
Abstract
Introduction:
In Western countries about 25% of prostate cancer (PCa) are high-risk tumors at presentation and its treatment is still a matter of debate among urologists. When a surgical approach is preferred the use of a mininvasive tecnique is still difficult due to the lack of data supporting it in literature. The aim of this study is to evaluate feasibility and safety of laparoscopic radical prostatectomy (LRP) for high-risk PCa.
Materials and Methods:
The study included 1114 patients with high-risk PCa submitted to LRP between 1998 and 2014. High-risk patients were defined according to D'Amico classification. We collected functional and oncological long-term outcomes and evaluated with univariate and multivariate analyses the role of predictive factors for survival and biochemical recurrence (BR).
Results:
Mean age at treatment was 62 ± 8 years; mean follow-up was 74 ± 50 months. We obtained an overall survival (OS) of 96.6% at a mean follow-up of 74 months (1076 patients) and a disease-free survival of 66.2% (737 patients). Age (p = 0.0006), pT (p < 0.0001), pN (p = 0.0018), and surgical margins (p = 0.0076) resulted as independent predictors for BR in multivariate analysis. pN (p = 0.0025) and Gs (p = 0.0003) are independent predictors for OS and cancer-specific survival in a univariate analysis; just the Gs results significant in the multivariate model.
Conclusions:
According to our encouraging data about oncological and functional outcomes we believe that radical prostatectomy represents an effective treatment for patients with high-risk PCa and that laparoscopy is a safe approach offering a mini-invasive alternative to open surgery.
Introduction
D
Laparoscopic radical prostatectomy (LRP) was introduced in the late 1990s, but to date only few series have shown long-term oncological results of this surgical approach and, moreover, this information is lacking especially in patients with high-risk disease. The importance of pure laparoscopic procedures is nowadays to underline in literature in order to encourage the use of mininvasive procedures in hospital that cannot afford a robot.
The aim of our study is to evaluate the feasibility and safety of LRP in terms of intra- and postoperative complications and long-term oncological and functional results.
Materials and Methods
Patient population
The study included 1114 consecutive patients with high-risk PCa who underwent LRP between May 1998 and May 2014 in 3 European Institutions: Henri Mondor University Hospital, Creteil, France (428 patients), SLK Clinic, Heilbronn, Germany (421 patients), and L. Sacco Hospital, Milan, Italy (265 patients). High-risk patients were defined according to D'Amico classification: PSA >20 ng/mL and/or Gleason score ≥8 and/or clinical stage > T2c.
PSA value was always measured before the prostate biopsy. Clinical stage was assigned before surgery. Pathologic grading was assessed according to the Gleason system and clinical stage was assigned according to the 2002 TNM system. 1 Patient's staging were performed according to EAU guidelinies with CT scan, prostatic magnetic resonance and/or bone scan. 1
Surgical procedure
All the procedures were performed transperitoneally by expert surgeons who already accomplished their learning curve in LRP.
Lymphadenectomy was performed according to the EAU guidelines indications at the moment of surgery; in most recent cases extended pelvic lymph node dissection (ePLND) was performed if the estimated risk for positive LNs exceeded 5%. 1
Data on limphadenectomy are available for 1022 patients (91.7%) due to the retrospective nature of the study; most of the pNx patients underwent surgery in the late 1990s when guidelines about this procedure were still evolving. Lymphadenectomy is performed before or after prostatectomy depending on surgeon habits. If performed after it, lymphadenectomy is always performed before the vescico-urethral anastomosis to allow better mobilization of the bladder without damaging the anastomosis. We always use a transperitoneal approach to minimize the risk of postoperative lymphocele formation.
Templates for standard dissection was the same in all the centers including obturator and external iliac nodes.
Due to the retrospective nature of the study and the variable definition of ePLND in literature the exact borders of the dissection is not always standardized in all the centers; all the procedures included obturator, external iliac and internal iliac nodes but not clear data are available about presacral, common iliac, and presciatic nodes.
Postoperative evaluation
The Clavien-Dindo complications grading system was used to evaluate intra- and perioperative complications. Postoperative follow-up included digital rectal examination and serum PSA and was scheduled according to the scheme proposed by EAU PCa guidelines. 1 A telephonic update was realized in September 2014 for all patients. Biochemical recurrence (BR) was defined as two consecutive PSA values >0.2 ng/mL.
Overall survival (OS) was defined as the number of alive patients at last follow-up. Cancer-specific survival (CSS) was defined as the number of patients alive after excluding deaths for other causes. Disease-free survival (DFS) was defined as no evidence of BR at last follow-up.
