
Abstract
Background:
Focal therapy for prostate cancer (PCa) remains experimental. Aim of the current study is to review available evidence and perform a pooled analysis exploring oncologic and functional results of high intensity focus ultrasound (HIFU) focal therapy for the treatment of unilateral PCa.
Methods:
The National Library of Medicine Database was searched for relevant articles. A wide search was performed, including the combination of following words: “HIFU,” “prostate,” “cancer,” and “focal.” Overall, 167 articles were reviewed. Of these, seven articles were identified and eligible for the pooled analysis. Data on HIFU hemiablation or focal prostate ablation, oncologic and functional results were pooled from these seven studies that included 366 men with unilateral PCa.
Results:
In the 366 analyzed cases, mean age was 67 years (95% confidence interval 66–69), and mean preoperative prostate-specific antigen was 6.4 ng/cc (5.5–7.4). Three studies included PCa up to Gleason 7 (3 + 4), three studies did include also Gleason 7 (4 + 3), whereas one study had no limitation in terms of Gleason score. Regarding early complications, low-grade Clavien–Dindo I–II were reported in 26% (16–37), whereas high-grade Clavien–Dindo ≥III were found in 3.8% (0–8.6). Analyzing oncologic outcomes mean follow-up was 26 months (23–31): at one year after HIFU, negative biopsy rate for clinically significant PCa was 87% (79–96), whereas salvage treatment-free survival rate was 92% (85–98). Regarding functional outcomes, reported potency rates were 74% (64–84), and continence 96% (91–100), although definitions of potency and continence were not homogenous across studies.
Conclusions:
This pooled analysis of the results of focal HIFU treatment of PCa shows promising oncologic and functional outcomes. Well-selected patients may be candidates for such a conservative partial treatment of the gland. Well-designed trials are awaited to compare HIFU focal treatment with current standard of care.
Introduction
P
The aim of the current study was to review available evidence and perform a pooled analysis exploring oncologic and functional results of HIFU hemiablation and focal therapy for the treatment of unilateral PCa.
Materials and Methods
This review was conducted in line with the recommendations from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The National Library of Medicine Database was searched for articles published between January 2007 and April 2017. A wide search was performed, including the combination of following words “HIFU” AND “prostate” AND “cancer” AND “focal.” Overall, 167 articles were reviewed. Of these, seven articles were identified and eligible for the pooled analysis.
According to the PRISMA guidelines, we used the Population, Intervention, Outcome, and Study design approach to define study eligibility. Population: Patients with localized PCa. Intervention: Focal HIFU or HIFU hemiablation of the prostate Outcomes: Rate of negative biopsies at 1 year, salvage treatment-free survival, urinary continence, and erectile function. Studies: Cohort studies. If two or more studies reported results of overlapping surgical series, we selected the one with the largest sample size.
After duplicates were removed, two authors (S.A. and F.A.) completed an independent review of 61 abstracts to ultimately select 16 studies for separate full-text evaluation. Any discrepancies in study inclusion were resolved by consulting the senior author (R.V.V.), who was in charge of supervising the systematic review process. In case of studies published by the same team from a specific center, the most recent and largest results were privileged. In accordance with all previously mentioned inclusion criteria, a final selection of seven articles published between 2007 and 2017 was made. The PRISMA flow chart depicting the process for the systematic literature search and selection of the studies is shown in Figure 1. Risk of bias was assessed following the Cochrane Handbook for Systematic Reviews of intervention. As all studies were nonrandomized, we added an extra item (“other”), which was judged by two senior authors.
