
Abstract
Background:
Minimal literature informs the use of robotic partial nephrectomy (RPN) in patients with chronic kidney disease (CKD). Therefore, we evaluated the renal functional outcomes in CKD patients undergoing RPN.
Methods:
We reviewed a prospective database of patients undergoing RPN 2010 to 2015 and identified 182 patients who had preoperative and postoperative nuclear renal scintigraphy (at 2 and 12 months postop). Preoperative and 12-month postoperative eGFR (mL/min/1.73 m2, by MDRD) were calculated. CKD was defined as eGFR ≤60 mL/min/1.73 m2 (CKD stages III and IV). Changes in creatinine, eGFR, and split function on mercaptoacetyltriglycine (MAG)-3 scan were compared by baseline CKD status. Correlations between pre- and postoperative eGFR were calculated.
Results:
Of 182 patients, 30 (16.5%) had baseline CKD. Preoperative eGFR was 48.5 and 99.0 in CKD and non-CKD patients, respectively (p < 0.001). From preoperation to 12 months postoperation, eGFR decreased by 2.8 and 1.1 mL/min/1.73 m2, respectively (p = 0.6). On MAG-3 scan, the contribution of the surgical kidney to overall renal function decreased by 5.0% and 4.8% (p = 0.9) in the CKD and non-CKD cohorts, respectively. When comparing renal scans at 2 and 12 months postoperation, in both groups the surgical kidney significantly recovered (both p < 0.001) and the patterns of kidney function recovery was similar in both groups (CKD +2.0%, non-CKD +1.4%, p = 0.6). On long-term follow-up (>2 years), eGFR did not change significantly in either the CKD or non-CKD group (−2.8 vs −1.1 mL/min/1.73 m2, p = 0.6). On pathology, tumors were more frequently malignant in CKD vs non-CKD patients (93.3% vs 73.2%, p = 0.02) and of higher Fuhrman Grade (grade ≥3: 49.7% vs 28.1%, p < 0.001).
Conclusion:
RPN is a reasonable treatment option in patients with CKD, as it did not lead to a greater decline in renal function contributed by the surgical kidney. The patterns of kidney function recovery after surgery are similar between patients with and without CKD.
Introduction
I
As the general population ages, patients presenting for surgery have increasing comorbid conditions that can affect the overall renal function. Chronic kidney disease (CKD) is a risk factor for cardiovascular events, progression to end-stage renal disease (ESRD), and ultimately, death. Therefore, there is growing interest in NSS in patients with CKD in an effort to preserve renal function and prevent or delay progression to ESRD. Partial nephrectomy (PN) has been shown to decrease progression of CKD IV to ESRD requiring hemodialysis when compared with RN in patients with baseline CKD. 3 While several other retrospective reviews have similarly found that PN results in greater renal functional preservation than RN, the only prospective randomized study (EORTC 30904) that compared NSS with RN surprisingly demonstrated that, on average patients, in the RN cohort lived longer than their PN counterparts (10-year overall survival 81.1% vs 75.7%). 4 However, a more recent analysis of EORTC 30904 data acknowledged that NSS substantially reduced the progression to CKD III compared with RN for patients with CKD I and II.
None of the studies in the literature has used objective measurements of glomerular filtration rates as a measure of function of the partially resected kidney and followed its alterations with long-term follow-up. Serum creatinine and eGFR have been widely criticized as inadequate surrogates of individual renal function due to compensation by the contralateral nonsurgical kidney. Renal scintigraphy has emerged as a promising technology for isolating function of the surgical kidney, although literature on its use among CKD patients is limited. 5
A recent study advocated use of ipsilateral renal function (IRF), defined as the ratio of the postoperative eGFR to preoperative eGFR for the surgical kidney, to assess the function of the surgical kidney. 6 Differential functions were calculated from renal scans, confirming the authors' suspicion that overall eGFR might underestimate the impact of surgery on the functional contributions of surgical kidney; IRF preservation (72%) was significantly lower than total eGFR preservation (83%) on short-term follow-up. A separate series noted a mean decrease of 22% in the function of the operated kidney 1 month postoperatively, but there remains a need for long-term renal scintigraphy-based data in a large cohort. 7
We, therefore, sought to objectively assess short-term and long-term renal functional outcomes of the surgical kidney in patients with CKD who underwent robotic PN (RPN) for solid renal masses compared with patients with normal baseline renal function.
