
Abstract
Objective:
To assess the frequency of minimally invasive radical cystectomy (MIRC) conversion to open surgery, what factors influence conversion, whether or not the benefits of MIRC vs open radical cystectomy (ORC) persist after conversion, and compare ORC and MIRC outcomes.
Materials and Methods:
We performed a retrospective cohort study from the National Cancer Data Base (2010 to 2013) analyzing patients who underwent completed MIRC (n = 5750), converted MIRC (n = 245), and ORC (n = 12,053) without prior radiotherapy. Multivariable logistic and linear regression analyses were used to assess the association between covariates, open conversion as well as surgical approach, and secondary outcomes such as positive surgical margins (PSMs), use of lymphadenectomy, lymph node yield, hospital length of stay (LOS), and 30-day readmission.
Results:
Rates of conversion were independent of patient factors such as race, sex, use of neoadjuvant chemotherapy, and clinical stage. Conversion occurred in 245 of 5750 MIRCs (4.3%) and declined over time (5.8% in 2010 vs 3.2% in 2013, odds ratio [OR] 0.50, 95% confidence interval [CI] 0.34–0.75, p = 0.001). MIRC was associated with fewer positive margins, higher lymph node yield, shorter LOS, and fewer readmissions compared with ORC, however, patients requiring open conversion had longer median hospital stays (8 days vs 7 days, p = 0.013), lower median lymph node yields (14 vs 17, p = 0.007), more PSMs (17% vs 11%, p = 0.006), and more 30-day readmissions (14% vs 9%, p = 0.008) compared to nonconverted. Converted MIRC had similar hospital LOS and 30-day readmission rates compared to ORC.
Conclusion:
Open conversion during MIRC is uncommon and has decreased in recent years despite the rising use of MIRC. MIRC had better short-term outcomes compared with ORC. These benefits were negated with open conversion; however, outcomes were similar compared to planned ORC.
Introduction
O
Unique to minimally invasive approaches is the need for open conversion in challenging scenarios. Systematic reviews of MIRC highlight perioperative outcomes, diversion type, and oncologic outcomes such as survival, node status, and positive surgical margins (PSMs), but have not described the impact of open conversion on outcomes. 3,9 –12 A recent early-phase, randomized, prospective three-arm trial of 60 patients comparing ORC, LRC, and RRC reported a conversion rate of 5% from RRC to ORC and 5.3% from LRC to ORC. 13 In addition, the trend of significant increase in surgical margins during RRC was recently reported in a randomized controlled trial. 14 There are also minimal data on risk factors for MIRC open conversion, but difficult dissection, large tumor size, and equipment failure have been cited as reasons for conversion. 13,15
Given the increasing popularity of MIRC and potentially unclear consequences of open conversion, 16 we sought to evaluate the frequency of MIRC conversion to open, what factors influence conversion, and whether or not the benefits inherent to a minimally invasive approach persist after conversion using a contemporary cohort from the National Cancer Data Base (NCDB).
Materials and Methods
Patients
We queried the NCDB bladder cancer participant user file, an oncology dataset comprised >1500 treatment facilities accredited by the American College of Surgeons and the American Cancer Society Commission on Cancer. 17 Our study population included all patients diagnosed with bladder cancer between 2004 and 2013, who underwent radical cystectomy with no prior radiation therapy (n = 28,997). The study years were chosen based on when the surgical approach variable was available in the NCDB. We excluded patients with missing data on surgical approach for a total of n = 17,803 included for analysis.
Covariates
Covariates were selected a priori for multivariable analyses. Patient characteristics included age, sex, year of diagnosis, race, insurance type, and Charlson Comorbidity index. 18 Patient home distance from treatment facility was calculated based on zip codes. Treatment facility characteristics included regional location within the United States and facility type, which are based on the number of cancer patients encountered each year, community (>100), comprehensive (>500), and academic (>500), and offer graduate medical training programs.
We also assessed the effect of cancer stage at diagnoses on our primary outcome, which we categorized using the American Joint Committee on Cancer grouping.
Although the coding in the NCDB includes type of urinary diversion, this was only recorded for about 56% of patients in our final cohort. About 90% of these patients received an ileal conduit and the descriptions for the other types of diversions were not specific enough for meaningful analysis.
Outcomes
Our primary outcome was MIRC conversion rate to open surgery. Secondary outcomes included PSM, 30-day readmission following discharge after surgery, use of lymphadenectomy, lymph node yield, and length of hospital stay (LOS) following surgery.
Statistical analyses
To compare short-term outcomes between surgical approaches and conversion cases, we used Pearson's chi-squared and Mann–Whitney U analyses. To assess the association between covariates and the odds of MIRC open conversion, we used multivariable logistic regression to calculate odds ratios (ORs). Both multivariable logistic and linear regressions were used to assess the association between open conversion and secondary outcomes. All statistical tests were performed using Stata 13.0 (College Station, TX), all t-tests were two-tailed, and significance was determined by p-values <0.05.
