
Abstract
Introduction:
Endoscopic management of upper tract urothelial carcinoma has become more popular over the last few decades as there has been an impetus for renal preservation in these patients. While radical nephroureterectomy has been the gold standard in treatment of this disease, ureteroscopic and percutaneous management has become a viable option for select patients.
Methods and Materials:
The literature on endoscopic management of upper urinary tract tumors was explored. Different management methods are discussed, both from published literature and experience of the authors of this chapter.
Results:
We review the indications, details of the procedure, and troubleshooting methods in the endoscopic management of upper tract urothelial carcinoma. Imperative indications as well as controversial indications are discussed. The role and efficacy of adjuvant intrarenal topical agents are examined as well as the protocol for administering these agents. Follow-up protocols are also reviewed.
Discussion:
In select patients, endoscopic management with ureteroscopy and/or percutaneous resection of upper tract urothelial tumors is appropriate and can preserve renal function while obtaining comparable oncologic control compared with radical surgery.
Indications
Traditionally, radical nephroureterectomy has been the gold standard treatment for high-grade, large-volume upper urinary tract urothelial tumors with a normal contralateral kidney. Over the past few decades, the role of ureteroscopic and percutaneous management of upper tract urothelial carcinoma gained popularity. The goal of the endoscopic approach is to preserve kidney function while attempting to achieve oncologic control similar to radical surgery. Ureteroscopy is used not just for diagnosis but also as a therapeutic means in the treatment of low-grade, low-volume, noninvasive disease. Percutaneous resection is preferred over ureteroscopy in cases of larger tumors or tumors in unfavorable locations via retrograde ureteroscopic approach (i.e., lower pole calix). Staging is also more feasible through the percutaneous approach where ureteroscopy often falls short. Furthermore, the percutaneous approach allows for antegrade intrarenal instillation of topical adjuvant treatments, such as Bacillus Calmette-Guérin (BCG) or mitomycin C (MMC).
The imperative indications for endoscopic management of upper tract urothelial carcinoma are the presence of low-grade tumor(s) in a solitary kidney, bilateral tumors, or chronic renal insufficiency. Renal preservation rates have been reported between 60% and 80% with follow-up periods of 3–6 years. 1 –3 Moreover, the endoscopic approach may be more appropriate for patients who cannot tolerate major surgery, as it is associated with lower complication rates with similar overall survival rates compared with radical surgery. 3 However, both the urologist and the patient must understand that local recurrence rates are high, obligating the patient to frequent surveillance cystoscopies and ureteroscopies. Tract seeding is another potential disadvantage of the percutaneous approach, although this is limited to a small number of case reports. 4
With the development of better equipment and improved techniques, the endoscopic approach has been used in patients outside of the abovementioned imperative indications. Although there have not been any randomized control studies comparing endoscopic vs radical surgery, many case series have been published supporting the practice of endoscopic resection of upper tract urothelial tumors in patients with a normal contralateral kidney. 4 –7 Some studies have even described similar survival rates in patients with high-grade tumors treated endoscopically in select patients. 8,9
Preoperative Preparation
To assess candidates for the endoscopic approach, a full medical and surgical history, as well as physical examination, is essential. In patients at low risk for perioperative cardiovascular events, aspirin can be held 7–10 days before surgery, although there is evidence that continuing low-dose aspirin does not significantly increase the risk of bleeding in percutaneous nephrolithtomy. 10,11 Depending on the medical indication, certain patients may have imperative indications to continue antiplatelet therapy, and this decision should be made in conjunction with the patient's internist or cardiologist. A complete blood count, basic metabolic panel, and coagulation studies should be obtained to assess for anemia, renal function, and bleeding disorders. A preoperative urine culture is required, and any infection should be treated before surgery. In cases with sterile preoperative urine culture, the American Urologic Association Best Practice Statement recommends 24 hours or less of a first- or second-generation cephalosporin as first-line antimicrobial perioperative prophylaxis. 12
Ideally, recent cross-sectional abdominal/pelvic imaging with delayed phase cuts (i.e., CT urography) should be obtained for surgical planning. Preoperative imaging is used to assess tumor burden, identify the optimal calix of entry, and ensure extrarenal organs are away from the intended percutaneous tract. Recent imaging can also dictate which treatment modality a patient requires—that is, if there is progression of disease or invasion into parenchyma, the patient would no longer be a candidate for endoscopic management.
Patient Positioning
After induction of anesthesia in the supine position, the patient is repositioned to dorsal lithotomy for a thorough cystoscopy if the bladder has not been inspected recently. An open-ended 5F or 6F ureteral catheter is inserted at this time into the ureter of interest to enable opacification of the collecting system. The patient will remain in this position if a ureteroscopic approach is performed.
The patient is then turned to the prone position if percutaneous resection is deemed appropriate. Gel rolls are placed underneath the torso to prevent hyperextension of the neck. The arms are abducted with the elbows below 90-degree angles on armrests on each side. All pressure points should be padded. Alternatively, if leg extenders are available, the entire procedure can be performed in the prone split-leg position. With the hips abducted, the urethra is easily accessible, allowing for cystoscopic surveillance as well as retrograde flexible ureteroscopy possible through this position.
Surgical Steps
Ureteroscopic evaluation and biopsy
When performing ureteroscopy for diagnosis and treatment of upper tract urothelial tumors, one should minimize trauma to the upper urinary tract. A 5F or 6F open-ended ureteral catheter inserted cystoscopically can be used to obtain ureteral washing with physiologic saline if selective cytology is warranted. Provided the ureteral orifice is patent enough, a flexible ureteroscope can be advanced into the ureter without the use of guidewires, to prevent any trauma or dislodgement of tumor and for better detection of carcinoma in situ. If available, using a smaller 7.5F flexible ureteroscope may avoid the need for ureteral dilation. If a ureteroscope is not easily passed, retrograde pyelography should be performed through an open-ended ureteral catheter to obtain a roadmap of the collecting system and identify any filling defects. Then, a sensor-tipped guidewire can be passed into the ureter up to the level of the renal pelvis under fluoroscopic guidance, and the flexible ureteroscope may be able to be passed over the wire more easily. Balloon dilation of the ureteral orifice may be necessary if the ureteroscope is still unable to be passed at this point.