Methods
Study population
We retrospectively reviewed a prospectively maintained single-center database of patients who underwent RPN for unilateral solid renal masses between 2010 and 2015. All operations were performed by a single, experienced, open and robotic urologic oncologist (R.G.). Data were collected in an Institutional Review Board-approved urologic oncology database. MAG-3 renal scintigraphy was performed at patients' preoperative baseline and at 2 and 12 months postoperation. Renal function, as measured by eGFR, was calculated using the MDRD equation at baseline and 1 year postoperation. Preoperative CKD was defined as an eGFR of ≤60 mL/min/1.73 m2 (CKD stages III and IV). 8 Serum creatinine was also obtained at long-term follow-up (2–3 years postoperation) and was used to assess long-term renal function. Patients were excluded from analysis if they underwent bilateral RPN or if they had incomplete data.
Statistical analyses
Mean changes in serum creatinine, eGFR, and split function of the partially resected kidney by renal scan were analyzed using paired t-tests. Patients with and without preoperative CKD were compared using t-tests with independent samples. Correlations between preoperative and postoperative eGFR were calculated. Confidence intervals are reported as per the method of Louis and Zeger and analyses were performed using Stata 14.1/MP for Windows (College Station, TX). 9
Results
We identified 182 patients who underwent RPN during our study period for whom complete data were available. Of these, 30 (16.4%) had preoperative CKD and 152 (83.6%) did not. Sixty-one percent were male and 36.3% were African American. Patients with preoperative CKD were significantly more likely to have a history of hypertension than those without CKD (86.7% vs 61.8%, p = 0.01), but the prevalence of diabetes was similar between the two groups (43.3% vs 26.3%, p = 0.08; Table 1). Patients with CKD were more likely to have a malignant tumor on pathology (93.3% vs 73.2%, p = 0.02) and a higher Fuhrman Grade (grade ≥3, 49.7% vs 28.1%, p < 0.001). The two groups had similar rates of positive margins (CKD vs non-CKD, 0% vs 2%, p > 0.9), median tumor sizes (3.0 cm vs 2.7 cm, p = 0.3), warm ischemia time (23 minutes vs 22 minutes, p = 0.7), and surgical blood loss (75 mL vs 50 mL, p = 0.8; Table 3). Preoperative eGFR was significantly lower among CKD vs non-CKD patients (48.5 and 99 mL/min/1.73 m2, respectively).
CKD = chronic kidney disease; eGFR = estimated glomerular filtration rate; IQR = interquartile range.
In the CKD group and non-CKD groups, respectively, postoperative creatinine rise was 0.23 ng/dL vs 0.09 ng/dL (p = 0.053), which corresponded to a change in eGFR of −4.1 vs −7.3 mL/min/1.73 m2 (p = 0.3). On long-term follow-up, patients with and without CKD also had similar net changes in eGFR (−2.8 vs −1.1 mL/min/1.73 m2, p = 0.6). Ten CKD patients (33%) progressed from CKD stage II to CKD stage III. One patient progressed from CKD stage I to stage III.
Patients with and without preoperative CKD experienced a similar decline in split renal function from preoperation to 2 months postoperation on MAG-3 scan (−7.0% vs −6.2%, p = 0.6; Table 3), as well as similar recovery of surgical kidney function at 1 year postoperation (CKD vs non-CKD, 2.0% vs 1.4%, p = 0.6). The net change in function of the surgical kidney on MAG-3 scans from preoperation to 1 year postoperation was also similar between the two groups (p = 0.9).
Discussion
In this single-center study of split renal function in CKD and non-CKD patients following RPN, we found that the contribution of the partially resected kidney undergoes significant changes during the postoperative period for all patients, regardless of preoperative CKD status. For all patients, the contribution of the partially resected kidney to overall renal function was significantly lower 2 months postoperation compared with preoperation and demonstrated significant but incomplete recovery at 1 year postoperation.
When comparing the effects of RPN on short- and long-term renal functional outcomes in the surgical kidney in patients with CKD to those with normal baseline renal function, patients with CKD experienced a 7.0% decline in IRF of the operated kidney on renal scans 2 months postoperatively (Table 2). The IRF improved by 2.0% at 1 year reflecting a partial recovery in eGFR of the surgical kidney and an overall decrease in the IRF of 5.0% compared with preoperative renal scans. Although the contribution of the surgical kidney remained lower at 1 year postoperation, the surgical kidney contributed significantly more at 1 year than at 2 months postoperation (p < 0.001), indicating some recovery of kidney function over time. Similar changes were found in the non-CKD group (Fig. 1).
