
Abstract
Introduction and Objective:
Robot-assisted sacral colpopexy (RASC) is a fast growing approach for surgeons treating patients with advanced stage pelvic organ prolapse (POP). Open abdominal sacral colpopexy has been the gold standard for advanced POP but requires longer hospital stays and a much larger incision. The indications, preoperative preparation, operative positioning, and operative steps are detailed, and an accompanying video shows the approach.
Methods:
RASC can be broken down into 11 steps and the reader will be able to reference the article to the corresponding portion of the video.
Results:
A total of 119 women underwent RASC between 2009 and 2016. Patients had similar preoperative characteristics. All POP-Q, UDI-6, and quality of life scores improved postoperatively. Apical failure was noted in 0, anterior failure was noted in 7 (average Ba +1.1 cm in failures), and posterior failure was noted in 4 (mean Bp +1.0 cm) patients at 15.6 months' follow-up. A total of 11 suture erosions were noted in five patients requiring excision in the clinic and 2 patients in the operating room. Four suture erosions were managed with observation. Two mesh exposure events were noted.
Conclusion:
Outcomes for robotic sacral colpopexy are like those of open abdominal sacral colpopexy.
Introduction
Abdominal sacral colpopexy is the gold standard treatment for women with advanced pelvic organ prolapse (POP). Although highly effective with long-term durability, this open procedure is associated with significant surgical morbidities. 1,2 Minimally invasive techniques, such as laparoscopic sacral colpopexy, have many advantages over abdominal sacral colpopexy. Laparoscopic sacral colpopexy has been shown to achieve outcomes similar to the open approach but the procedure is technically demanding with longer operative times. 3 The introduction of the DaVinci® Surgical System in recent years has resulted in a paradigm shift for management of POP, and this approach has been increasing nationwide. 4 A recent meta-analysis demonstrated equivalent long-term outcomes for abdominal sacral colpopexy and robot-assisted sacral colpopexy (RASC). Serati and colleagues reviewed >1400 RASC procedures in the literature, highlighting the growing popularity of this approach. 5 The complications of RASC are not as well described in the literature as those for the open technique. Mesh extrusion has received significant attention recently and is among the most concerning complications from a patient perspective. The aim of this article is to describe indications, preoperative preparation, positioning, and technique for RASC. Outcomes data are presented from a single-institution experience with RASC.
Indications
Women who are symptomatic from POP and exhibit Stage II–IV POP by pelvic organ prolapse quantification (POP-Q) examination 6 are candidates for sacral colpopexy, using any approach. More specifically, there must be evidence of uterine or apical descent to consider sacral colpopexy. Absent apical descent, compartment-specific repairs are appropriate and sacral colpopexy is not necessary. Our group considers RASC when there is at least 2 cm of apical descent, and some groups have advocated additional criteria such as a Ba point by POP-Q examination no greater than −1. 7 Moreover, the inability to tolerate Trendelenburg position, such as untreated hiatal hernia, or unacceptable ventilation pressures once placed in this position, is contraindications to the robotic approach, but not necessarily open abdominal sacral colpopexy.
Concomitant procedures, such as hysterectomy, salpingo-ophorectomy, mid urethral sling, Burch culposuspension, culdoplasty, cystocele, or rectocele repair, can be left to the discretion of the surgeon. All patients should be counseled about the possibility of postoperative urinary incontinence, suture extrusion, mesh erosion, and the possible need for a staged continence procedure during preoperative consultations. Prior abdominal surgery is not a contraindication to robotic or laparoscopic approach, but this should be left to the surgeon's discretion.
Preoperative Preparation
Patients should be assessed preoperatively for the ability to safely tolerate a potentially prolonged operative procedure in the lithotomy position. Obese patients and prolonged operative time >4 hours have been associated with increased incidence of neurovascular complications. 8 The authors do not routinely perform bowel preparation. Anticoagulants with the exception of aspirin 81 and 325 mg dose are discontinued at the recommended times ahead of surgery.