Results
Factors affecting conversion of MIRC
There were 5750 MIRCs and 12,053 ORCs registered in the NCDB between 2004 and 2013. Over the study period, the percentage of patients receiving ORC decreased from 74% to 64%, while MIRC increased from 26% to 36% (Fig. 1). A total of 245 (4.3%) MIRCs were converted to open (c-MIRC; Table 1). There was no difference in conversion rate of MIRC performed by gender (4.7% of females and 4.1% of males) or race (white and African American patients were converted 4.2% and 4.4% of the time). Importantly, the rate of conversion was not affected by clinical stage as 3.6% of patients with stage I, 4.4% of patients with stage II, and 4.4% of patients with stage III-IV were converted to open cystectomy. While we found no patient-specific factors associated with open conversion, the year of treatment was significantly associated with conversion as MIRC conversions decreased continuously over time from 5.8% in 2010 to 3.2% in 2013. Multivariable analysis of race, age, sex, use of neoadjuvant chemotherapy, and facility annual radical cystectomy volume was not significantly associated with odds of conversion (all p > 0.05; Table 2), while year of surgery was the only parameter predicting c-MIRC (OR 0.50, 95% confidence interval [CI] 0.34–0.75, p = 0.001; Table 3). These data suggest that patient-specific factors were not predictors of open conversion.
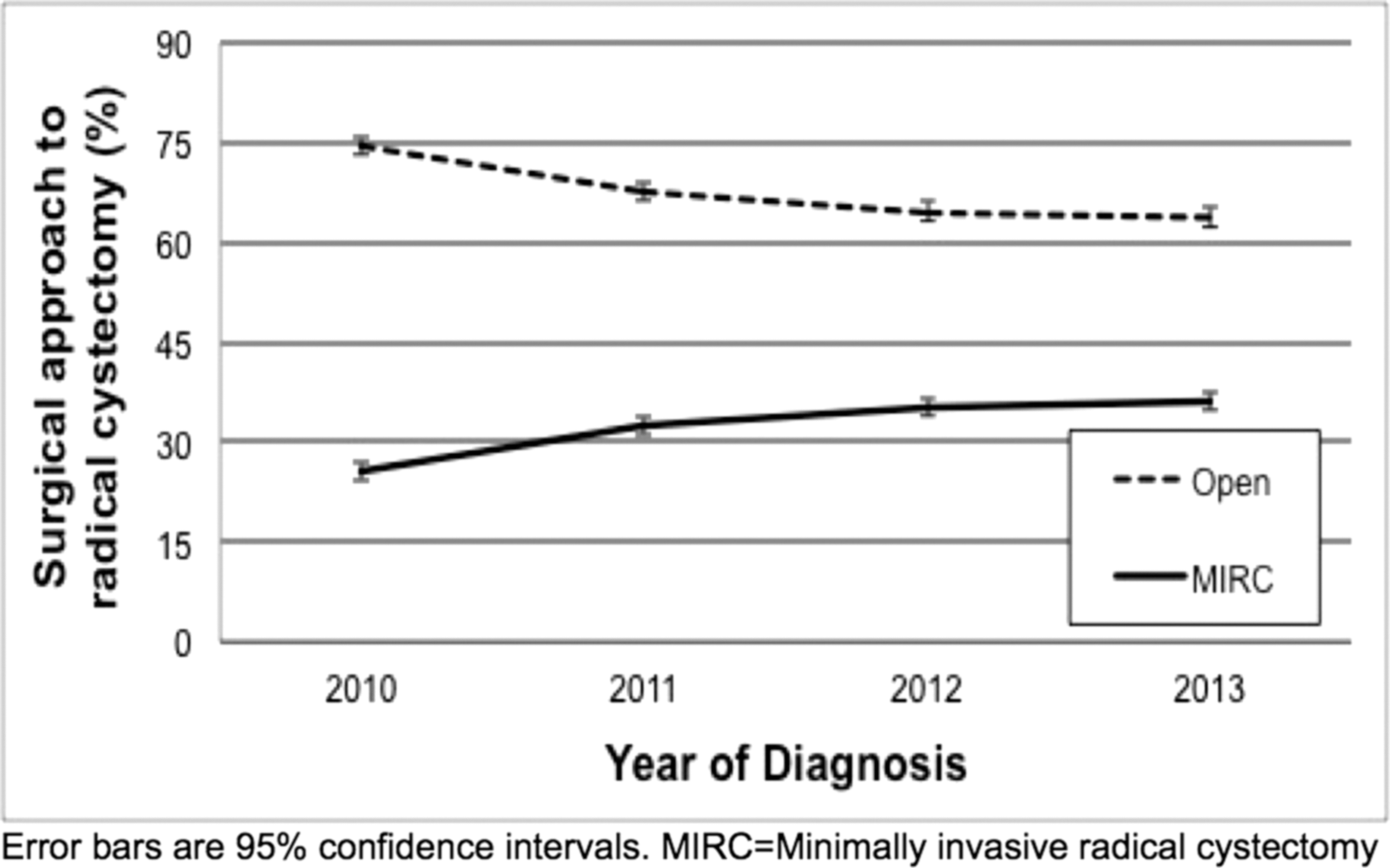
Temporal trends in radical cystectomy surgical approach.
