complication of pelvic tumor radiation therapy. Radiation cystitis incidence may vary from 23% to 80%, due to different types and doses of radiation therapy among different medical subspecialties. 2 Radiation cystitis generally develops after a mean of 31.8 months after radiotherapy and the male:female ratio is 2.8:1, due to the radiotherapy treatment for prostate cancer. 3 Hematuria is often the first symptom, varying from a mild to a severe life-threatening condition.
Following an American Urological Association (AUA) Update Series, the initial management of HC includes hyperhydration, blood transfusion if needed, transurethral three-way catheterization, and continuous bladder irrigation. 4 For persistent bleeding, no standardized therapy has been established as a gold standard. Currently, the AUA and the European Association of Urology (EAU) do not provide any specific guidelines for the treatment of radiation cystitis.
In 2002, Shekarriz and Stoller analyzed the application of fibrin glue (FG, or fibrin sealant) in urological surgery. Despite the need of further investigations, FG was considered a promising topical tool for controlling surface bleeding during urological procedures. 5 We previously demonstrated the efficacy and repeatability of FG, administered by endoscopic intravesical application, in the management of HC after allogeneic stem cell transplantation. 6
The FG is produced through an enzymatic reaction that converts patient-derived fibrinogen into fibrin I polymer, which is then administered endoscopically within the bladder leading to the activation of the final steps of the coagulation cascade. 7
Herein we have assessed the clinical value of endoscopic intravesical FG application in a single cohort of patients with refractory HRC.
Patients and Methods
HRC classification
HRC was classified using conventional published criteria into four grades: grade 1 (microscopic hematuria), grade 2 (macroscopic hematuria), grade 3 (hematuria with clots requiring blood transfusion support), and grade 4 (macroscopic hematuria with clots and impaired renal function). 8,9
Inclusion criteria
All patients with HRC were initially treated with conventional therapy that consisted of hyperhydration, catheterization, continuous bladder irrigation, transfusion if needed, and transurethral endoscopic electrocoagulation with clot evacuation. Patients who were eligible for FG application met the following criteria: (1) progression from grade 1 to grade ≥2 HRC following standard treatment, or (2) grade ≥2 HRC that was unresponsive to standard treatment (refractory HRC).
Patients
Patients treated with FG for HRC at our institution were enrolled (Table 1). Urine cultures was negative for all the patients. A pre-endoscopic treatment bladder ultrasound was performed to exclude the presence of macroscopic bladder malignancies and to assess the presence of signs of radiation cystitis such as clots, intravesical debris, and diffuse bladder wall thickening.
Patients and Clinical Characteristics
HRC = hemorrhagic radiation cystitis.
Our analysis included data on patient demographics; pelvic malignancies; radiotherapy regimens; total dose of radiation received; time of onset; severity of hematuria according to the European Organization for Research and Treatment of Cancer (EORTC) and the Radiation Therapy Oncology Group (RTOG) criteria 10 –12 ; time from onset of hematuria to FG application; and previous vesical management. The first episode of hematuria after radiotherapy was considered as its onset, regardless of its EORTC/RTOG grade. The timing of therapy (primary, adjuvant, or salvage treatment) and the total radiation dose delivered were analyzed independently.
Methods
Fibrin glue preparation
FG was derived from virus-inactivated fresh-frozen human plasma (Octaplas, Vienna, Austria) and produced using Vivostat System (Vivolution, Birkeroed, Denmark), an automated process that generates a vial of ∼6 mL from 120 mL of the patient's own fresh-frozen plasma (or whole blood) in about 30 minutes. For each application, we prepared 12 mL of FG. The procedure begins by drawing 120 mL of the patient's blood and separating platelet-depleted plasma from the blood sample. An enzymatic reaction converts fibrinogen from the plasma into fibrinopeptide A without activating factor XIII. This causes fibrin I polymer to be formed, which is then separated from the reacted serum and dissolved in a small amount of sodium acetate buffer (pH 4). A vial of purified fibrin I concentrate is then transferred to the applicator unit. The solution is administered to the patient at the same time as 1.0 mL of 0.75 mol/L carbonate/bicarbonate buffer (pH 10), which is delivered by a syringe within the applicator unit. During the application process, the two solutions are combined in a 7:1 ratio (fibrin I:pH 10 buffer). This creates a neutral pH, allowing the conversion of endogenous prothrombin to thrombin in the presence of calcium ions. In turn, the endogenous thrombin causes the formation of fibrin II from fibrin I through cleavage of fibrinopeptide B. The thrombin also activates endogenous factor XIII, which creates chemically stable cross-linkages within the acid-soluble fibrin II polymer to form a clinically useful fibrin sealant. 13 The FG instantly forms a gel that becomes more rigid with increasing polymerization and covalent cross-linking.