Patient Positioning
The procedure is performed in the lithotomy position. As with all lithotomy procedures, it is important to ensure that the weight of the patient's leg is borne by the heel and not the calf when positioning the lower leg into the stirrup. The arms are padded and tucked to the patient's side (Fig. 1). In the case of exceptionally obese patients and a relatively narrow operative table, table extenders (“sleds”) can be used to support the arms. The robotic arms and port placement are effectively described by Chopra and colleagues using a “W” configuration to avoid clashing. 9 For the RASC, the authors prefer a single 5 to 8 mm bedside assistant port on the patient's right side, as opposed to the left-sided assistant described by Chopra and colleagues, because the sigmoid colon is reflected from right to left, exposing the right aspect of the sacral promontory, giving the assistant a direct approach. This is described in the accompanying video. The 8-mm port is large enough to pass most needles but does not require closure and may have less risk of port site herniation than a 12 mm bedside assistant port. Moreover, early in the Indiana University experience, the authors were closing 12 mm assistant ports in the lateral location and patients frequently complained of port-site pain postoperatively. If preoperative procedures such as localizing ureteral stents are planned, it is preferable to prepare and drape the patient once, allowing for both the cystoscopic procedure and the robotic procedure with a hybrid lithotomy drape having a collection bag and a large abdominal fenestrated area. Once the ports are placed, the legs in secure padded stirrups are lowered until the thighs are parallel to the axis of the spine (straight upper leg, bent knee, and lower leg pointing toward the ground). The patient is then placed in 27 degrees Trendelenberg position, with careful attention to airway pressures as well as blood pressure. Some patients are unable to tolerate this amount of Trendelenberg, but it is optimal for allowing the bowels to fall out of the pelvis and away from the operative field.

Arm tucked and wrapped with foam, legs in stirrups.
Surgical Steps
RASC is performed using DaVinci S and Si Surgical System (Intuitive Surgical, Sunnyvale, CA). The technique can be broken into 11 stages. The corresponding video segment is referenced below: 1. Video--Chapter 1, “Setup, Positioning, and Port Placement”: The four-arm robotic setup is detailed in an accompanying video of this article and the robot can be positioned between the legs, or to the side of the left leg to maintain access to the vaginal area. The side-docking technique is more prone to crashing of Arms 2 and 3 with the DaVinci SI® system but careful planning will avoid this. An assistant port is necessary, and can be 5 mm that is not large enough to pass needles, 8 mm (the authors' preference, large enough for needles as big as SH-1® but not CT-1®, and not large enough to accommodate rolled porcine dermis graft), or 12 mm (large enough for anything, but closure can result in port-site pain postoperatively in the authors' experience). Once ports are in place, 27 degrees of Trendelenburg position is used to allow the bowel to fall out of the pelvis. When hysterectomy was indicated, one of the following three techniques is used: (1) robotic total hysterectomy with one-layer vaginal cuff closure using polyglactin suture, (2) robotic total hysterectomy with two-layer vaginal cuff closure using two layers of polyglactin suture, and (3) robotic supracervical hysterectomy. Concomitant bilateral salpingo-ophorectomy can be performed in indicated postmenopausal patients. It is necessary to place a retractor in the vagina to expose the anterior vaginal wall. Vaginal retraction can be accomplished with a Breisky–Navratil retractor ( 2. Video--Chapter 2, “Exposure”: Hysterectomy is also done at this time. Instruments shown in the video are Arm 1 (right hand) Intuitive Monopolar Scissors®, Arm 2 (left hand) PK Dissector® but bipolar dissector can be used as well, and Arm 3 (far left hand) Intuitive Double Fenestrated Grasper® (this has longer “fingers” than the commonly used Prograsp® forceps but a weaker grip strength). 