Urinary incontinence was evaluated in all patients and continence was defined as the use of 0 pads. We did not evaluate potency due to the risk characteristics of our population that exclude a nerve sparing approach according to the EAU guidelines; this decision was in 1998 and is still adherent to the guidelines where no specific recommendations for high-risk tumor is made. 1
Statistical analysis
Categorical variables are reported as count (percentage), continuous variables are reported as mean ± standard deviation or median (range), as appropriate.
Kaplan–Meier analyses were used for the estimation of survival curves, considering BR, cancer-specific and all-cause mortality as the events of interest respectively. The log-rank test was used for comparison of survival curves between groups of patients.
Subsequently, univariate and multivariate Cox regression analyses were performed to establish the predictors of outcomes. Covariates were age, preoperative PSA, pathological Gleason score, surgical margins status, use of lymphadenectomy, pT, and pN. Only those predictors that resulted significant in univariate analysis were introduced in the multivariate model. Thereafter, a backward elimination procedure was used to find the optimal predictive models. This set of analyses was performed for both BR and cancer-specific mortality. For all the fitted Cox models, the proportional hazard assumption was checked. Hazard ratios, with their 95% confidence intervals, were derived from the Cox models.
p-Values <0.05, two sided, were considered statistically significant. All the statistical analyses were performed with SAS statistical software (release 9.4; SAS Institute, Inc., Cary, NC).
Results
Patients characteristics, preoperative PSA, clinical stage, and bioptic Gleason score are reported in Table 1.
PSA = prostate specific antigen.
Complications
Table 2 reports all the complications classified according to Clavien Dindo and respective treatments. 7 Overall 180 patients (16.2%) presented a total of 186 complications. Blood transfusions represented the most common postoperative complication, a total of 132 cases (11.8%). Excluding transfusions, number of patients with perioperative complications decreased to 54 patients (4.8%).
ePLND = extended pelvic lymph node dissection; stPLND = standard lymphadenectomy.
The 11 patients presenting symptomatic lymphocele underwent percutaneous drainage.
Ten patients presented urethral stenosis at different point of follow-up; six of them underwent adjuvant radiotherapy.
The overall complication rates were similar in patients undergoing ePLND, standard PLND (stPLND), and no PLND (15.8% vs 17.2% vs 16.1, p = 0.412).
Oncological and functional outcomes
Mean follow-up time was 74 ± 50 months.
In Table 2 are reported pathological results after LRP. There were 296 patients (26.6%) with pT2 tumor, 769 (69%) with pT3 tumor including 348 (31.2%) cases of seminal vescicle invasion (pT3b); pT4 stage is reported in 49 cases (4.4%). One hundred eighteen patients (10.6%) presented positive nodes and 383 (34.4%) positive surgical margins. Most of the tumors (61.6%) resulted with a Gleason score ≤7. We obtained an OS of 96.6% at a mean follow-up of 74 months (1076 patients) and a DFS of 66.2% (737 patients).
The mean (SD) overall lymph node yield was 18.5 (5.7).
Seven hundred eighty-one patients (76.4%) underwent ePLND with a node yield of 19.1; 241 patients (23.6%) underwent stPLND with a node yield of 15.6. In Table 2 are shown pathologic data according to standard and extended procedures.
In Table 3 is reported survival results stratified for stage, relapse, and adjuvant treatment.
Values are represented by n (%).
Patients with biochemical recurrence and patients with persistent disease after surgery.
Seventy-five patients (6.7%) presented disease persistence after surgery and are now alive and free of disease. Most of these patients (54) had a pT3 tumor; 17 a pT2 and just 4 a pT4. Five hundred thirty-six patients (48.1%) had a biochemical recurrence followed by adjuvant therapy; 527 (98.3%) are still alive; 6 (1.1%) died of the tumor and 3 (0.6%) of other causes. Five hundred patients (44.9%) did not receive any adjuvant treatment; most of them had a pT3 tumor (327), 155 had a pT2, and 18 a pT4. Four hundred seventy-two (94.4%) are still alive; 14 (2.8%) died due to the tumor and 14 (2.8%) due to other causes. As reported in Table 4 age (p = 0.0006), pT (p < 0.0001), pN (p = 0.0018), and surgical margins (p = 0.0076) resulted as independent predictors for BR in multivariate analysis.
Reference category.
CI = confidence interval; HR = hazard ratio; BR = biochemical recurrence.