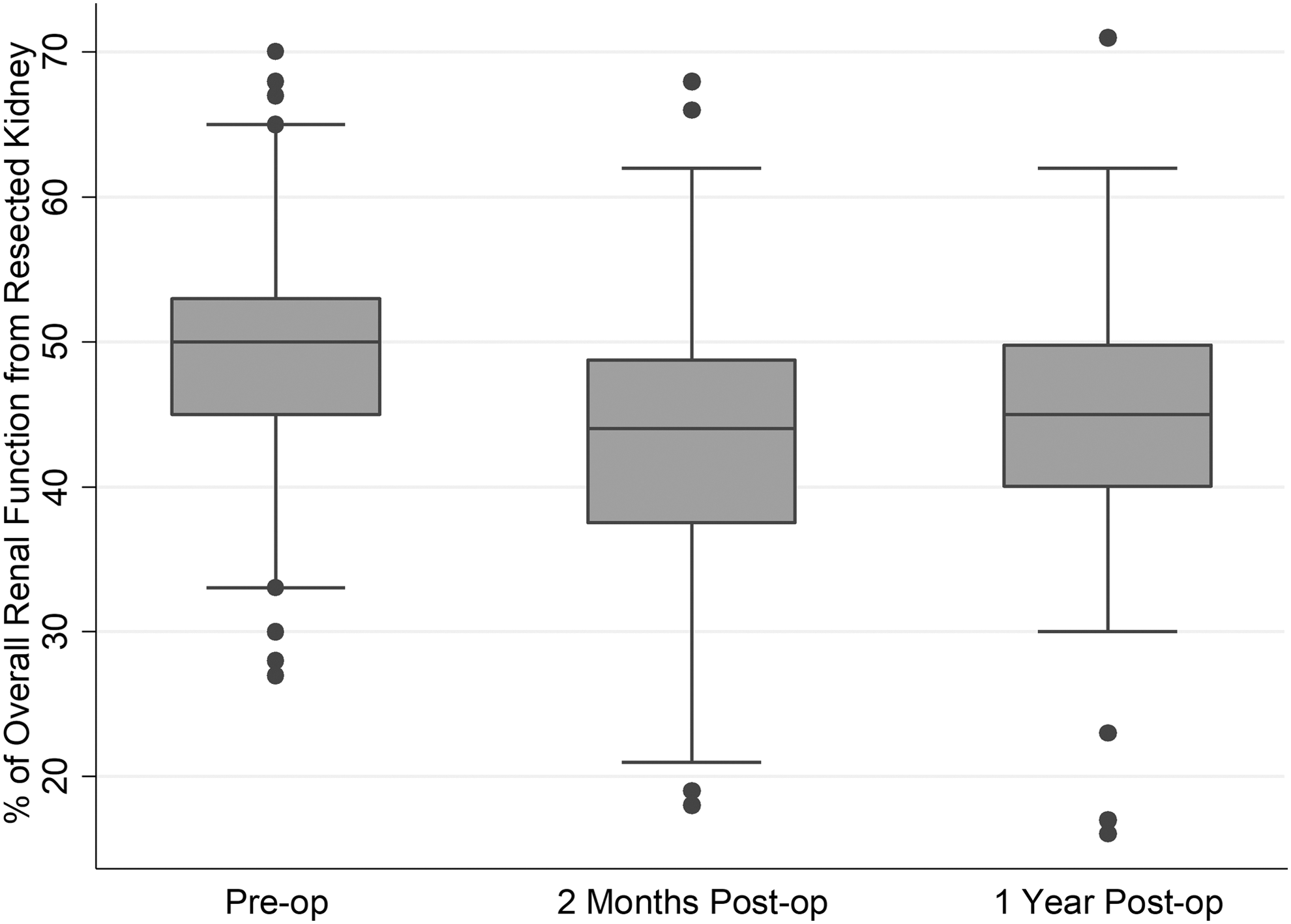
Contribution of surgical kidney to overall renal function following unilateral robotic partial nephrectomy.
CI = confidence interval.
Patterns of kidney function decline and recovery following RPN were similar among patients with and without CKD. Since our main purpose was to objectively analyze the renal functional outcomes, we elected not to perform volumetric studies in our cohorts, although the serial MAG-3 scans performed in these patients reflect some of the same changes as volumetric studies and are the most accurate tool to date that allowed us to assess split renal functions. We found no significant differences in patient or operative characteristics that might have affected surgical outcomes (e.g., warm ischemia time, tumor size, estimated blood loss) between the CKD and non-CKD groups (Table 3). In other words, a similar length of warm ischemia time and its resultant ischemic insult did not appear to affect patients with CKD more than non-CKD patients.
Postoperative renal function outcomes were also similar between patients with and without CKD; we observed similar decreases in eGFR in the first 2 months postoperatively and similar renal function recovery of the surgical kidney at 1 year among both groups. In both groups, function of the surgical kidney following RPN therefore appears to decrease, partially recover, and stabilize in a similar pattern in the first year postoperation regardless of preoperative renal function. Of note, while the changes in creatinine were statistically similar between the two groups (p = 0.053), replication of these results in larger samples is warranted to determine whether a significant difference in creatinine rise went undetected in our study due to sample size.