3. Video--Chapter 3, “Anterior and Posterior Dissection”: The bladder is typically filled with 120 mL of saline to better identify the reflection of the bladder wall and anterior vaginal wall, particularly in patients who have undergone prior hysterectomy as this can exhibit scarring. The anterior dissection is carried down to the level of bladder trigone whereas the posterior vaginal wall dissection is carried to the rectovaginal space. Usually an anterior dissection ranges from 5 to 10 cm in length. As a helpful measurement tool, the gray insulation on the DaVinci Monopolar Scissors device measures 5.5 cm. 4. Video--Chapter 4, “Bring in Needles and Mesh”: This can be done in many ways, the authors prefer to bring 4 × 2-0 PDS® or 4 × 2-0 Prolene® sutures (used for securing mesh or porcine dermis graft) as well as 0-Vicryl® to close vaginal cuff if a total hysterectomy is performed, as well as mesh, porcine dermis, or fascia lata through the assistant port. If the assistant port is only 5 mm, it is possible to use Robotic Arm 1 port, which is 8 mm, or the camera port (12 mm). The needles are “stored” in the right lower quadrant abdominal wall and once used, the needles are “stored” in the left lower quadrant abdominal wall, until the end of the case. Some surgeons may prefer to remove used needles immediately to reduce the risk of a lost needle. The mesh can be cut and tailored at this point. Many prefabricated type 1 polypropylene mesh prostheses exist, but the authors prefer to cut their own mesh into a “Y” configuration using a 10 × 15 cm sheet of type 1 polypropylene mesh (Fig. 4) based on the measured length of the anterior and posterior dissection. It is usually 3 to 4 cm wide and 5 to 10 cm long, with the balance of the 15 cm long sheet making up the “tail” of the “Y” (Figs. 5 and 6). Porcine dermis graft material can be measured and cut in the same way. Fascia lata is also offered to patients at Indiana University and can be harvested from the leg before positioning in lithotomy (Fig. 7). 5. Video--Chapter 5, “Secure Mesh Posterior”: This can be done in interrupted or running manner, with delayed absorbable suture or nonabsorbable suture. The key is to use Robotic Arm 3 and vaginal retractor to optimize exposure. 6. Video--Chapter 6, “Secure Mesh-Anterior”: This can be done before or after posterior fixation, depending on surgeon preference. 7. Video--Chapter 7, “Pass Needles for Sacrum”: The authors prefer to pass these needles in two stages to minimize suture tails obscuring the view in the pelvis. Traditionally, Prolene or Gore-Tex® sutures have been used to fix mesh to the sacrum, but Pro-tack® laparoscopic titanium tacks have also been used. The authors use 0-Prolene on SH-1 needles × 3 to secure the mesh to the sacrum, and either 2-0 Vicryl or 2-0 Stratafix® barbed suture to close the peritoneum. 8. Video--Chapter 8, “Sacral Dissection”: A peritoneal tunnel is created to cover the mesh, but many surgeons prefer to open the peritoneum and simply close the retroperitoneum at the end. The mesh is passed through the tunnel before dissecting out the ligamentum flavum, which covers the sacral promontory. The sacral promontory is exposed by retracting the sigmoid colon medially and incising the peritoneum over the sacrum. 9. Video--Chapter 9, “Secure Mesh to Sacrum”: Interrupted sutures of 0-Prolene are used to fix the mesh, it is important to clear the promontory completely so the mesh adheres to the ligamentum flavum (anterior longitudinal ligament). The structures to be aware of include middle sacral vein, often medial and running cranial–caudal, right ureter, left common iliac vein (if one is extremely cephalad), and branches of hypogastric veins and arteries (if one is extremely caudad). Diskitis has been described when sutures are anchored in the intervertebral disk, and osteomyelitis has also been described.
10,11
10. Video--Chapter 10, “Close Peritoneum”: The peritoneum is reapproximated to cover the mesh using a running absorbable suture. The authors prefer barbed suture. 11. Video--Chapter 11, “Remove Needles and Close Ports”: If a hysterectomy is performed, this can be removed using the 10 cm Endo-Catch® bag and either morcellated or removed intact through a small extension of the umbilical port.