Fibrin glue: endoscopic technique
To identify the type and extent of mucosal lesions, and to carry out evacuation of clots, we initially performed conventional cystoscopy while patients were sedated and on oxygen ventilation. Following this initial endoscopic evaluation, the bladder was emptied and a 22F cystoscope was connected to a laparoscopic CO2 insufflator to ensure the bladder remained distended at a constant pressure of 12 mm Hg. The FG applicator was inserted through the lumen of the cystoscope, allowing 12 mL of glue to be sprayed directly onto the raw, bleeding surface of the bladder mucosa (Fig. 1). Use of CO2 insufflation during FG application avoids overflow and overdistension of the bladder. 6,14 The procedure generally lasts for about 30 minutes: FG application and spraying takes around 5–10 minutes for every 6 mL vial of FG, pneumo-cystoscopy lasts for about 5–10 minutes after glue application. Pneumo-cystoscopy is needed to temporarily prevent bleeding, provide a good vision, and permit to air-spray the glue, allowing the activation of coagulation cascade and cross-linking of fibrin polymers as well as avoiding an intraluminal downfall of a single clot. At the end of the procedure, a Foley catheter was inserted (without bladder irrigation) and removed once hematuria was no longer evident.
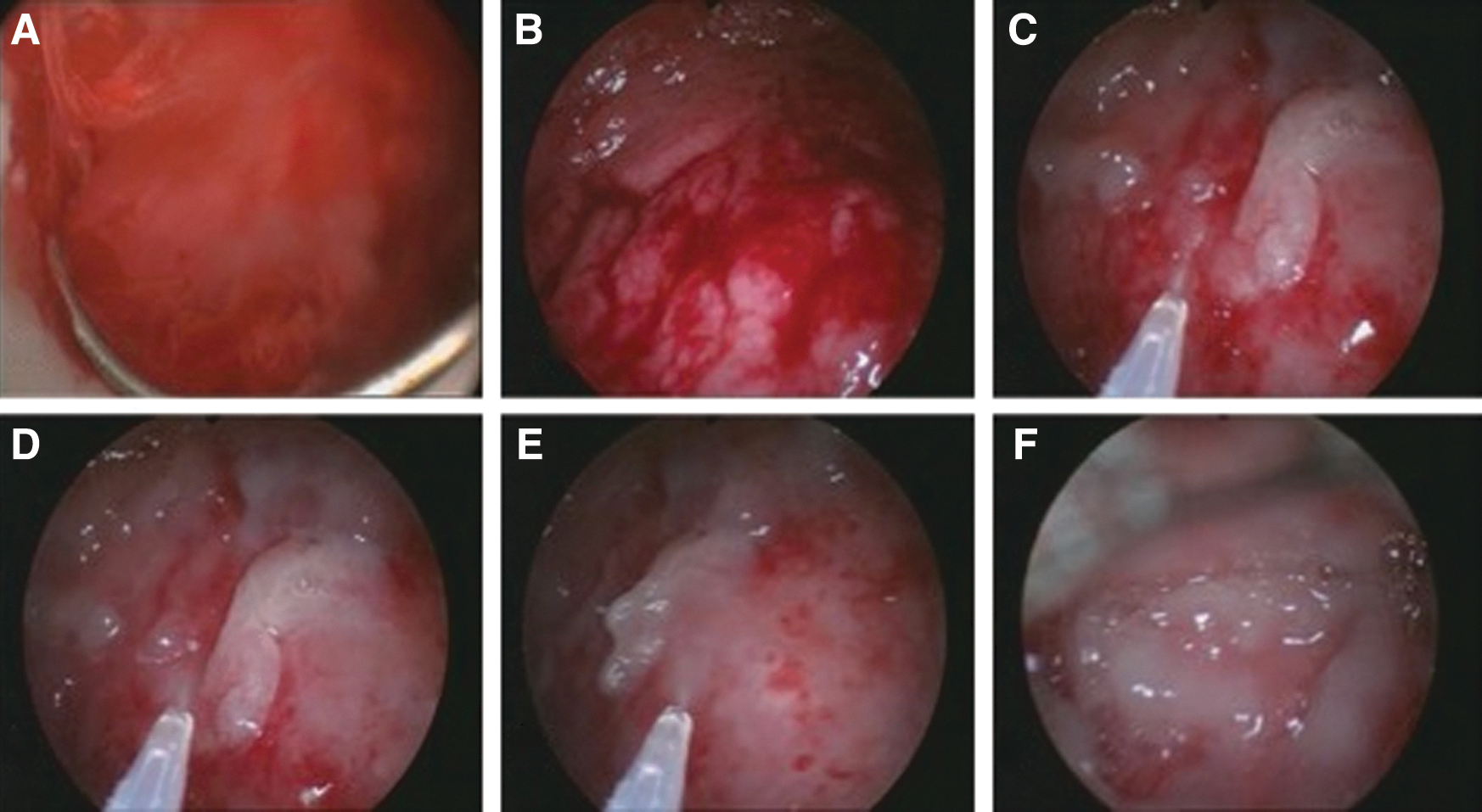
Cystoscopic images
Data were retrospectively reviewed. Continuous variables are presented as mean (standard deviation) if they were normally distributed; and as median if not normally distributed. Categorical variables are reported as number and percentage.