IQR = interquartile range; MIRC = minimally invasive radical cystectomy; NMIBC = nonmuscle invasive bladder cancer.
Bold value indicates statistical significance with p < 0.05.
CI = confidence interval; OR = odds ratio.
Pearson's Chi-squared analyses were used to compare dichotomous outcomes while Mann–Whitney U analyses were used to compare median values. Bold value indicates statistical significance with p < 0.05.
PSM = positive surgical margin.
Surgical margin status and morbidity of conversion
We next investigated whether conversion of MIRC to ORC had an impact on margin status. Since margin status has a strong correlation with survival, we evaluated the margin rates of MIRC compared with c-MIRC and found that c-MIRC cases had higher rates of PSM (16.5% vs 10.8%, p = 0.006; Table 2). In addition to margins, we investigated other parameters associated with surgical quality (lymph node yield) and surgical morbidity (LOS and rates of readmission). Compared with MIRC, c-MIRC was associated with increased frequency of 30-day readmissions (14.4% vs 9.3%, p = 0.008), decreased median node yield upon node dissection (14 vs 17, p = 0.007), and increased median LOS following surgery (8 vs 7, p = 0.013). There was no difference in rate of lymphadenectomy between MIRC and c-MIRC (89% vs 90%, p = 0.7).
Since MIRC is relatively a new technology, ORC remains the “gold standard.” We compared MIRC and c-MIRC to ORC. Compared with MIRC, ORC cases had higher rates of PSM (13.1% vs 10.8%, p < 0.001), increased use of lymphadenectomy (91% vs 89%, p < 0.001), decreased median node yield (13 vs 17, p < 0.001), increased median LOS following surgery (8 vs 7, p < 0.001), and increased rates of 30 day readmissions (11% vs 9%, p = 0.001). When c-MIRC was compared with ORC, we found no statistically significant differences in PSM, 30-day readmissions, rates of lymphadenectomy, nodal yield, or hospital LOS (all p > 0.09), suggesting that converted MIRC has similar outcomes compared with planned ORC.
We hypothesized a difference in margin rate between MIRC vs ORC as one benefit of open surgery is the tactile appreciation of bulky tumor. Therefore, margin rates were stratified by clinical stage. There were no statistically significant differences in PSM between c-MIRC and nonconverted MIRC or ORC by stage. Compared to planned ORC, MIRC had similar rates of PSM for stage I (7.9% vs 7.6%, p = 0.8; Table 2), higher rates for stage II (12.5% vs 10.3%, p = 0.036), and lower rates for stage III-IV disease (18.5% vs 22.6%, p = 0.011), suggesting that tumor bulk was not a cause for conversion. Unfortunately, NCDB does not delineate the specific location of the margin (i.e., positive soft tissue vs urothelial margin), which has oncologic prognostic implications.
Multivariable analysis controlling for multiple patient and clinical covariates was performed and c-MIRC was not associated with more PSM compared to nonconversion (OR 1.46, 95% CI 0.98–2.18, p = 0.064; Supplementary Table S1; Supplementary Data are available online at
Discussion
MIRC for MIBC has been increasingly described over time. 3,19 However, the open conversion rate in MIRC is not well reported in large systematic reviews, and there are no epidemiologic studies on this subject. 9,10 In single institutional series, conversion rates are noted to range widely from as low as 0% to 15.4% for all-comers. 4,5,7,12,13,20 Furthermore, the risk factors for open conversion and the impact of conversion on patient outcomes are unclear. We found in a national cohort of patients who underwent radical cystectomy, open conversion rate of MIRC in the United States is low at 4.3% and open conversion rates decreased from 2010 to 2013. Race, sex, clinical stage, and use of neoadjuvant chemotherapy did not affect conversion rates.
Open conversion has declined over time
As laparoscopic radical cystectomy gained attention for bladder cancer in the late 1990s to early 2000s and Menon and colleagues described the first robotic series in 2003, there has been a surge of literature and interest dedicated toward MIRC. 2,21,22 Open conversion in MIRC was less likely to occur in the more recent years of this study as the proportion of MIRCs conversions decreased by nearly half from 2010 to 2013. This may reflect growing surgeon experience with MIRC, a trend commonly seen. From the International Robotic Cystectomy Consortium (IRCC) data, the learning curve for RRC was only 30 cases to achieve acceptable proficiency using proxy measures (estimated blood loss, lymph node yield, transfusion rate, and PSM). 21 As MIRC use in the United States continues to increase as seen in the NCDB, it is likely that the conversion rate to open will continue to decline.