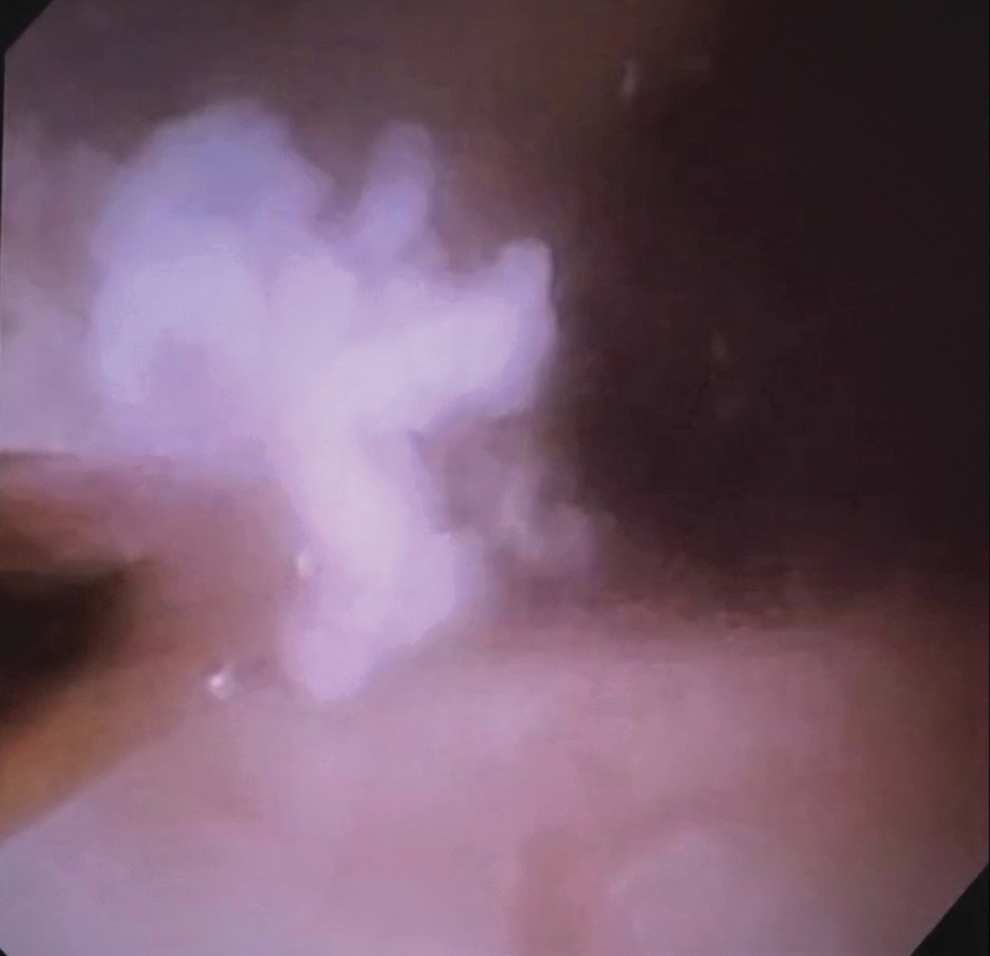
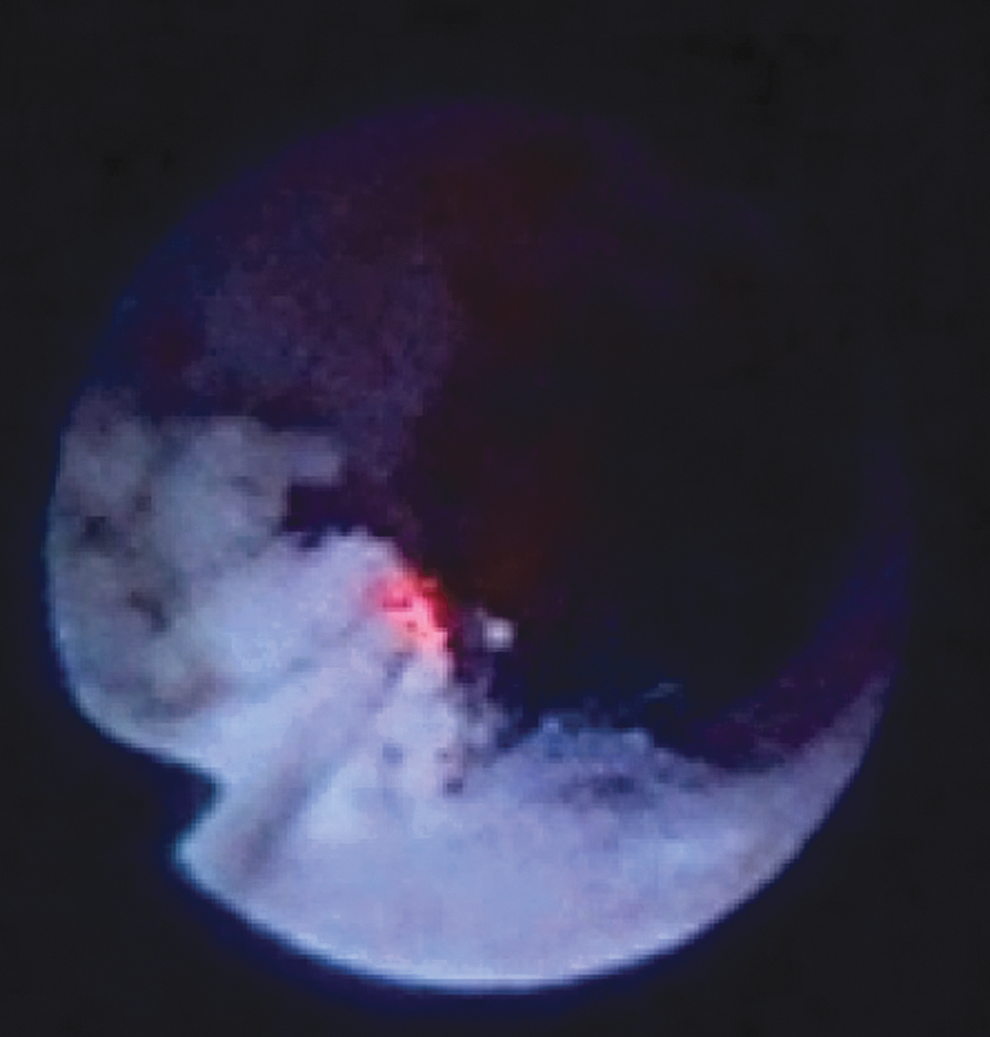
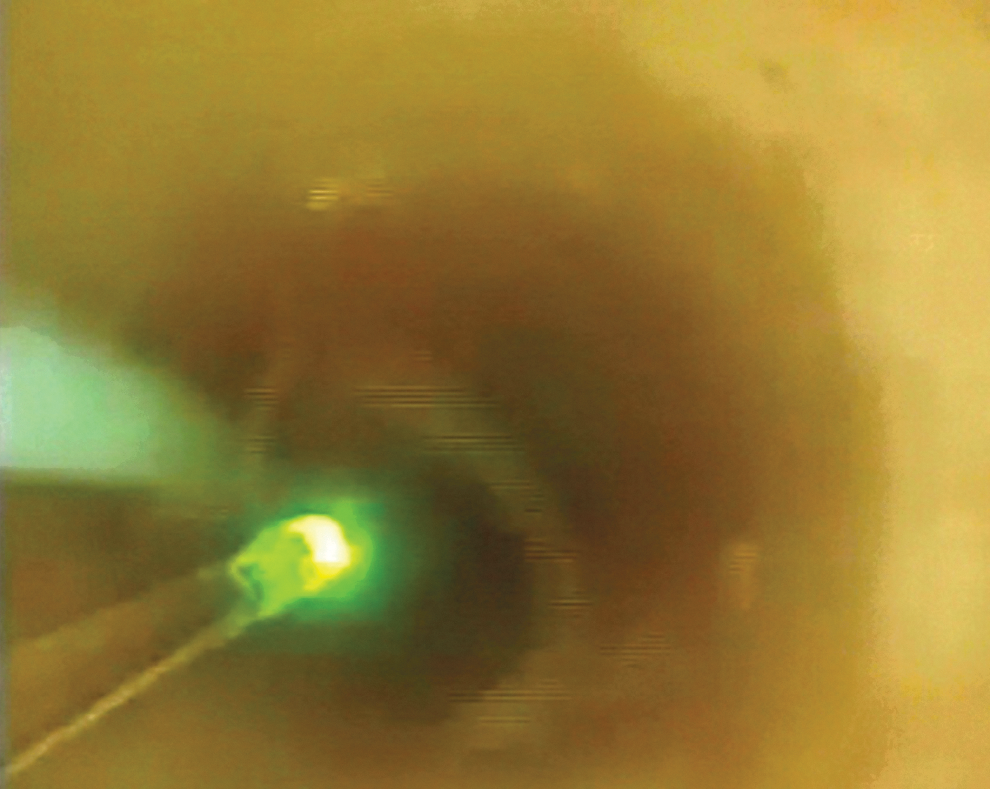
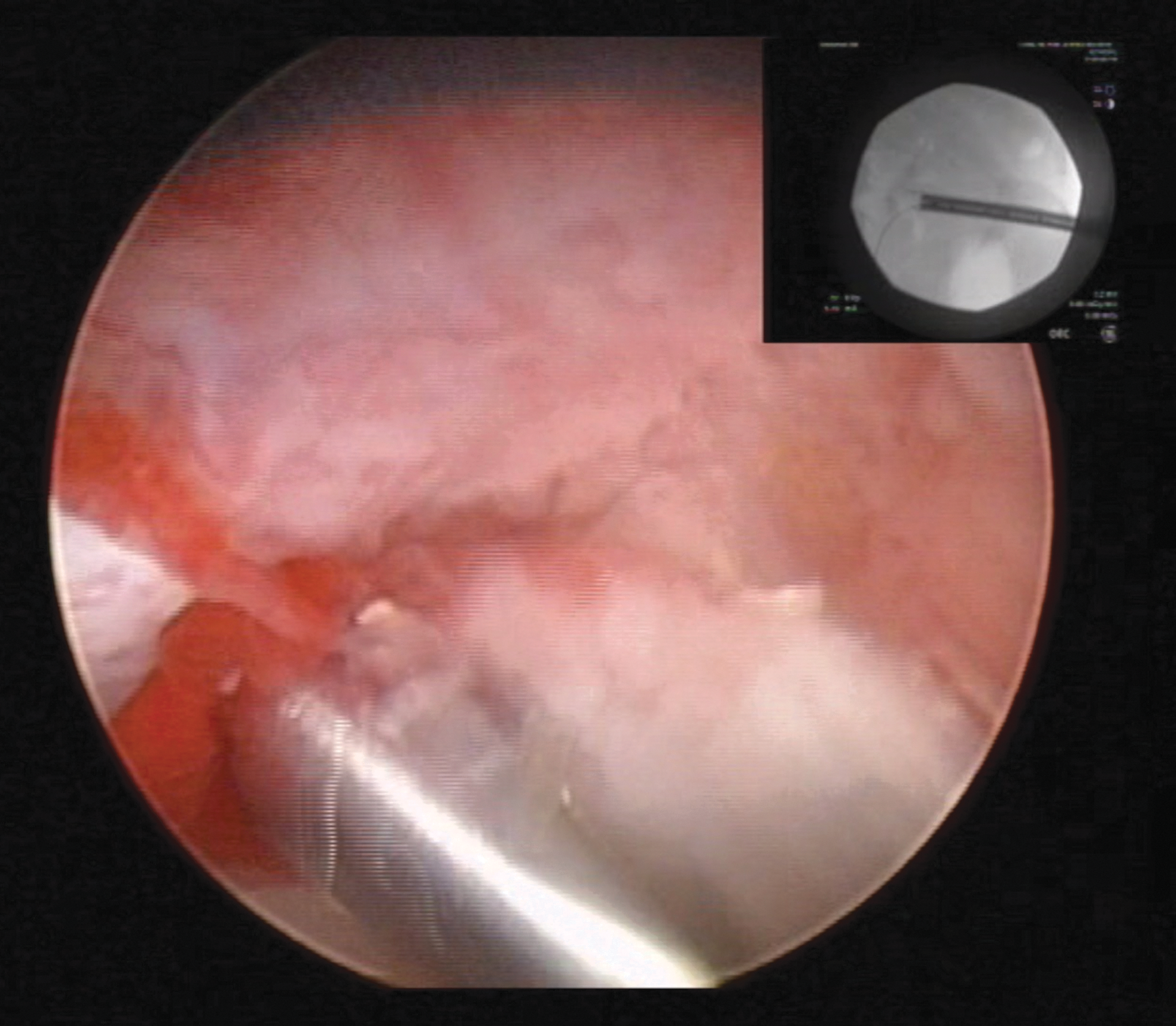
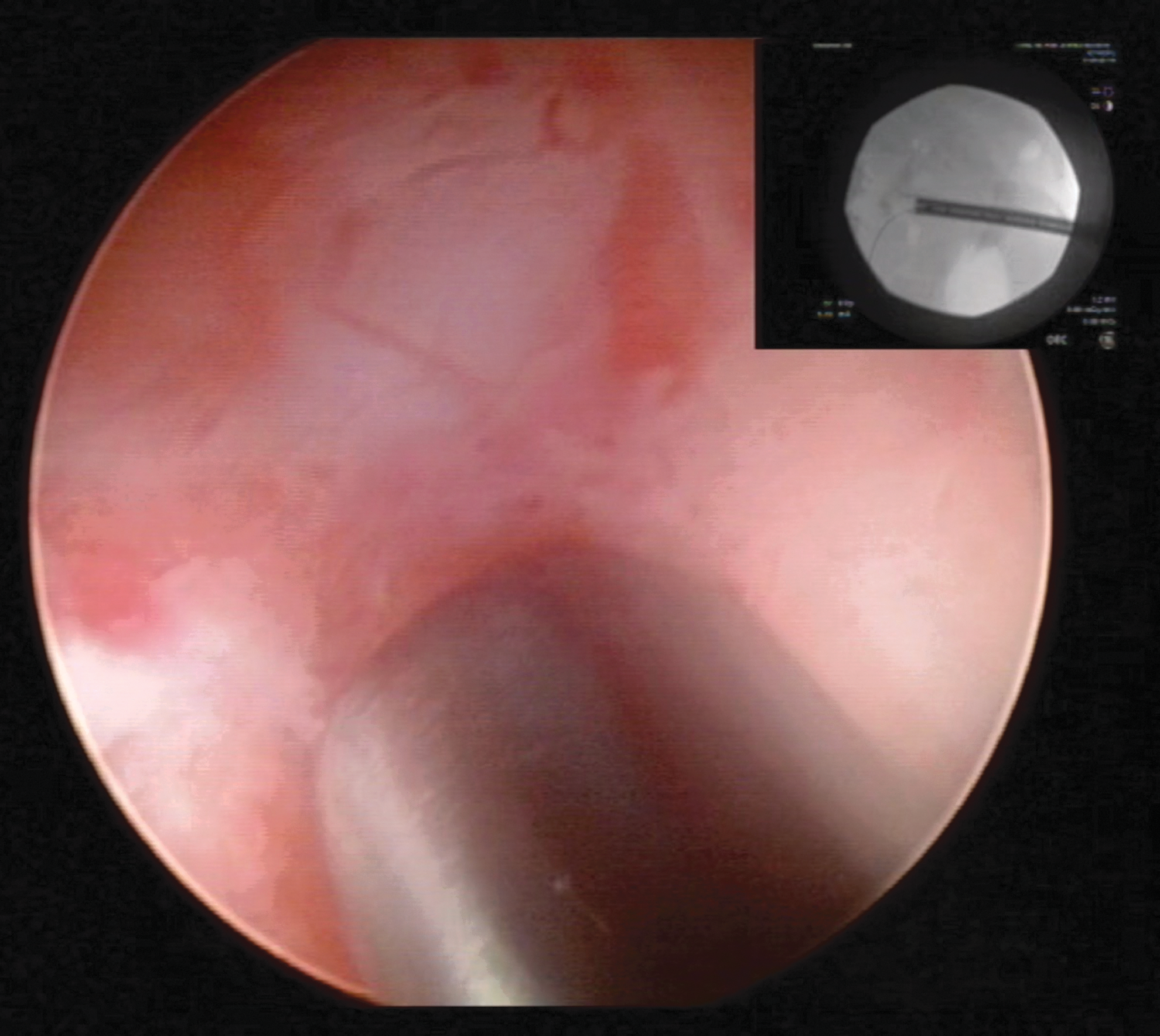
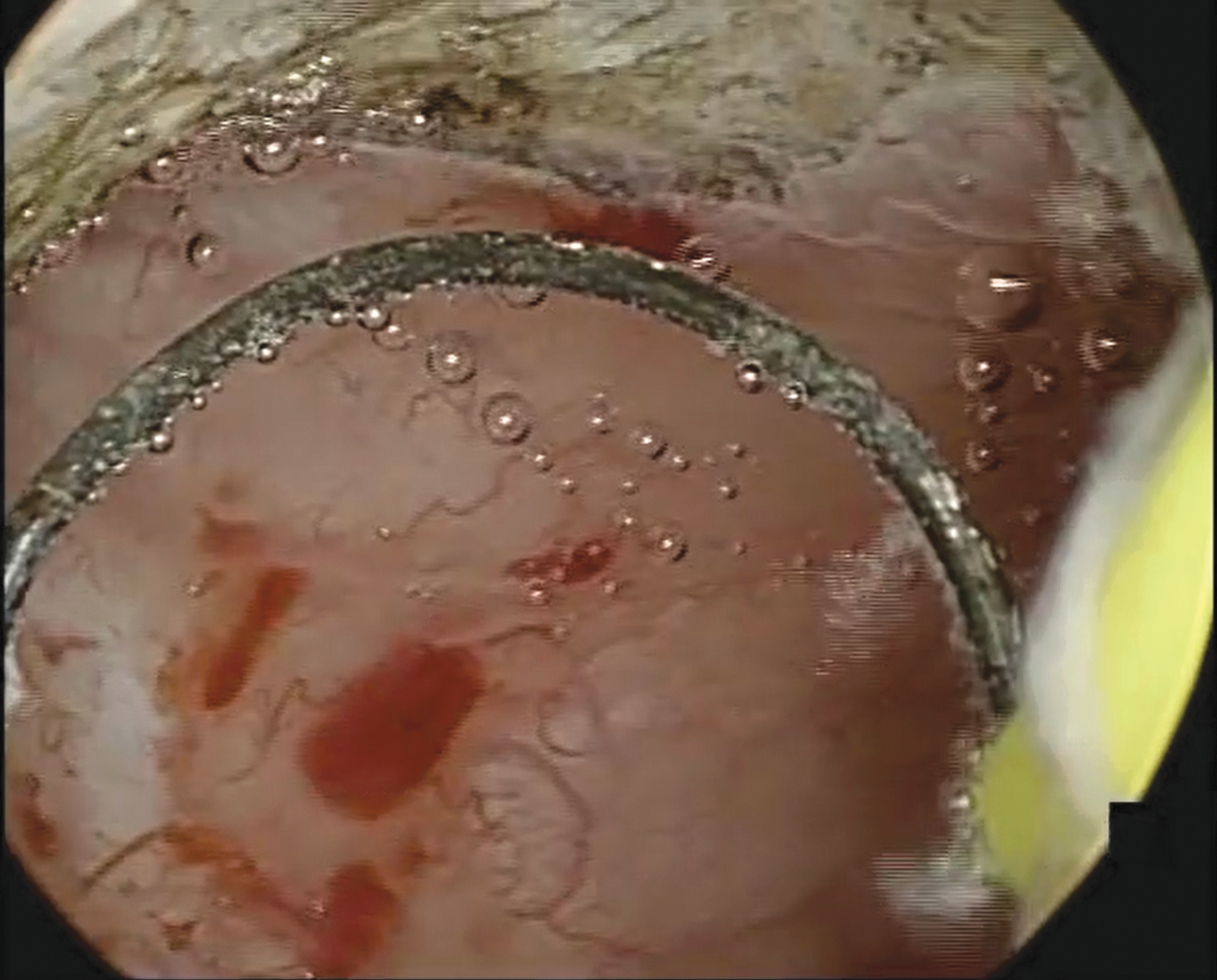
Once the ureteroscope is advanced into the ureter, the entire upper tract should be visualized, and physiologic saline washing of any suspicious areas should be performed. Narrow band imaging, if available, may help detect subtle abnormalities in the urothelium (Figs. 1 and 2). 13 If any papillary tumors are seen, a ureteroscopic cold cup biopsy forceps (Figs. 3 and 4) or stone basket (Figs. 5 and 6) can be used to remove the tumor at its stalk. The specimen is best sent to the cytopathology laboratory as it is usually too small to be sent for conventional pathologic review. Next, the tumor base is treated using electrocautery or laser energy (holmium:YAG, neodymium:YAG, or thulium). The holmium laser has a 0.5-mm depth of penetration and can safely be used in the ureter and renal pelvis (Fig. 7). Commonly used settings are an energy of 0.6–1.0 J with a frequency of 10 Hz. In comparison, neodymium laser has tissue penetration of up to 5 mm and works by coagulative necrosis. The thulium laser has a shallower depth of penetration at 0.25 mm and has similar tissue effects as the holmium laser, but has a continuous rather than pulsatile wave pattern (Fig. 8). After all tumors are ablated, a ureteral stent is typically left in place to aid in the healing process.