Bed-mounted vaginal retractor before anchoring to bed.

Bed-mounted vaginal retractor after being anchored to bed.
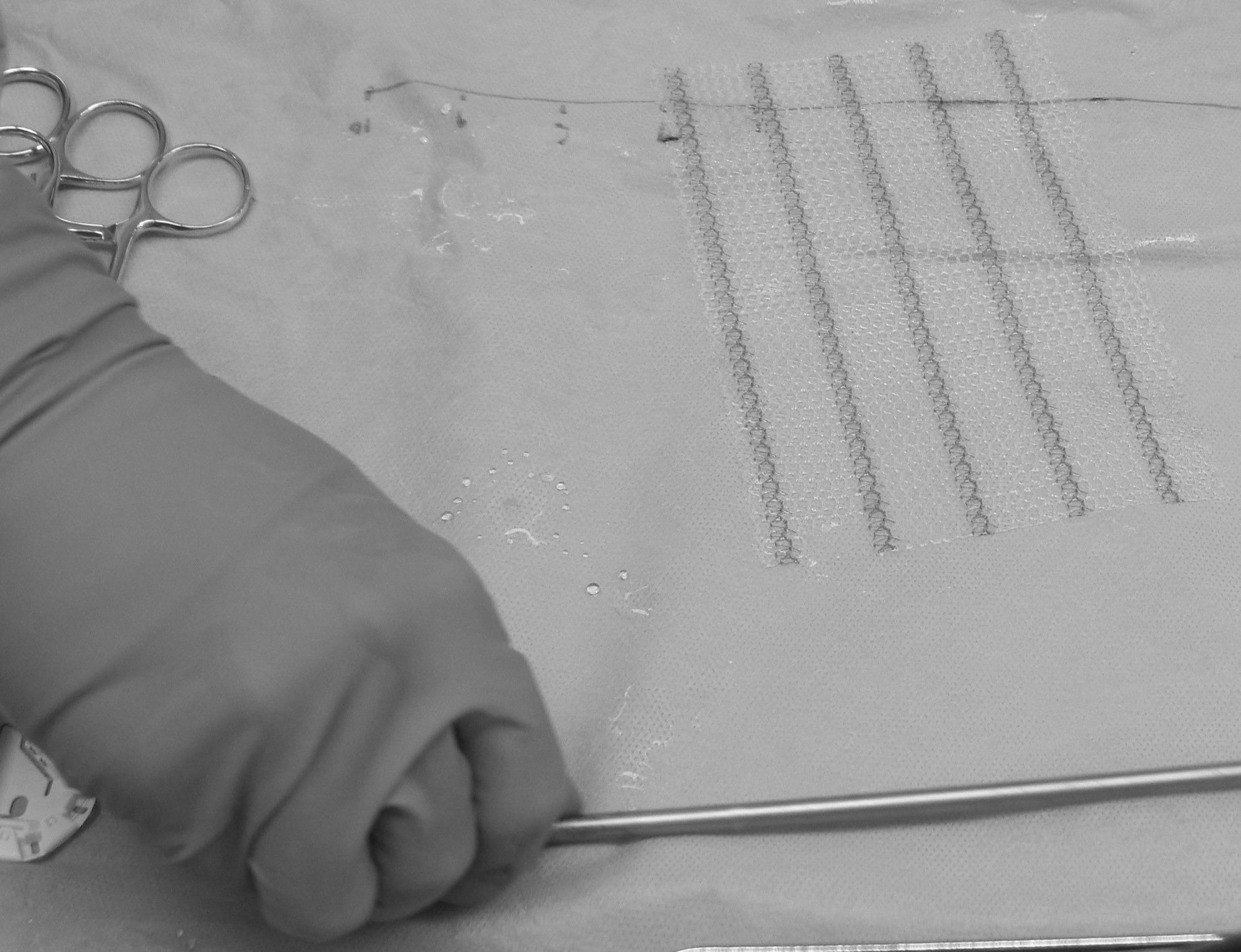
Uncut type 1 macroporous polypropylene mesh sutured to the anterior vaginal wall, posterior vaginal wall, and anchored to the sacrum.