Figures 1 to 5 show survival curves with Kaplan–Meier model for DFS. Table 5 identifies pN (p = 0.0025) and Gs (p = 0.0003) as independent predictors for OS and CSS in a univariate analysis; just the Gs results significant in the multivariate model.
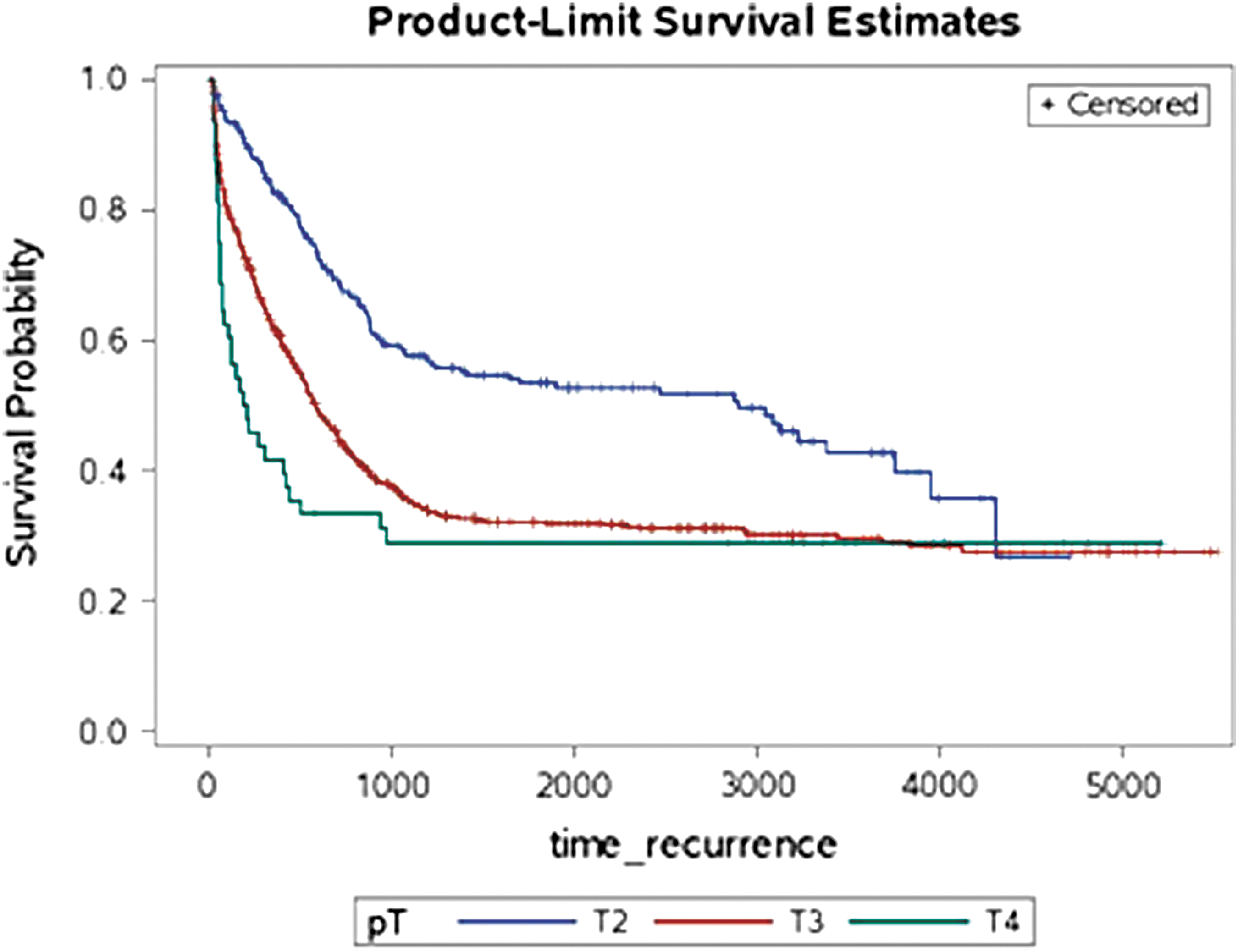
Pathological T.