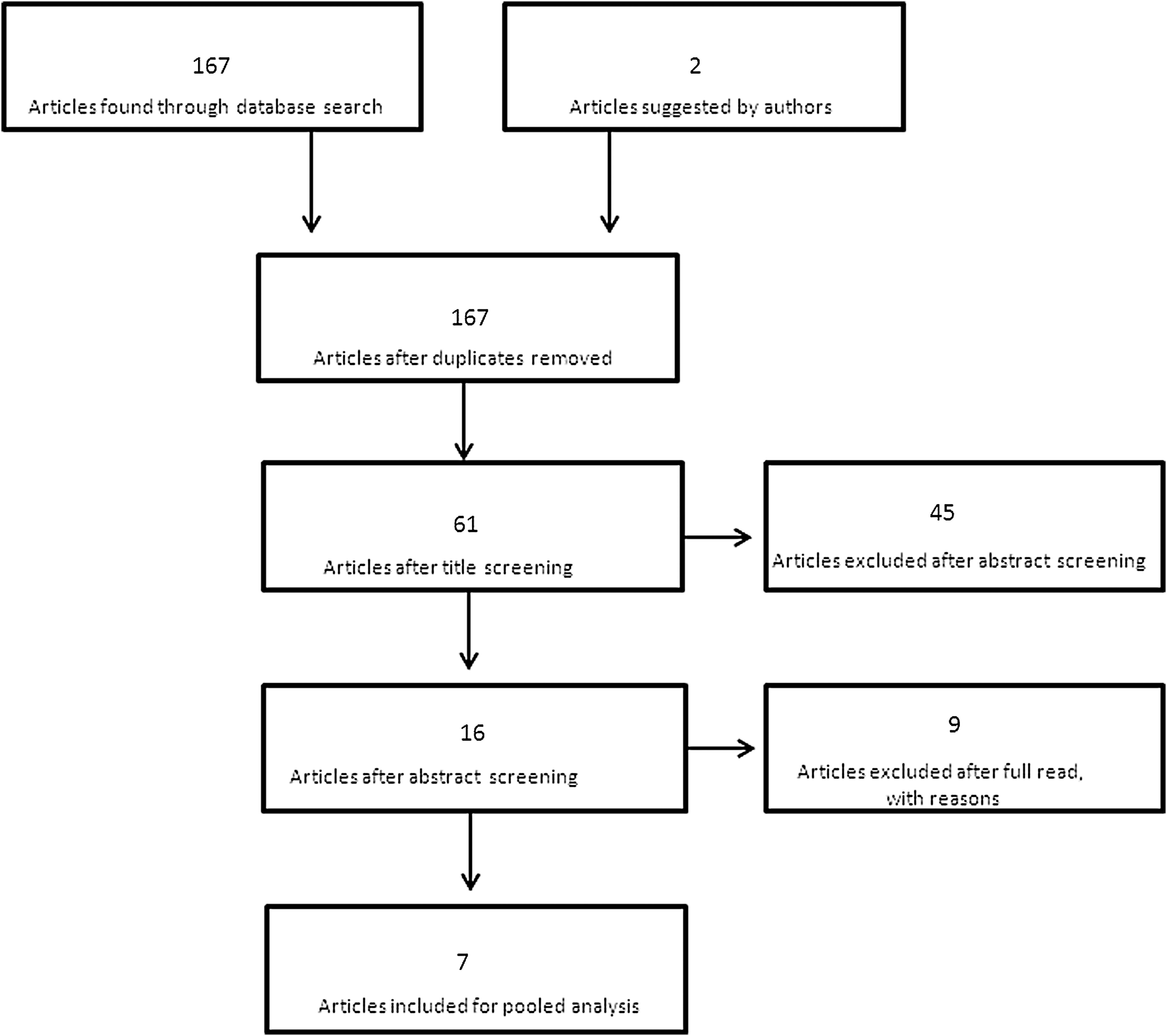
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart.
Statistical analysis
We first described each variable for individual studies by the mean or percentage with the 95% confidence interval (CI). For the percentage we used the Wilson method to avoid percentage <0% or >100%. Second, we determined the weight of each study by the inverse of the square of the standard error to take account of the number of patients in each study. The total effect is summarized by the mean or the percentage for the total effect with the 95% CI. Clinically significant PCa was defined according to Epstein criteria, 9,10 meaning Gleason score ≤6, core length ≤3 mm, and ≤2 cores involved with PCa.