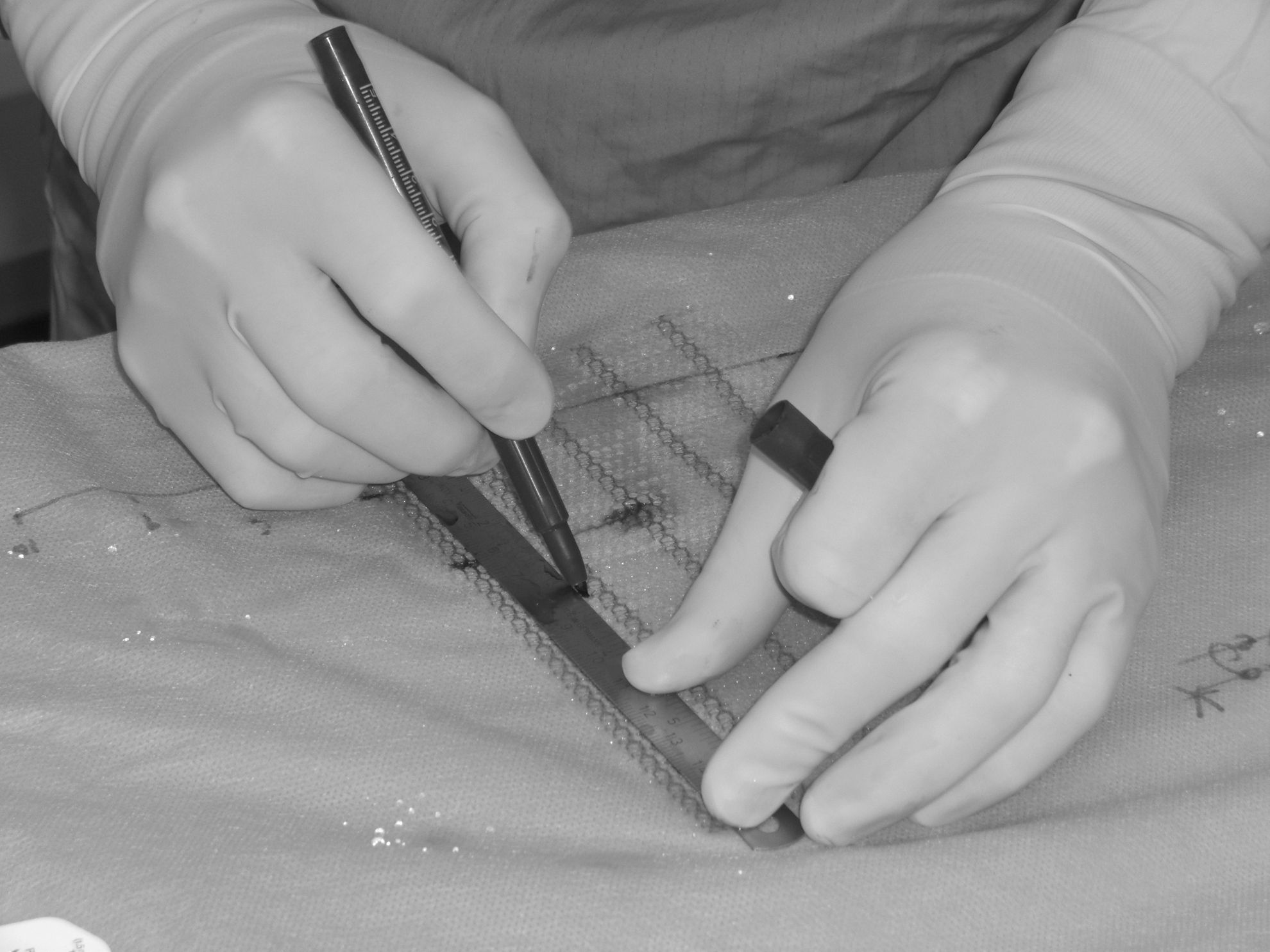
Measuring the mesh based on individual patient specifications.