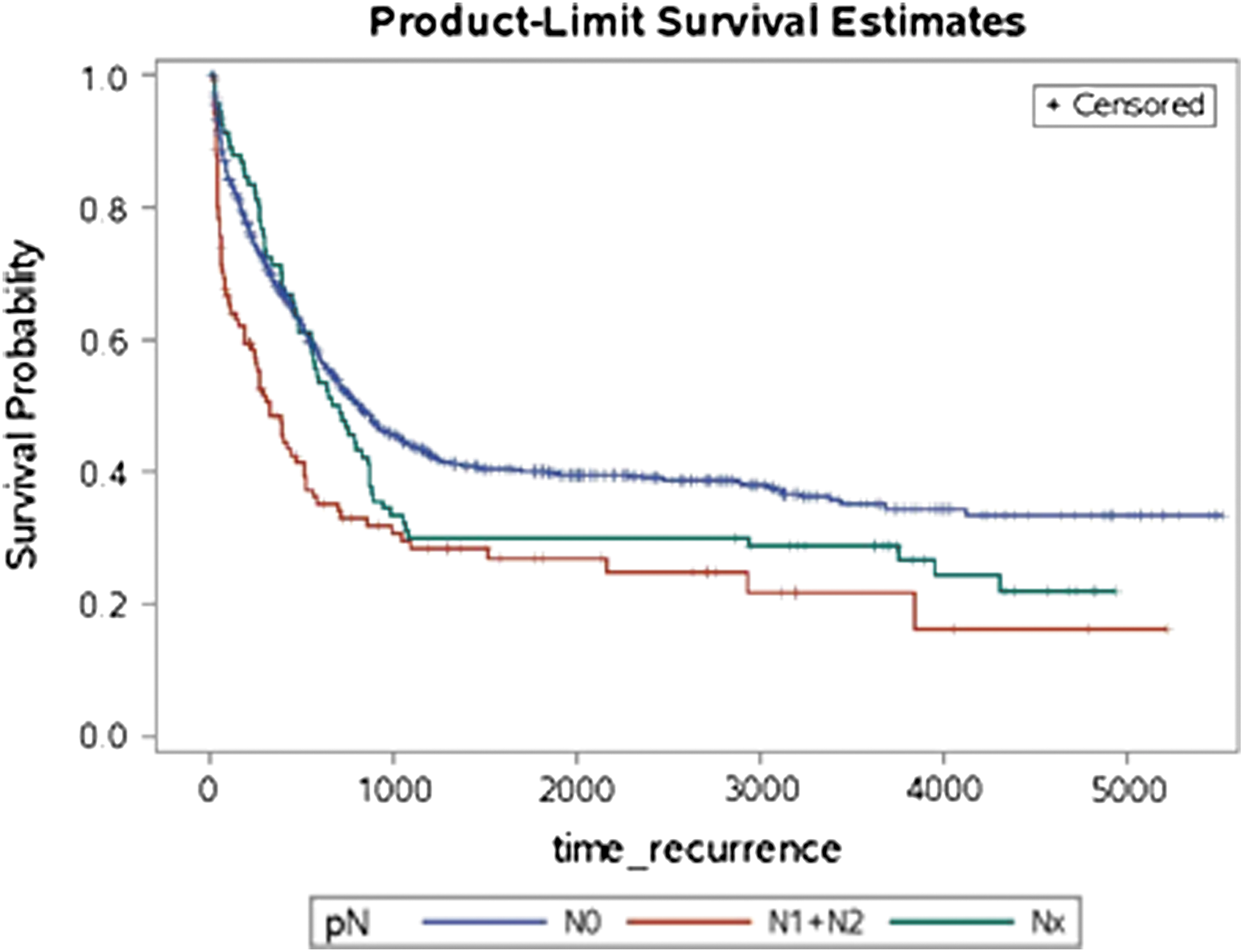
Pathological N.

Pathological Gleason score.