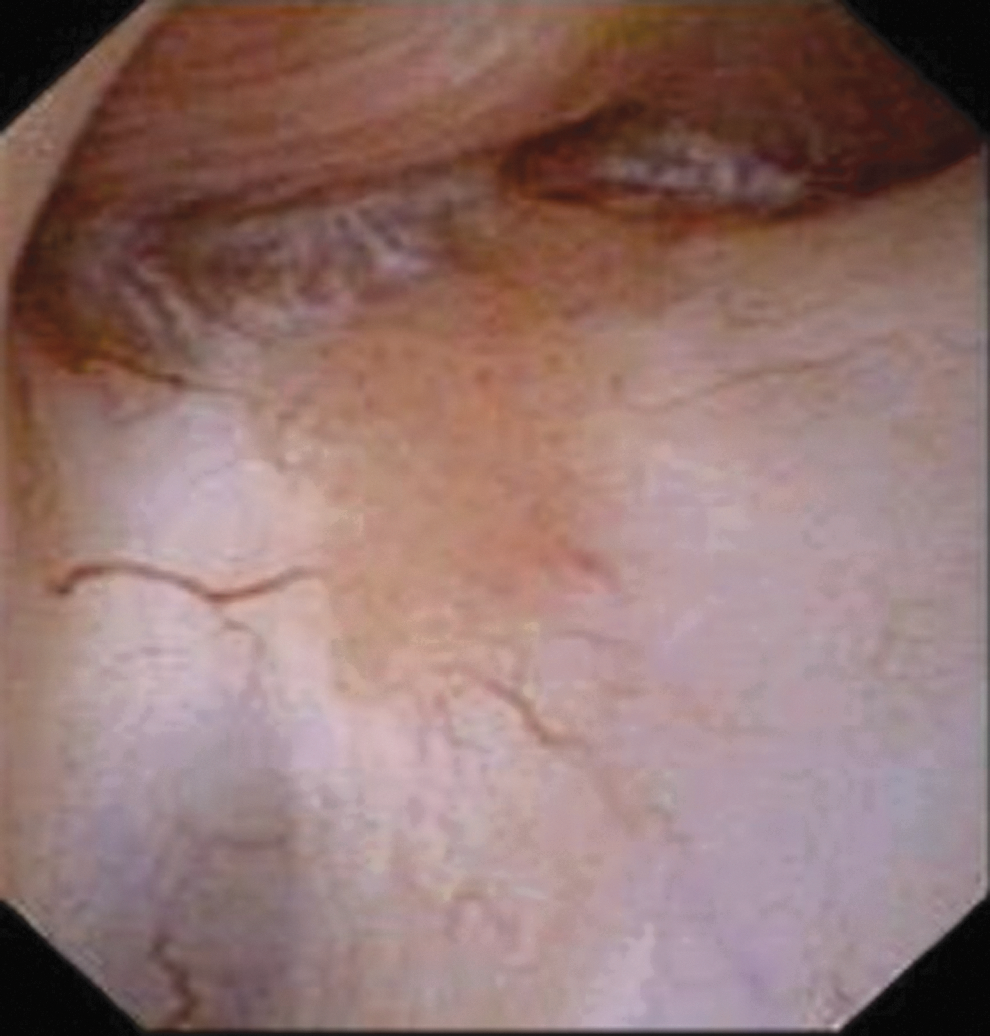
White light ureteroscopic image of urothelial tumor.
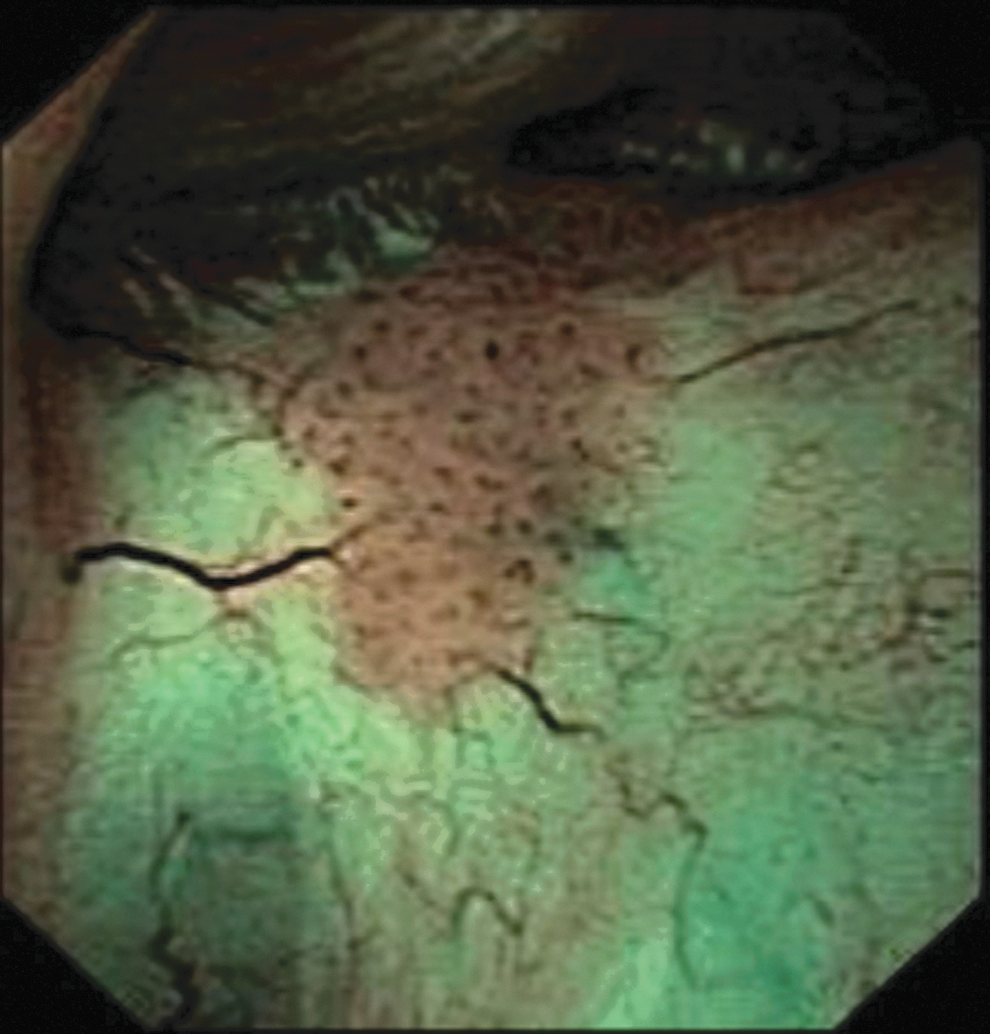
Ureteroscopic image of urothelial tumor with narrow band imaging.