Open conversion may worsen operative outcomes but is comparable to open surgery
To our knowledge, the impact of open conversion in MIRC with regard to patient outcomes such as hospital stay and oncologic outcomes is not well described. Reported PSM rates range from zero in small, institutional series to as high as 28% in studies with patients having advanced disease. 9 SWOG 8710 (Southwest Oncology Group) reported a 10% PSMs rate in ORC. 23 We found a higher percentage of PSM in open conversion compared with nonconverted cases (17% vs 11%) and no difference between converted and ORC cases (13%).
Notably, when stratified by clinical stage, PSM rates varied between ORC and nonconverted MIRC. In multivariable analysis, ORC was associated with increased odds of PSM compared with nonconverted MIRC. Conversion did not significantly affect margin status in this analysis. Previous data have suggested no difference in margin status when comparing ORC to MIRC. 13 However, given a PSM may more than double the risk of metastatic disease, and the risk of death from bladder cancer, 24 margin status, and type of margin should be further scrutinized as data from randomized clinical trials comparing ORC and MIRC matures.
Median LOS for ORC and MIRC has been reported at around 7 to 9 days. 4,8,11,12 One purported benefit of MIRC is reduced convalescence, which our data support. We found that national median hospital stay for ORC and MIRC was comparable to the range reported in the literature. Although modest, a shorter LOS of 1 day was seen in MIRC cases compared with that of ORC and c-MIRC, and this trend was consistent upon multivariable analysis. Generally, LOS following surgery may be considered a proxy for relative level of complicated postoperative course. This may be considered true for 30-day readmissions as well, and accordingly, both converted MIRC and ORC were associated with more 30-day readmissions following discharge.
The rate of lymphadenectomy for radical cystectomy has increased in recent years and improves cancer-specific survival. 25 We found ORC had a slightly higher rate of lymphadenectomy compared with that of MIRC with omission of lymphadenectomy in only about 10% of cases, similar to the rate seen in previous work. 24 A wide range for the number of lymph nodes removed has been reported in the literature, however, the yield rates may be higher in MIRC 26 and a higher yield may improve cancer-specific survival. 27 When MIRC cases were converted, the median lymph node yield decreased in the NCDB.
Our data also demonstrated lymph node yields are increased in completed MIRC cases compared with ORC. However, this finding should be interpreted with caution given the handling of lymph nodes with robotic trocars often means lymph nodes are extracted in more packets, which may surreptitiously increase the number of exclusive nodes assessed by pathologists without a uniform system of processing of lymph nodes, which may vary greatly from institution to institution.
Study limitations and strengths
There are several important limitations to our study that must be considered when interpreting our results. Certain factors such as body mass index and reason for conversion were not reported in NCDB and other confounding factors, including better patient selection or institutional protocols, may exist and could contribute to the decreased conversion rate with time. The retrospective nature of this analysis and the inherent selection bias may limit definitive conclusions, especially in the setting of absent widespread enhanced recovery protocols (ERAS) for ORC during the time of this dataset. We also could not discern the use of extra vs intracorporeal diversions or laparoscopic vs robotic-assisted MIRC in this dataset, which may confound reported outcomes as retrospective data have suggested slightly lower complication rates and gastrointestinal side effects in the intracorporeal group, however, the learning curve for intracorporeal diversion as well as pure LRC remains steep and adds to operative time. 19,28,29 In addition, we could not control for individual surgical volume and evaluated volume based on facility radical cystectomy volume relative to each facility within the current study. Finally, NCDB may not accurately capture all 30-day readmissions, as our ORC readmission rate of 11% is lower than contemporary reported single-institution rates, but MIRC readmission rates may be under captured as well. 30
Strengths include the large size of our cohort and its general well-rounded representation of the four major regions of the United States (each of the regions comprised 19%–30% of the total patients) as well as the availability of other epidemiologic data from NCDB regarding MIRC. To our knowledge, this is the largest study to date reporting MIRC conversion rates, associated factors, and outcomes.
Conclusion
Few MIRCs are converted to open, and conversion rates for MIRC have declined in recent years, perhaps reflecting improvement in minimally invasive skills. Nonconverted MIRC was associated with modestly shorter hospital stays, fewer 30-day readmissions, increased lymph node yields, and fewer PSMs compared to converted MIRC and ORC. Our results are limited mainly by the retrospective nature of this study, but suggest that the purported benefits of MIRC may be negated when converted to open; however, overall outcomes in conversion are comparable to planned open surgery.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.