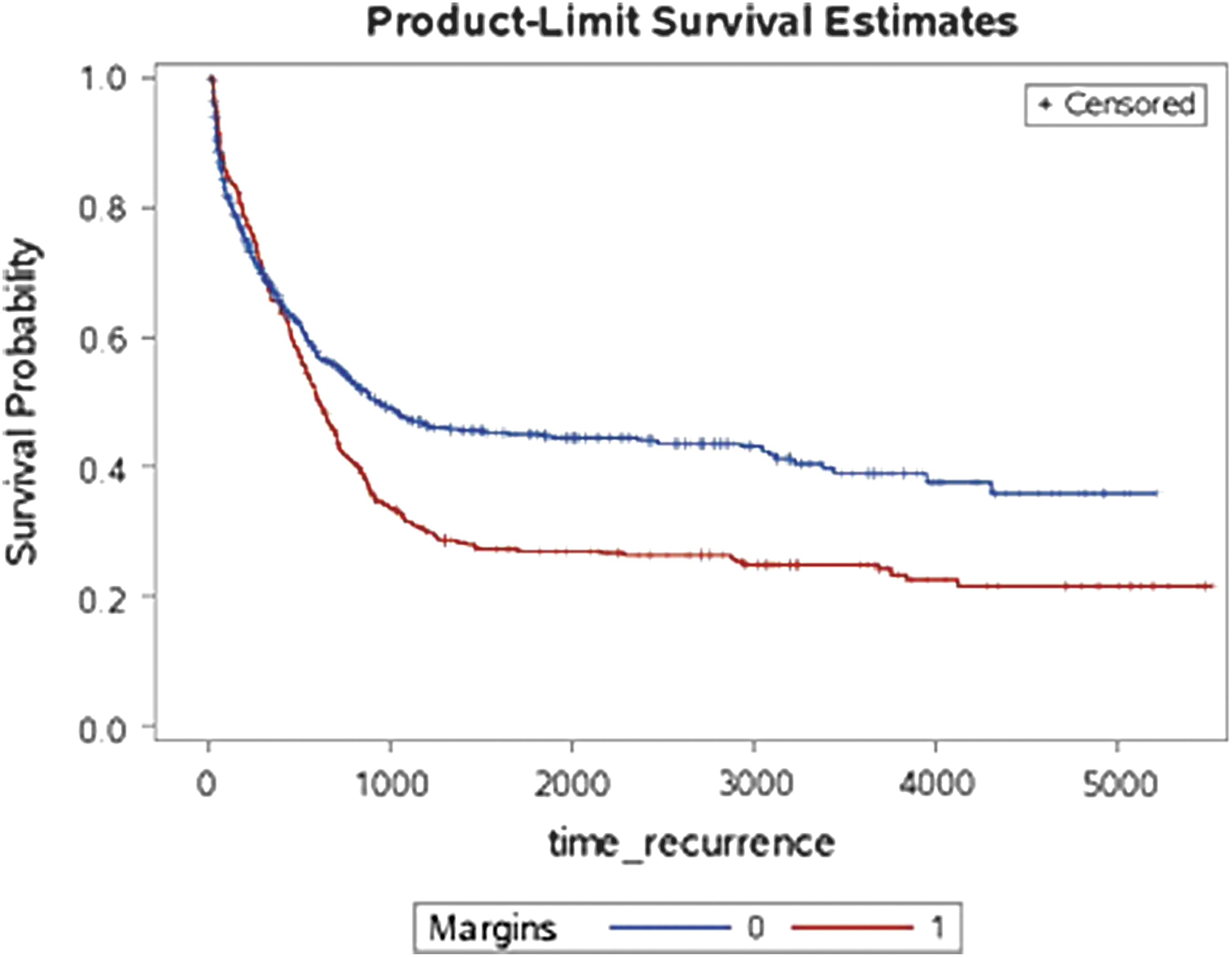
Surgical margins.

Lymphadenectomy.
Reference category.
pGs was the only variable that maintained statistical significance at multivariate analysis.
At a mean follow-up of 74 months, 911 patients (81.8%) were continent.
Pathological results
In Table 6 is reported clinical stagings and our final pathological results. About 237 patients were cT1; 64 (27%) pT2, and 173 (73%) pT3. All the cT4 tumors were confirmed by final pathological examination.
Discussion
PCa is characterized by heterogeneus presentation, extension, and progression. The D'Amico classification allows a risk stratification helping the urologist to suggest the patient the best therapeutic opportunity. However, it remains impossible to surely predict the behavior of the disease, its progression, treatment success, and the risk of biochemical recurrence. 9 If it is generally not easy to choose the best approach it is even more difficult when we have to face a high-risk tumor. 10 The surgical approach remains nowadays a matter of debate; radical prostatectomy plays an important role and it is still very controversial if a mini-invasive technique should be the standard of care. 4,5,11
The safety of the procedure and its feasibility is strongly related to the complications. Gontero and colleagues described radical prostatectomy for high-risk patients as an acceptable procedure in terms of morbidity; with increase in surgery time, transfusion rate, and lymphoceles. 12 Recently, Soares and colleagues described a large population of 1138 patients treated with LRP. 13 More than 80% were low-intermediate risk patients according to D'Amico classification. The overall complication rate was 5.2% (59 patients); which is lower than our 16.2% (180 patients); this group becomes significantly smaller if we exclude patients who needed blood transfusions, remains than just 54 patients (4.8%) which is a comparable rate. Encouraging data emerge analyzing grade III complications; the author describes complication rate of 3.3%, higher than our 1.4%. Our results seem encouraging also compared with those presented by Di Benedetto and colleagues: 446 patients with high-risk tumor undergoing LRP; the author describes an overall complication rate of 7.6% and a grade III rate of 6.5%. 14
Certainly, we report a significant transfusion rate (11%); however, this value is not so far from many results described in literature for LRP: Artibani and colleagues describe a TR of 11% in a series of 71 patients, in a series of 219 patients the TR for Rassweiler and colleagues is 9.6% and 9.8% for Rozet and colleagues after 133 LRP. 15 –17
We can assume that complications are relatively rare and most of them are not severe and also easy to treat.