A recent analysis of renal function outcomes after minimally invasive NSS has suggested that although only 14% of patients will progress significantly in CKD stage at 5 years after surgery, nearly half will have progressed by the 10-year mark. 10 In a separate multi-institutional retrospective PN cohort, nearly a quarter of patients presented with CKD stage III before surgery, and 29% of patients with CKD stage I or II eventually progressed to CKD stage III at a median follow-up of 1 year. 11 The statistical analysis of our cohort (33% progressing from CKD II to III at 1 year) based on eGFR seems to correspond with numbers from other series. However, in our analysis, our CKD cohort did not include patients with CKD stage I, as we wanted to evaluate the patterns of kidney function deterioration and recovery in patients with more advanced renal impairment. At long-term follow-up (2.5 years) in our CKD group, eGFR had decreased by 2.8 mL/min. This was not statistically significant, reflecting a less substantial decrease in kidney function than anticipated. Whether this is related to improvements in understanding and treatment of renal insufficiency or to improvements in nephron-sparing surgical techniques remains unclear and requires evaluation by larger-scale studies.
Lane et al. recently suggested that the etiology of nephron loss may impact the rate of CKD development in patients undergoing nephrectomy. 12,13 They examined three groups of patients with CKD stage III; one with preexisting medical CKD undergoing surgery (CKD medical and surgical [MS]), another group that only developed CKD de novo following surgery (CKD surgical only [S]), and compared longitudinal outcomes with a registry of patients with medical CKD (CKD medical only [M]) who did not undergo surgery. The probability of progressive decline in renal function, defined as 50% reduction in eGFR or progression to dialysis at 3 years, was lower in the CKD-S cohort than those with medical renal disease. The authors proposed that patients with CKD-S may be identified as lower risk for progression to renal failure. Satasivam et al. further confirmed that patients with normal renal function but with medical risk factors for CKD, including diabetes mellitus, are at increased risk of developing progressive renal impairment despite undergoing NSS. 14 Another population-based Canadian analysis in 2011 concluded that NSS was underutilized in patients deemed highest risk for both renal and cardiovascular deterioration; those with diabetes mellitus and hypertension, were both prevalent comorbidities in our study cohorts. 15 A 2014 study by Kaag and colleagues reported up to a 30% decline in eGFR following RN. Factors independently associated with decline in eGFR included patient age, preoperative eGFR, and the presence of other comorbidities. These findings would suggest that patients with baseline CKD, as in our study population, would have a high risk of eGFR decline and poor postoperative recovery of renal function after RN. This contrasts with our findings that patients with CKD undergoing PN had comparable postoperative renal function trajectories and outcomes to patients without baseline CKD. 16
Interestingly, we found a higher incidence (93.3%) of malignant mass in patients with preexisting CKD although many confounding factors can account for this difference. This might be explained by a stricter patient selection for patients with CKD, creating a selection bias for patients with more radiographically and clinically suspicious renal masses to surgical resection. Urologists tend to be more conservative in the management of small renal masses in patients with baseline CKD out of concern for further significant decline in postoperative renal function. Therefore, patients with CKD are more likely to be followed conservatively with serial imaging to assess the growth rate of these tumors rather than early surgical resection or ablative therapy. Other strict radiologic characteristics of some renal masses are also considered, adding more selection bias in this scenario before these patients with CKD are subjected to PN. However, this selection bias would not necessarily explain the association between CKD and higher Fuhrman grade we observed among patients with malignant tumors, especially since important characteristics such as tumor size were similar between groups (CKD vs non-CKD, 3.0 cm vs 2.7 cm, p = 0.3). Again, these numbers shed light on more disparities and variables when managing renal masses in patients with CKD. Oliguria following laparoscopy is sometimes attributed to pneumoperitoneum, but there is insufficient data in the literature to show persistent detrimental effects of abdominal insufflation with carbon dioxide on kidney function in patients with normal renal function or CKD. Although our sample size is limited by the number of patients who received serial MAG-3 renal scans, we believe this objective radiologic measurement of renal function provides important data in assessing IRF following PN. However, we acknowledge that larger prospective studies with similarly objective radiologic measurements of renal function are needed to support treatment and management recommendations for these patients.
Conclusions
While patients with CKD have impaired renal function at baseline compared with those without CKD, our results suggest that the loss in IRF in the surgical kidney can partially recover by 1 year postoperation regardless of baseline renal function. While larger studies are required to confirm these results, our findings suggest that RPN largely preserves kidney function in patients with CKD and does not accelerate the progression of CKD.
Footnotes
Author Disclosure Statement
No competing financial interests exist.