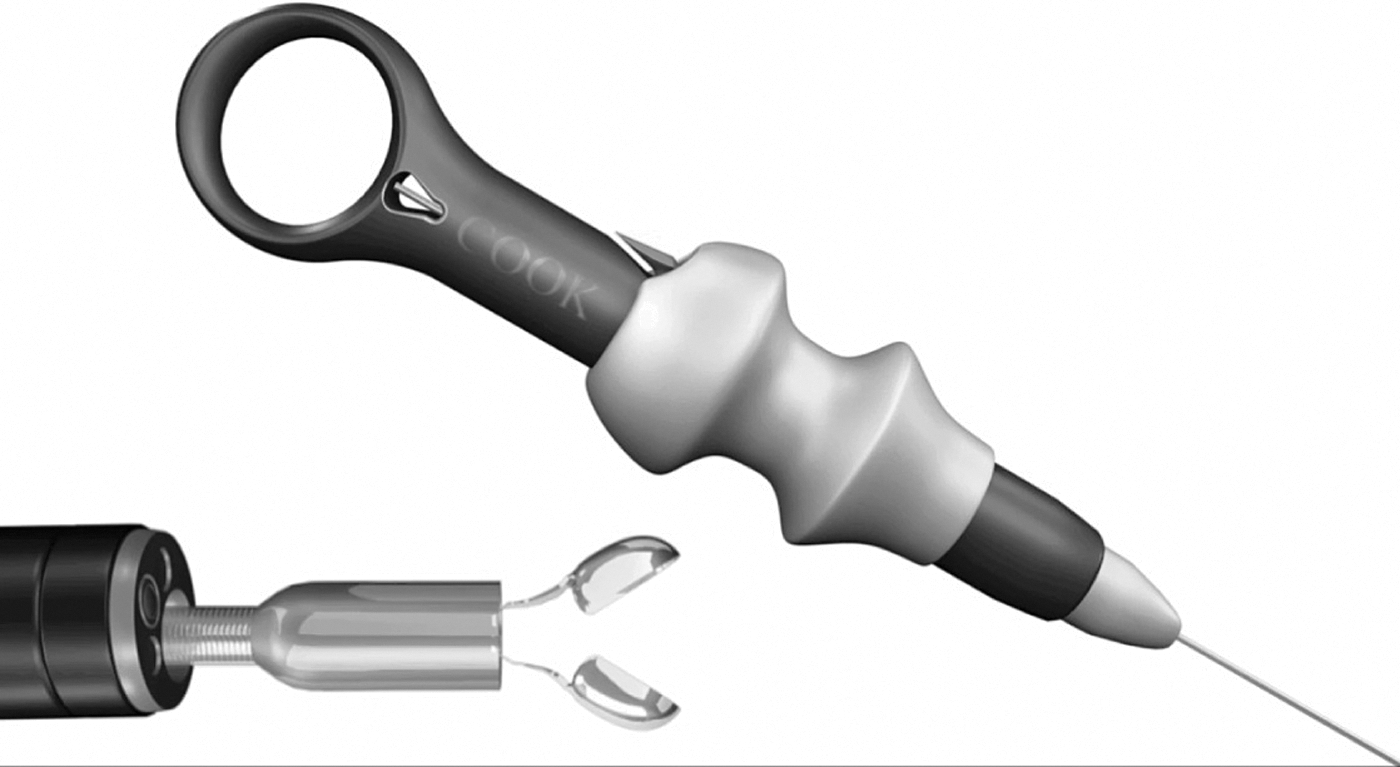
Ureteroscopic BIGopsy cold cup biopsy forceps with handpiece (permission for use granted by Cook Medical, Bloomington, IN).

Ureteroscopic biopsy of renal pelvis tumor (permission for use granted by Cook Medical).
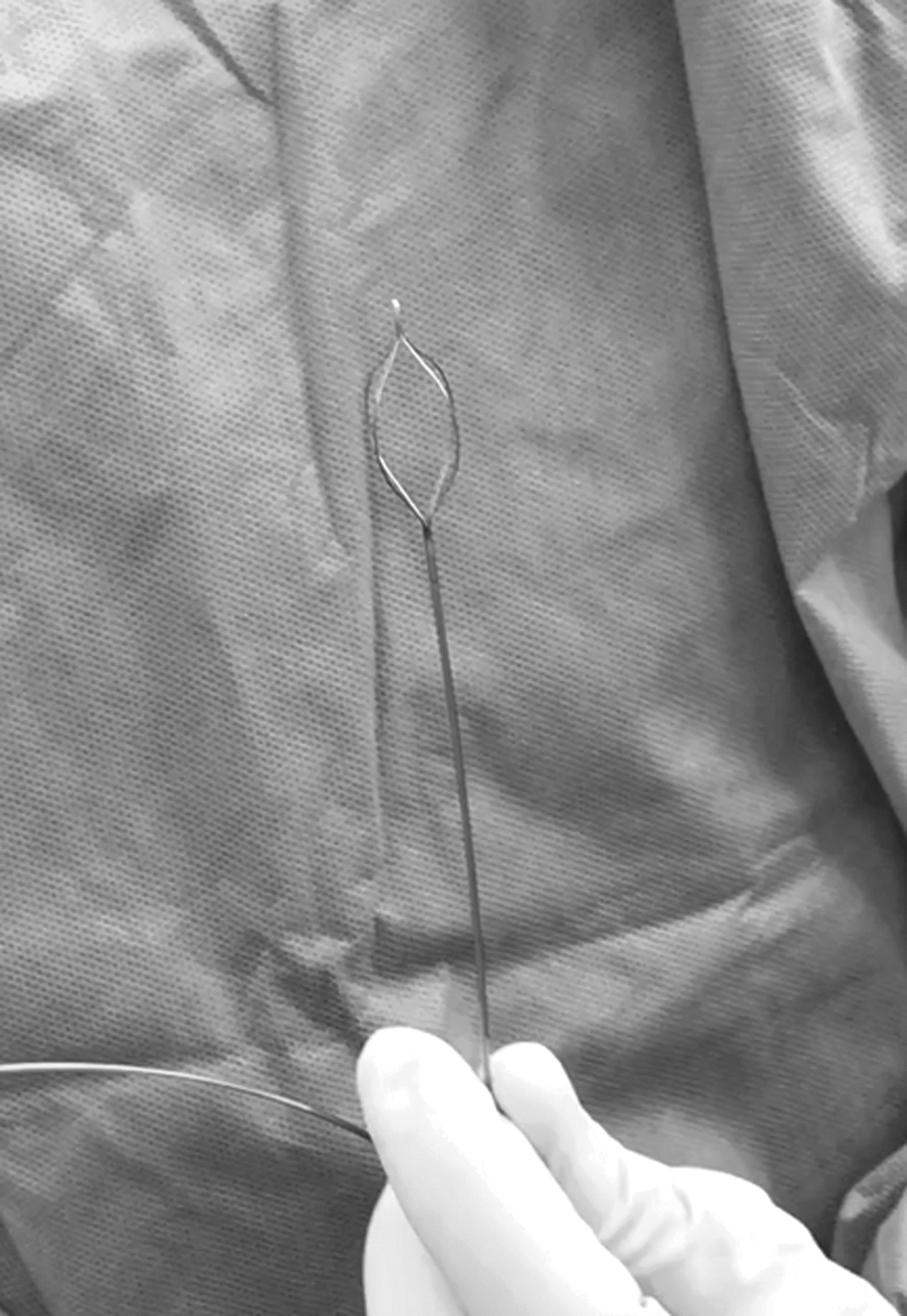
Segura basket.
Tumor within Segura basket.
Holmium lasering of ureteral tumor.
Thulium laser in ureter.
Nephrostomy tract access
Proper selection of the calix of entry is critical in optimizing the amount of tumor able to be resected. Tumors in posterior calices are best accessed by direct puncture into the affected calix. Anterior caliceal tumors may be difficult to access directly and may require flexible nephroscopy through a posterior calix. Renal pelvis and upper ureteral tumors should be approached through an upper or middle calix to allow the nephroscope to be maneuvered in the renal pelvis and upper ureter with minimal torquing of the kidney. However, caution should be used when obtaining access into the upper pole to minimize the risk of pleural injury, especially if it requires a supracostal puncture.