The mean (SD) overall lymph node yield was 18.5 (5.7), which is comparable to data described in literature on open and robotic surgery. 18
A total of 781 patients (76.4%) underwent ePLND with a node yield of 19.1; 241 patients (23.6%) underwent stPLND with a node yield of 15.6. In Table 2 are shown pathologic data according to standard and extended procedures.
Our results are encouraging about the node yield when compared with data in literature; for an adequate detection is necessary a node yield of at least 13 nodes removed during PLND of high-risk PCa patients by robotic surgery, described by Sagalovich and colleagues, 19 and by retropubic prostatectomy, described by Briganti and colleagues. 20
We obtained an OS of 96.6% (1076) and a DFS of 66.2% (737 patients) at a mean follow-up of 74 ± 50 months, which is acceptable when compared with results by Rassweiler and colleagues that described an OS of 94.9% and a DFS of 78.2% in patients laparoscopically treated for organ-confined tumors. Our OS and DFS are also comparable with those recently described by Boorjian and colleagues 6 and Di Benedetto and colleagues 14 for patients with high-risk tumors treated with open and laparoscopic approach respectively. The last author presents a population of 446 patients and found out that the minimally invasive approach does not hide worse oncological and functional outcome when compared with an open approach. Probably, the most important comparison should be made against radiotherapy, which is described by randomized studies as the best approach for these tumors; our results are encouraging and seem comparable to the series presented by Bolla and colleagues on radiotherapy (RT) and 3 years of androgen deprivation therapy. 21 Table 3 shows how an adjuvant therapy plays a positive role in survival rate in proportion to the higher T stage. The disease persistence occurred in 75 patients after surgery; they all received an adjuvant treatment and 74 of them were alive with no BR at the follow-up. Five hundred patients did not receive any adjuvant therapy after surgery; 438 of them were alive and free of disease at the follow-up. We think our data describe an encouraging outcome for patients receiving adjuvant therapy; however, it is not easy to state the best timing like Zwergel and colleagues tried to do; they describe a 5 year PSA progression-free survival rate of 76% in patients with immediate hormonal treatment and 53% in patients with surveillance and delayed hormonal therapy. 22
Our uni- and multivariate analysis show that pT and pN are directly proportional to the probability of BR. Positive surgical margins are also a positive predictor for BR. The age at surgery is inversely proportional; younger patients are more likely to present BR after surgery. These correlations are well described in Kaplan–Mayer curves. On the contrary, in Zwergel's analysis none of the investigated parameters was demonstrated to be of independent prognostic significance for tumor-specific survival. The data regarding pN confirm the importance of lymphadenectomy in these patients as described by Briganti and colleagues who developed a nomogram and by Bader who analyzed the survival of patients with positive nodes. 23,24 Our data appear in line with the growing evidence that ePLND plays not only a prognostic role but also a therapeutic one in high-risk patients, there is now level 1 evidence as reported in literature. 25
Just pN and pGs resulted as predictors for OS and CSS; they are obviously inversely proportional.
The comparison of clinical and pathological stage brought interesting results. We reported a clinical understaging in about 30% of cT2 and in 100% of cT1. It means that patients clinically considered at low or intermediate risk could reveal a high-risk tumor, it plays a fundamental role in defining the disease and approaching it with the best treatment.
Conclusions
Our work brings encouraging data about the oncological and functional safety of LRP even in high-risk patients. We believe that radical prostatectomy represents an effective treatment for patients with high-risk PCa and that laparoscopy is a safe approach offering a mini-invasive alternative to open surgery. It also permits a better identification and characterization of the disease leading to a more accurate evaluation of the prognosis and planning of the follow-up. We therefore propose a more comprehensive use of this technology in all patients who are candidates for surgery.
Footnotes
Author Disclosure Statement
No competing financial interests exist.