Results
Three hundred sixty-six men were included in the pooled analysis of seven studies. Mean age was 67 years (66–69) and median preoperative prostate-specific antigen (PSA) level was 6.4 ng/cc (5.5–7.4). As shown in Table 1, most studies included low- and intermediate-risk PCa, 8,11 –15 with the exception of one study in which no limit was imposed. It should be underlined that such study was the oldest one, published in 2008. 16 With the exception of the team from London, 13,15 who performed focal ablation of the index lesion, all other investigators performed prostatic hemiablation on the affected lobe. Regarding follow-up, most centers perform PSA evaluation every 3 months after focal HIFU, and an MRI with associated biopsies between 6 and 12 months after the ablative procedure. Concerning risk of bias (Table 2), all studies included were observational nonrandomized trials and it was inevitably impossible to blind participants and investigators to treatment received. However, risk of detection and reporting biases were overall low.
HIFU = high intensity focused ultrasound; PCa = prostate cancer; PSA = prostate-specific antigen; TURP = transurethral resection of the prostate.
1 = low risk of bias; 2 = intermediate risk of bias; 3 = high risk of bias.
Regarding postoperative complications, Clavien–Dindo I–II were detected in 26% (16%–37%), whereas Clavien–Dindo III–IV were reported in 3.8% (0–8.6). Of note, all Clavien–Dindo III complications reported regarded endoscopic revision, mainly due to urethral stenosis or retention of necrotic tissue, and no patient died as a consequence of HIFU treatment in the analyzed studies.
Mean follow-up was 2.2 years (1.9–2.6). Concerning oncologic follow-up, it must be underlined that 3/8 studies followed patients for 12 months, whereas intermediate term follow-up details were available for the other 5/8. Control biopsy results were available in 7/8 trials: negative biopsy rate was 77% (66–87) for any cancer and 87% (79–96) for clinically significant PCa (Fig. 2). HIFU retreatment rate was 4.6%, with globally 17/366 men requiring a second HIFU session. On the other hand, salvage treatment-free survival (radiotherapy, salvage prostatectomy, or androgen deprivation therapy) rate was 92% (85–98) across the analyzed studies (Fig. 3).
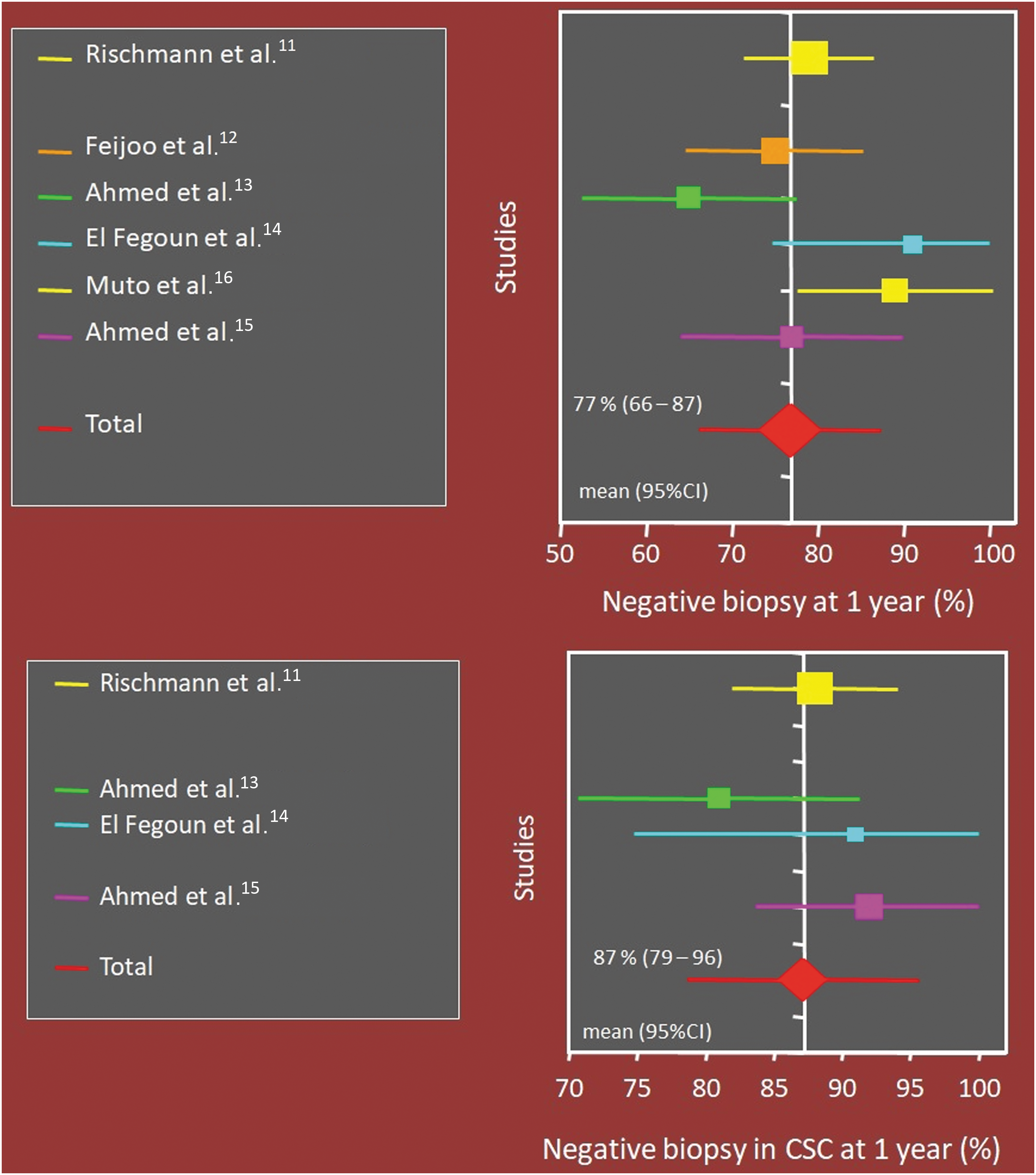
Oncologic outcomes of focal HIFU. CI = confidence interval; CSC = clinically significant cancer; HIFU = high intensity focused ultrasound.

Oncologic outcomes of focal HIFU.
When exploring functional results of focal HIFU ablation, most studies defined continence as a “pad-free” status (Table 3). Given this strict definition of continence, at 12-month follow-up, 96% (91–100) of the men included in the studies were fully continent and pad free (Fig. 4). Concerning potency evaluation, the definition in this scenario was instead more variable, ranging from “erections sufficient for penetration,” to International Index of Erectile Function 5 ≥ 16 or ≥22 (Table 3). Although such inherent limitation, we calculated potency rates at 12 months to be 74% (64–84) of the men considered potent before HIFU ablation.