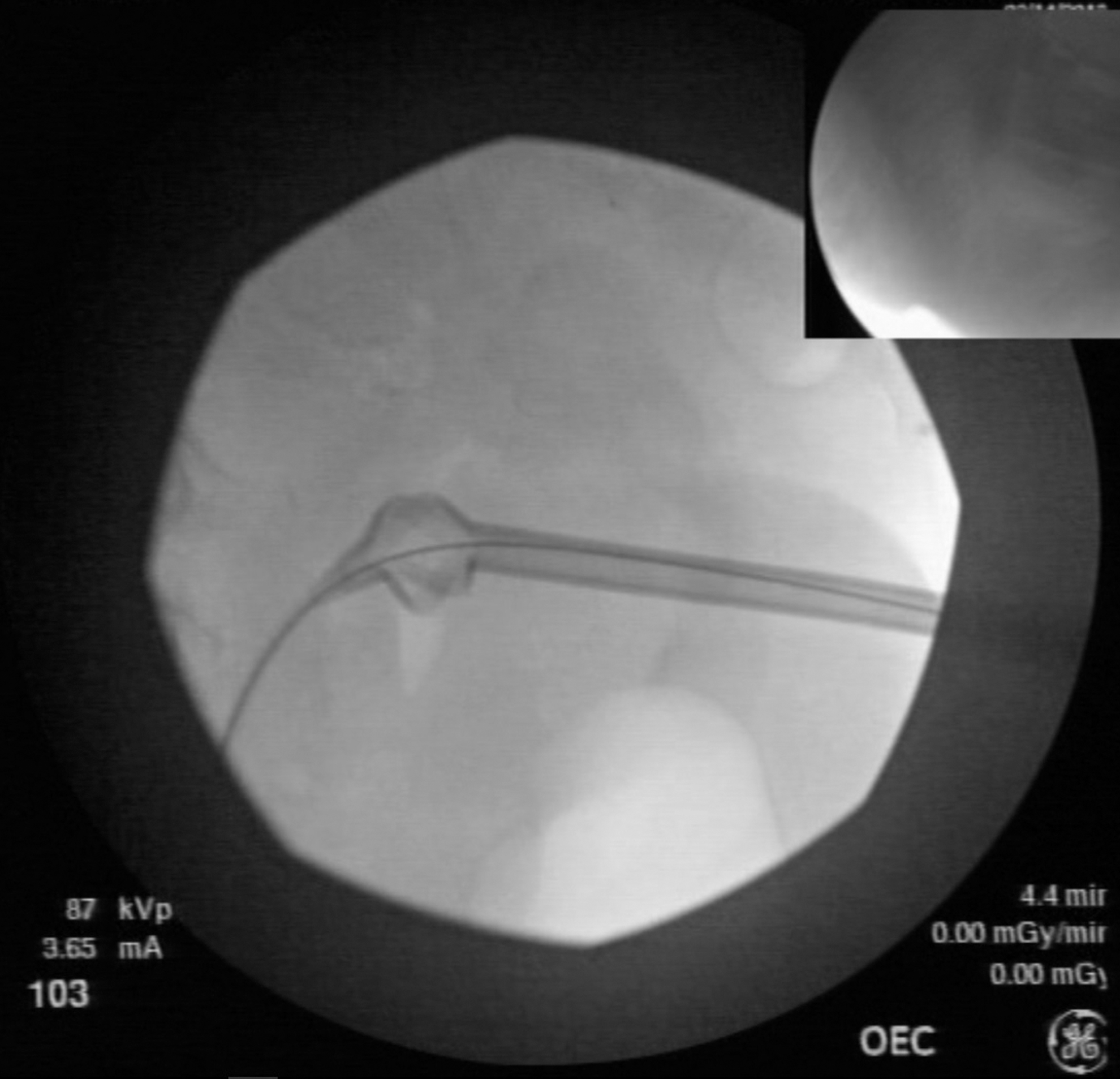
Radiopaque contrast is injected through the open-ended ureteral catheter that was previously placed in the ureter to opacify the collecting system. A diamond-tipped 18-gauge needle is used to access the desired calix either by the bull's eye or triangulation technique with fluoroscopic guidance. Once a wire is secured in the collecting system, the tract is dilated to 30F using either sequential renal dilators or a balloon dilator.
Percutaneous resection
Once the 30F Amplatz sheath is positioned in the proper calix, the rigid nephroscope is passed into the collecting system to visualize the tumor directly (Figs. 9 and 10). Secure placement of the sheath should be ensured to minimize the risk of tract seeding. Using the cold cup biopsy forceps, the tumor is removed piecemeal without creating thermal artifact that loop electrocautery may create (Fig. 11). A biopsy of the base of the tumor is essential in proper staging (Fig. 12). Once the bulk of the tumor burden has been removed, a resectoscope with loop electrocautery can then be used to fulgurate the base of the tumor and establish hemostasis (Fig. 13). The loop can also be used to resect any remaining tumor using the cutting current. Care must be taken not to cut too deeply into the parenchyma, which could cause intractable bleeding. Furthermore, cauterization should be minimized near the infundibula and ureteropelvic junction to avoid stenosis. Hemostasis of the tumor base can also be achieved using a rollerball or bugbee electrode (Fig. 14). Flexible nephroscopy and the use of laser energy can be used to treat tumors within adjacent calices that the rigid scope may not reach without creating a separate percutaneous tract.

Advancement of Amplatz sheath under fluoroscopy.
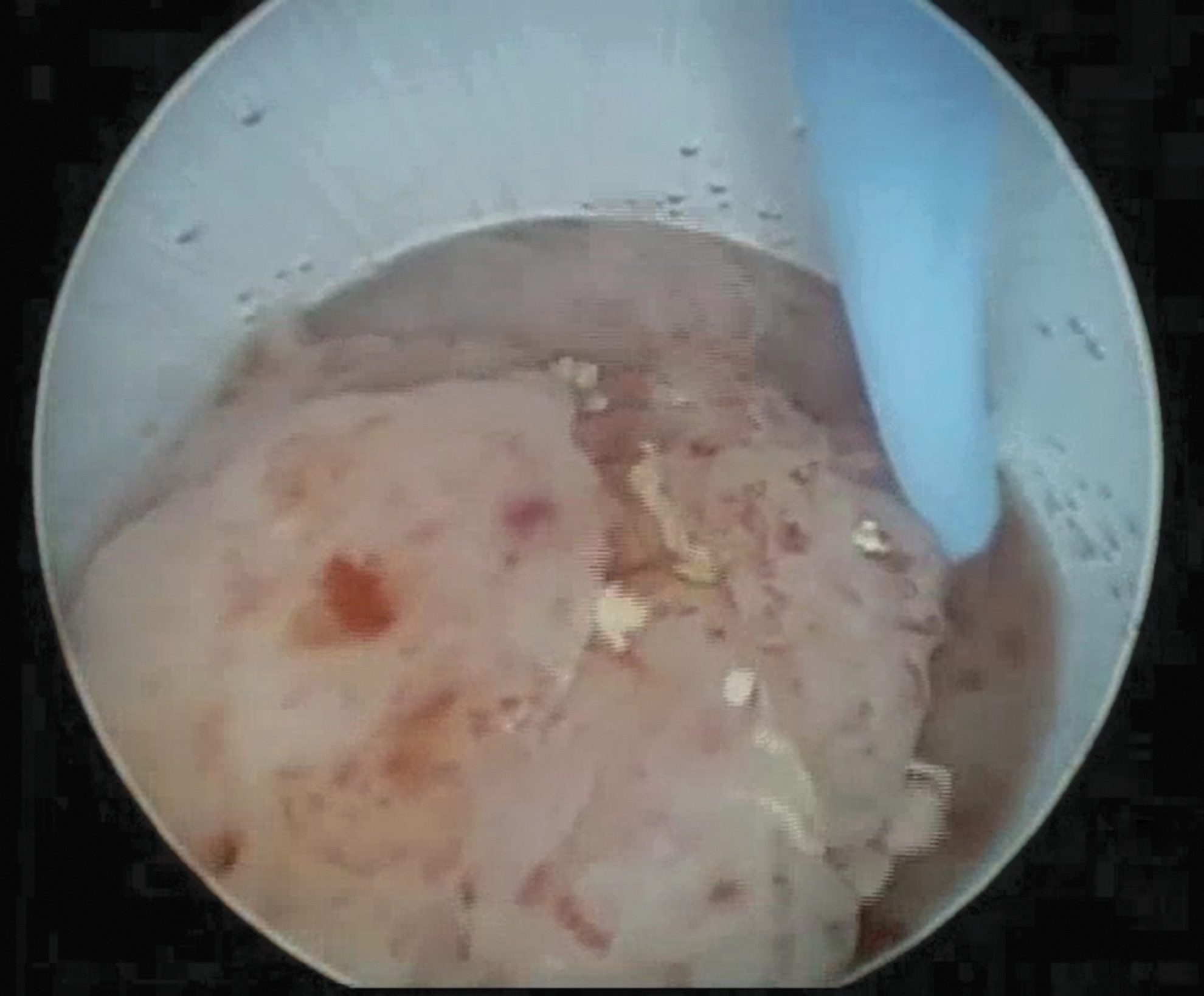
Tumor within the Amplatz sheath under nephroscopy.