Y-mesh has now been cut and is ready to be passed into the body.

Harvest site and harvested fascia lata, right leg is demonstrated here, lateral aspect carries the highest quality fascia. Although the skin and fat are closed, the fascia lata does not require closure.
Postoperative Care
Patients are encouraged to ambulate on postoperative day 0 the evening of the surgery. Clear diet is started and advanced as the patient tolerates. Vaginal packing with estrogen-impregnated gauze is left overnight, as is a Foley urinary catheter. A history of breast cancer is a relative contraindication to estrogen cream and bacitracin ointment can be used in its place. Foley and packing are removed in the morning on postoperative day 1. Patients who undergo concomitant midurethral sling or Burch colposuspension are given a voiding trial and, if unable to void, or able to void with an elevated postvoid residual >150 mL, are taught to perform clean intermittent catheterization and instructed to perform this twice daily until the 2 week follow-up visit. Complete blood count is taken on postoperative day 1 to detect occult bleeding. Since mobilization of the bowel is generally necessary for patients who have undergone prior surgery, suspicion for occult laparoscopic bowel injury is high. In general, patients are discharged on postoperative day 1.
Troubleshooting
Many potential pitfalls and complications exist. The most common, De-novo stress urinary incontinence (SUI) occurs with open sacral colpopexy as well. Commonly, women who present without preoperative complaints of SUI will develop it postoperatively. A 40% rate of de-novo SUI was documented in the colpopexy and urinary reduction effort (CARE) trial using the open approach to sacral colopexy, 12 and the Indiana series reflects this with a 34% rate. Our practice is to counsel all patients about this possibility, offer a sling at the time of RASC but encourage waiting for those with no preoperative incontinence, and plan for a delayed sling 6 weeks postoperatively if bothersome incontinence develops. Mesh exposure and suture extrusion events are also possible, and good preoperative counseling is necessary. Some exposures are asymptomatic and some require limited mesh excision and closure of the vaginal defect in the operating room. Apart from the standard laparoscopic complications, crepitus extending as far as the face and eyes can be seen after RASC, and although not life threatening or permanently damaging, prompt attention must be given to the patient to reassure her that it will resolve with no permanent damage. When 12-mm assistant ports placed in the midaxillary line are closed, there is a possibility of port site pain, which the surgeon should be aware of. Bladder injury and vaginal injury during dissection can be managed by immediate closure with a braided absorbable suture and are not a contraindication to using mesh, in the opinion of the authors. Bowel injury at the time of surgery, in contrast, is a contraindication to proceeding with mesh. Porcine dermis has been used safely in a similar situation by the authors when an elective colostomy takedown was combined with sacral colpopexy. Bleeding during sacral dissection is a potentially troubling complication, and with the open approach, this sacral bleeding can rapidly obscure the operative field. If a significant injury to the middle sacral vein is noted, the bleeding can be slowed by temporarily increasing CO2 insufflation pressure from 15 to 20 mm Hg. If the mesh and permanent monofilament suture used to anchor the tail of the mesh to the sacrum are in position, simply securing the mesh to the sacrum over the bleeding area can often tamponade the bleeding. This is not advisable for arterial bleeding, however. The PK Dissector or bipolar cautery can often control small arteries.