Response criteria
Each patient's response to FG application was defined as one of the following: (1) clinical response: absence of dysuria, urgency, and frequency; discontinuation of analgesic medication; and Foley catheter removal, but with ongoing hematuria grade <2; (2) complete response: clinical response and no further hematuria; or (3) no response: no clinical response, sustained hematuria. Blood count levels were checked at days 1, 3, and 7. Urine analysis was performed after 1 and 3 months. Post-treatment cystoscopy was not performed in patients with symptomatic improvement.
Results
From May 2014 to December 2016, we enrolled 20 patients (12 women and 8 men; mean age, 69 ± 7.5 years) who were treated with FG for HRC at our institution. HRC had developed as a result of prior radiotherapy for prostate cancer (n = 7; 35%), bladder cancer (n = 6; 30%), or a gynecological malignancy (n = 7; 35%). The mean dose of radiation was 60 ± 2.50 Gy. The mean time period from receiving radiotherapy to onset of HRC was 3 ± 1.9 years. The mean duration of hematuria was 3.5 ± 2.5 months.
Eighteen patients were hospitalized directly from the emergency room with a grade ≥2 HRC; two patients were transferred from another hospital after failure of conventional therapy. Twelve patients had a grade 2 HRC, and eight patients a grade 3 HRC. In eight patients (40%), hospitalization during which FG was utilized represented their first admission for HRC refractory to conventional therapy.
All patients had shown an inadequate response to conventional therapy with hyperhydration, catheterization, continuous bladder irrigation and transurethral endoscopic clot evacuation, hemostasis, and transurethral endoscopic electrocoagulation. Eight patients (40%) underwent multiple transfusions during conventional therapy. Hypogastric artery embolization was performed in two patients with unsuccessful results.
Overall, FG treatment was successful, with a complete response achieved in 16 patients (80%) and a clinical response achieved in 4 patients (20%). Four patients (20%) underwent the treatment twice with a second FG treatment after 3 (n = 2) and 4 days (n = 2), respectively. Following endoscopic intravesical FG application, no further HRC support therapy was given before hospital discharge. None of the patients required transfusion after FG application. The mean hemoglobin level before the procedure was 8.7 ± 0.5 g/dL; 1 week after the procedure, the mean hemoglobin level was 9.2 ± 0.4 g/dL (p < 0.05). The catheter was removed after 4 ± 1 days (grade ≤1 HRC). Mean hospital stay was 6 ± 2.5 days. The mean follow-up for the full cohort was 26.2 ± 9.78 months.
After FG endoscopic treatment, 6 patients (30%) had grade 1 HRC at the 30-day follow-up visit (microhematuria). None of them underwent hyperbaric oxygen (HBO) therapy or other treatments. At the 3-month follow-up visit, four patients had microhematuria (20%). They neither had relapse of a macroscopic hematuria (≥2) nor had anemia clinical signs during clinical oncology follow-up. One patient developed a cardiac valve prolapse and one developed a radiation-related bladder squamous cell carcinoma requiring cardiac surgery and radical cystectomy respectively.
The FG treatment showed promising tolerability in all patients. No major adverse event was reported. Bladder spasms were the only minor adverse events reported (six patients; 30%). None of the patients developed urinary tract infections (Table 2).
Results After Fibrin Glue Application
Clinical response: disappearance of dysuria, urgency, and frequency; analgesic agent discontinuation; and Foley catheter removal with persistence of hematuria grade <2, grade 2 hematuria, macroscopic hematuria; complete response: clinical response and absence of hematuria.
FG = fibrin glue.
Discussion
HRC is a progressive condition with high morbidity that could significantly affect the patient's quality of life. Radiotherapy leads to mucosal ischemia, epithelial damage, and ulcer formation that may cause pain and discomfort. 2 A total dose exceeding 60 Gy is highly toxic for the bladder. 3
This is the first case series on the use of FG in HRC. Our experience includes 20 patients with HRC refractory to standard therapies who underwent endoscopic FG intravesical application. Therapeutic utilization of FG was a complete success in 16 patients. In four patients, a clinical response was achieved. FG endoscopic application therapy combined with standard treatment is effective and safe in the management of HRC with a reduced incidence of gross and microhematuria during the follow-up of the full patient cohort. There were no reports of adverse events. Our results confirm the first reported experience of Ouwenga and colleagues on the use of fibrin sealant for refractory HRC with a successful outcome after failed conventional treatment, urinary diversion, formalin instillation, HBO, and multiple other treatment modalities. 15
Several treatment options have been reported for HRC in case reports or very small case series. Although the results reported in some cases have been encouraging, the number of patients treated have been low and the experience confined to a single center.