Nephroscopic cold cup biopsy.
Biopsy of base of tumor.
Bipolar loop fulguration of base of tumor.

Fulguration with Bugbee electrode.
A second-look nephroscopy to ensure completeness of resection should be done at least 2 days after the initial resection to permit any ongoing bleeding to subside. Residual tumor may have been missed because of bleeding during the initial resection. An Amplatz sheath should be placed when there is considerable amount of residual tumor requiring a resectoscope or rigid nephroscopy. If the patient is to receive adjuvant intrarenal topic therapy, a 10F to 14F Cope loop nephrostomy tube is left in place.
Intrarenal instillation of topical therapy
Instillation of BCG or MMC into the collecting system can be performed through an indwelling nephrostomy tube as adjuvant treatment for select patients. Adjuvant BCG has been shown to decrease local recurrence rates and disease progression in patients with carcinoma in situ of the upper tract, but the oncologic benefit for Ta or T1 tumors is unclear. 6,14,15 Published oncologic results for adjuvant MMC for Ta/T1 tumors are promising but length of follow-up is relatively short. 16 While the risk of sepsis from BCG has been established, no systemic side effects from intrarenal instillation of MMC have been reported.
BCG should not be instilled until at least 2 weeks after resection and a negative urinalysis has ruled out an infection. Before the infusion, contrast should be injected through the nephrostomy and unobstructed flow from the renal pelvis to the bladder should be confirmed with fluoroscopy. A dose of 81 mg of TheraCys BCG therapy is diluted into 50 mL of physiologic saline and infused over 1 hour. 6 Manometry monitoring is used to ensure the intrarenal pressure is below 25 cmH20. A total of 6 weekly treatments are given, mimicking the intravesical protocol for BCG. MMC is administered in the same manner, with a dose of 40 mg in 40 mL of sterile water.
Postoperative Care
The immediate postoperative period is similar to that of a patient after a percutaneous nephrolithotomy, except a nephrostomy tube is almost always left in place to facilitate a second-look nephroscopy during the same admission. After the initial resection, a re-entry nephrostomy catheter with an 18-cm extension allows for easy access to the ureter with safety guidewire during the second look (Fig. 15). Complete blood count should be monitored in the recovery room and on the first postoperative day. If there is a high suspicion for pleural injury (i.e., supracostal access), a chest X-ray should be obtained in the recovery room. After the second-look procedure, a nephrostomy tube of smaller caliber (10F–14F) is left in place if instillation of topical adjuvant therapy is planned as an outpatient. However, if there is no bleeding from the second procedure and adjuvant therapy is not indicated, a nephrostomy tube is often not necessary.
Re-entry nephrostomy under fluoroscopy.
Surveillance of the upper tract with ureteroscopy and CT urography should follow a strict protocol as local recurrence occurs at a high rate following endoscopic management of upper tract urothelial carcinoma. Our protocol is to perform upper tract surveillance every 3 months to rule out any recurrence for 1 year and then every 6 months for 2 years. Yearly ureteroscopies or CT scans should then be performed for another 2 to 3 years. Careful cystoscopy should also be performed during each ureteroscopy. Incision of the ureterovesical junction has been described in patients who require frequent surveillance of the upper tract, enabling flexible ureteroscopy without the need for wires or dilation and facilitating reflux for intravesical instillations of adjuvant topical agents when needed. 17
Troubleshooting
Percutaneous surgery of upper tract urothelial tumors has similar complications as percutaneous surgery for stones, including bleeding, perforation of the collecting system, sepsis, injury to surrounding organs, and incomplete resection. Unique to percutaneous resection of upper tract tumors is the risk of bleeding due to excessively deep cuts with the resectoscope. This can be avoided by using the rigid grasper to debulk the tumor until the base is visualized. The cold cup biopsy forceps can be used to obtain a biopsy of the base and the tumor base can be fulgurated with a rollerball electrode rather than a loop electrode to ensure that cauterization occurs superficially. If significant tract bleeding is encountered, the sheath can be advanced into the collecting system to tamponade any open vessels. Excessive bleeding may oblige the surgeon to abort the case, at which time a large bore re-entry nephrostomy tube or balloon catheter is inserted to control bleeding. The nephrostomy tube should be allowed to clot off or even capped to create pressure within the confined space of the retroperitoneum to facilitate hemostasis.
Sometimes a calix is not easily accessible, and more than one approach may be necessary to resect the entire tumor. Large-volume tumors of the renal pelvis are best approached through an upper pole calix to minimize the amount of torque needed to access the lower pole and proximal ureter. Combining retrograde ureteroscopy with the percutaneous approach may save the patient multiple punctures and tracts.
Supplementary Video
Supplementary Video S1 describes the indications and techniques of endoscopic management of upper tract urothelial carcinoma and is available online at
Recommended Videos from Videourology
1. Jutzi S, Kramer MW, Wolters M, Kuczyk MA, Herrmann TR, Imkamp F. Laser En-Bloc Resection of Solitary Papillary Tumors in the Upper Urinary Tract: Description of the Technique Using a Thulium:YAG-Laser. September 2014, 28.
2. Geavlete P, Georgescu D, Multescu R, Mirciulescu V, Geavlete B. Improving the Diagnosis of Upper Urinary Tract Tumors: Narrow Band Imaging Technology. Journal of Endourology Part B, Videourology. September 2013, 27.
Footnotes
Acknowledgments
We would like to thank the previous Endourology fellows who graduated from the Smith Institute of Urology for providing some of the images and video clips in this manuscript. These prior fellows include Dr. Mantu Gupta, Dr. Phil Zhao, Dr. Piruz Motamedinia, and Dr. Sammy Elsamra.
Author Disclosure Statement
No competing financial interests exist.