Alternative Approaches/Modifications
Many alternative approaches to RASC have been described. Original descriptions of the procedure involved multiple interrupted permanent monofilament sutures to secure the mesh. 13 The authors now use a running technique to save time, as demonstrated in the video, and have not noted any decline in success rates. Moreover, delayed absorbable monofilament suture is now used to secure mesh without a decline in success. Many reports do not detail how far the anterior and posterior dissections are carried, but some early reports described supporting only the apex of the vagina, dramatically reducing operative time, but often secondary or concomitant compartment-specific procedures were required. Uterine-sparing procedures have also been described, citing patient preference as the reason for keeping the uterus. 14
Outcomes
POP-Q examination was performed and recorded preoperatively and postoperatively on every patient. Treatment failure was defined as recurrent apical prolapse >2 cm or any leading edge beyond the hymen (Ba = 0 or Bp = 0). Surgical outcomes can be monitored with POP-Q examination, and validated quality of life (QoL) instruments such as UDI-6, Likert QoL, and IIQ-7.
Results
A total of 119 consecutive women underwent RASC between 2009 and 2016. Pre- and postoperative characteristics were noted (Table 1). Of them, 53 had undergone prior hysterectomy, 15 had undergone prior vaginal prolapse repair, and 8 had undergone prior incontinence procedures. Many patients underwent concomitant procedures at the time of colpopexy. A total of 66 underwent robotic supracervical or total hysterectomy, 34 underwent midurethral sling at the time of colpopexy, 22 underwent culdoplasty for enterocele, and 5 underwent concomitant anterior vaginal wall suspension. All POP-Q, UDI-6, and QoL scores improved postoperatively (Table 1). Apical failure was noted in 0, anterior failure was noted in 7 (average Ba +1.1 cm in failures), and posterior failure was noted in 4 (mean Bp +1.0 cm) at 15.6 months mean follow-up.
Preoperative and Postoperative Results After Robot-Assisted Sacral Colpopexy, Mean Follow-Up 15.6 Months
Continuous variables are reported as mean ± standard deviation, analyzed with Students two-tailed t-test. Failure was by POP-Q examination, 2 cm apical descent, or any compartment leading edge beyond the Hymen.
NS = not statistically significant; POP-Q = pelvic organ prolapse quantification; QoL = quality of life; TVL = total vaginal length.
Eleven of 119 patients were noted to have suture erosion (9.2%). Postoperative UDI-6, QoL, and IIQ-7 scores improved after surgery (Table 1). Complications included two wound infections managed with antibiotics (Clavien–Dindo classification Grade II 15 ) and two vaginal mesh erosions, as well as one prolonged intubation who was effectively extubated on Post Operative Day 2 for respiratory compromise thought to be because of untreated hiatal hernia and advanced age (92 years). One new-onset episode of atrial fibrillation was also noted. Three port site hernias were noted postoperatively, all occurred at the 12 mm port site, one required operative intervention (Clavien–Dindo classification Grade IIIb), and the remaining two were managed nonoperatively. One of the vaginal mesh erosion events occurred after total hysterectomy at the time of colpopexy, managed with operative intervention (Clavien–Dindo classification Grade IIIb). The other patient had undergone prior hysterectomy, had no recognized vaginotomy or opening in the vagina, and was asymptomatic and chose nonoperative management (Clavien I).
Conclusions
RASC has outcomes comparable to published series describing the open and laparoscopic approaches and can be described in 11 steps as depicted in the accompanying video. (Supplementary Data are available online at
Recommended Videos from Videourology
1. Videourology Aug 2012
Robotic Laparoendoscopic Single-Site Sacrocolpopexy
Benjamin E. Dillon, Jeffrey A. Cadeddu, Philippe E. Zimmern
2. Videourology. Feb 2014
Robotic Sacrocolpopexy: Salvage Procedure After Failed Open SacrocolpopexyCarey Robert I., Pilkington James E., Blau Elliot K., and Martin Christopher J
Footnotes
Author Disclosure Statement
Investigator Astellas, Inc. —Powell.