Browne and colleagues reviewed the management of RC, dividing treatments into systemic, interventional procedures, and intravesical. 16 Systemic treatments aim to enhance the protective polysaccharide layer to prevent later RC. Interventional procedures, considered as a last resort, include selective embolization or ligation of internal iliac arteries and urinary diversion. 17 Several agents have been administered intravesically, but high-quality evidence in their support is lacking. HBO therapy stimulates angiogenesis, reversing the vascular changes induced by ionizing radiation. 18 However, HBO therapy has limited effects in preventing further injuries once ischemia and significant fibrosis have already occurred. 19,20 HBO response rate has been assessed as 27%–92% with a recurrence rate of 8%–63%. 21 Chuang and colleagues retrospectively reviewed six patients with refractory HRC who underwent 200 U bladder botulinum toxin A (BoNT-A) injections. The authors reported promising results of BoNT-A injection in patients with refractory RC. 22 Chondroitin sulfate and hyaluronic acid have been also used intravesically to treat HRC. The authors of a pilot study noticed a significant reduction in nocturia. 23 Two other non-randomized studies on glycosaminoglycans in HRC reported a significant increase in bladder capacity, relief of pelvic pain and dysuria, and a reduction in overactive bladder scores. 24,25 Formalin has also been described in the intravesical treatment of HRC in small reviews. By the occlusion of telangiectatic tissue, 26 formalin use is associated with a range of hematuria resolution that goes from 70% to 89%, but rates of serious complications are as high as 30%. 27,28
As regards the costs, one application of 12 mL FG was used for each of the 20 patients. The cost for the entire process to generate 6 mL of FG is 500 Euros (12 mL costs 1000 Euros). In 2012, Smart and Wallington analyzed the direct costs of treating RC with HBO treatment. HBO costs were 12,014.95 Australian dollars (about 7585 Euros) in 38 treatments spread over 60 days. 29 Although there seems to be a significant cost reduction with FG compared with a complete cycle of HBO, this Australian article analyzed the cost of only a single patient. More focused studies are needed to better clarify the cost-effectiveness of FG compared with HBO or other techniques.
Endoscopic FG application has recently been described as an innovative and efficacious treatment even for refractory HC after unrelated marrow, cord blood, and haploidentical hematopoietic stem cell transplantation. 2,6 FG is generally used in various surgical fields, including urologic procedures, with favorable results. 5,30
Although this is a pilot non-controlled study on a limited number of patients, it appears to be an innovative and affordable technique. FG has never been used for HRC, and we report the first application series ever described in urologic literature. Further studies are necessary on a larger sample of patients. Randomized clinical trials (RCTs) are needed to compare FG with other HRC treatment options.
The use of a cystoscope to allow visualization of the mucosa together with a rotating endoscopic catheter to spray the glue onto the damaged areas are important contributors to the optimal application of fibrin adhesive within the bladder. Concomitant use of CO2 insufflation maintains a constant pressure in the bladder and avoids overflow and overdistension. Since FG adheres rapidly to human tissue, the risk of blood or urine washing away the glue is minimal. This is important for the promotion of tissue repair process. The outcome of this pilot study indicates that endoscopic application of FG appears to be a simple and safe therapeutic option for the management of refractory HRC. Even in those patients who take dual antiplatelet therapy, FG has been successful, suggesting a protective role of FG itself on bladder urothelial barrier and vascular epithelium. In addition, the procedure is repeatable in the event of HRC relapse. We recommend that FG treatment should be administered as soon as possible after the onset of HRC, since the hemostatic and reparative effects of the glue may limit further damage to the bladder mucosa. We also recommend that the use of FG in this clinical setting should be prospectively investigated using a large patient cohort to more accurately define its role within the context of current management and to further evaluate its efficacy and impact on the need for transfusion support, length of hospitalization, quality of life, and costs.
Conclusion
Endoscopic intravesical FG application for HRC led to an increased therapeutic response rate in patients who failed with conventional therapy and endoscopic clot evacuation and hemostasis. Application of FG is an effective, practical, affordable, and repeatable procedure for the treatment of grade ≥2 HRC. Further studies are mandatory to better clarify the benefits of FG in HRC.
Footnotes
Acknowledgment
The authors acknowledge. Karen Lipworth for her precious help in language review.
Disclosure Statement
No competing financial interests exist.