Functional outcomes of HIFU focal therapy.
IIEF = International Index of Erectile Function; NA = not applicable.
Discussion
To date, focal therapy for PCa remains experimental as clearly stated by guidelines. 17 Nonetheless, great efforts are being pursued to provide strong data in support of such a conservative approach. Across energy sources for prostatic focal ablation, HIFU has been implemented for >10 years, with multiple generations of machines and growing technology enabling precise targeting and energy delivery. The current study aimed at gathering available evidence and resume current oncologic and functional data after HIFU focal ablation of PCa. The evaluation of oncologic outcomes after partial prostatic ablation can be extremely tricky and lead to misinterpretation of results. As opposed to radical therapy, especially surgery, where PSA is an excellent biomarker to detect recurrence, when healthy prostatic tissue is left behind (as in HIFU focal therapy), PSA inevitably suffers of major confounding bias limiting its accuracy. Multiple investigators have reported biochemical-free survival according to Phoenix or Stuttgart criteria, in analogy with external beam radiotherapy. 18 However, such thresholds are not validated for partial prostatic ablation to define recurrence. Therefore, comparison of focal to radical therapies in terms of oncologic outcomes may turn out to being as comparing apples and pears. To overcome such a difference, experts have proposed to use the salvage treatment-free survival rates, 4 which usually include salvage surgery or radiotherapy or androgen deprivation therapy. In the current analysis, the pooled salvage treatment-free survival rate was 92% (85–98). Villers et al. 19 recently reported short-term outcomes of partial anterior robotic prostatectomy: although excellent continence and potency rates, at 2 years follow-up recurrence-free survival was 86% and 24% of men required completion by radical prostatectomy. As said, comparison to radical prostatectomy should be cautious and to date no randomized controlled trial exists. For such reason, it is beyond our scope to compare the herein presented results to those of radical prostatectomy cohorts; as such comparison would be methodologically flawed. Our message is instead provocative, given the acceptable rate of salvage treatment-free survival, in that focal treatment should be compared with radical therapy in well-designed prospective trials. 20 Moreover, we want to stress that the present study presents a level of evidence of two (comparative studies without randomization), 21 as there were no randomized studies, and many were single-institutional, retrospective series. Furthermore, there is variability across the studies analyzed concerning inclusion and exclusion criteria (Table 1), thus imposing caution when pooling the results of such trials.
Functional outcomes are indeed a major driver of patient QoL after PCa therapy. Despite brilliant outcomes for highly experienced surgeons, 22 radical prostatectomy may lead to major deterioration of continence and potency. In the ProtecT trial, 23 the rate of patients using absorbent pads increased from 1% at baseline to 46% at 6 months in the prostatectomy arm, with great impact on QoL. High rates of urinary leakage were reported in the PIVOT (Prostate Cancer Intervention versus Observation Trial) trial, 24 with 17% of men requiring ≥1 pad at 24 months after surgery, whereas Sanda and coworkers 25 reported 76% pad-free rate 1 year after radical prostatectomy in 602 men. Moreover, when evaluating erectile function in the ProtecT trial, the percentage of patients being potent, defined as erections sufficient for penetration, decreased from 67% to 12% at 6 months after surgery. 23 Intuitively, one can expect improved functional results with focal cancer treatment: if the organ is only partially ablated, without disrupting completely the anatomy and its physiologic function, improved outcomes can be awaited. Again, comparison to radical treatment cohorts is delicate, as patient selection, age, and preoperative continence and potency status are major confounders, which must be accounted when exploring functional results of PCa therapy. Similarly to HIFU, focal cryotherapy studies report encouraging functional results. 26 Ward et al. 27 published results of the COLD registry, evaluating >1000 men who underwent focal cryotherapy, and found continence rates of 98.4%; Bahn et al., 28 in a prospective trial of focal cryotherapy in 70 patients, found potency was conserved in 86% of cases. Overall, such rates seem comparable to those reported in the herein presented results.
Finally, a potential advantage of HIFU therapy is the possibility to repeat treatment in recurring patients. Indeed, the enormous progress in preoperative imaging, MRI-fusion biopsies, and molecular imaging as positron emission tomography-prostate specific membrane antigen is ameliorating our ability to correctly select the right patient for the right treatment. 29 Nonetheless, some patients do experience recurrence with significant PCa, requiring therapy: in well-selected patients, this can safely be delivered with a second HIFU treatment to the ipsilateral or contralateral prostatic lobe. 8 In the current analysis, 5% of patients required a second HIFU treatment. Given the low morbidity and short hospital stay of the technique, 30 this is usually well accepted by the patients.
Our study is not devoid of limitations. First, the included studies are somewhat nonhomogenous, with different endpoints and study designs; pooling such different studies may therefore suffer bias. Second, it is to date not possible to identify a comparator to match HIFU focal therapy, as no focal treatment has yet been approved by international guidelines. It is our hope that prospective trials will be designed in the future to compare focal and radical therapy for PCa. The reported oncologic outcomes all suffer from bias, as even salvage treatment planning, decision and timing can be highly surgeon dependant, and thus may question the true impact of salvage treatment-free survival rates. Moreover, the follow-up of focal therapy studies is not yet as long as radical prostatectomy and radiotherapy studies and there is a lack of standardization and guidelines for the treatment of failure of focal therapy, thus introducing more bias in the interpretation of these results. Finally, overall the level of evidence of the presented studies is low, as none was randomized and most were single institution, retrospective cohorts. Nonetheless, to our knowledge, this study pools the largest data available of HIFU focal therapy, addressing a vital issue in the evaluation of management options for unilateral PCa.
Conclusions
HIFU focal therapy is today an established technique in the management of unilateral PCa. Although direct comparison of oncologic outcomes to radical therapy remains methodologically flawed, in this pooled analysis of 366 patients, we report that valid oncologic results with salvage treatment-free survival rate was 92% (85–98). Continence and potency rates after HIFU focal therapy remain extremely favorable, making this a promising technique in the years to come. Nonetheless, prospective randomized studies are highly needed to compare focal therapy to well-established radical treatment of unilateral localized PCa.
Footnotes
Authors Disclosure Statement
No competing financial interests exist.