
Abstract
The feasibility of laparoscopic retroperitoneal lymphadenectomy (RLA) for testicular cancer was shown >25 years ago. Initially the indication was clinical stage I (CS I) nonseminomatous germ cell tumor (NSGCT). Compared with that of open surgery, the morbidity was much decreased. However, in Europe, surgery for CS I is now replaced by chemotherapy. A relatively new indication is laparoscopic retroperitonal lymphadenectomy for small unilateral residual tumor after chemotherapy. The technique of unilateral lymphadenectomy for both indications is described in detail and with a video. The most recent development is bilateral laparoscopic RLA for residual tumors larger than 5 cm.
Preoperative Preparation
Acomplete medical history and physical examination are mandatory. A basic evaluation of blood status, including a full blood count and a biochemistry panel, is indicated. After platinum-based chemotherapy combined bleomycin, special attention should be paid to respiratory function on these patients. In such cases, a preoperative pulmonary function test might be required. Nowadays, a special bowel preparation is not required.
Patient Positioning
Similar to laparoscopic radical nephrectomy, the lateral tilted position is used in this situation; the patient is thus placed at 45° so that rotating the operating table allows frank lateral decubitus or supine positioning without having to reposition the patient. We also routinely flex the table at the level of the umbilicus (Fig. 1). Padding is used at pressure points, as with any other extended surgery. 1 An indwelling catheter is placed.
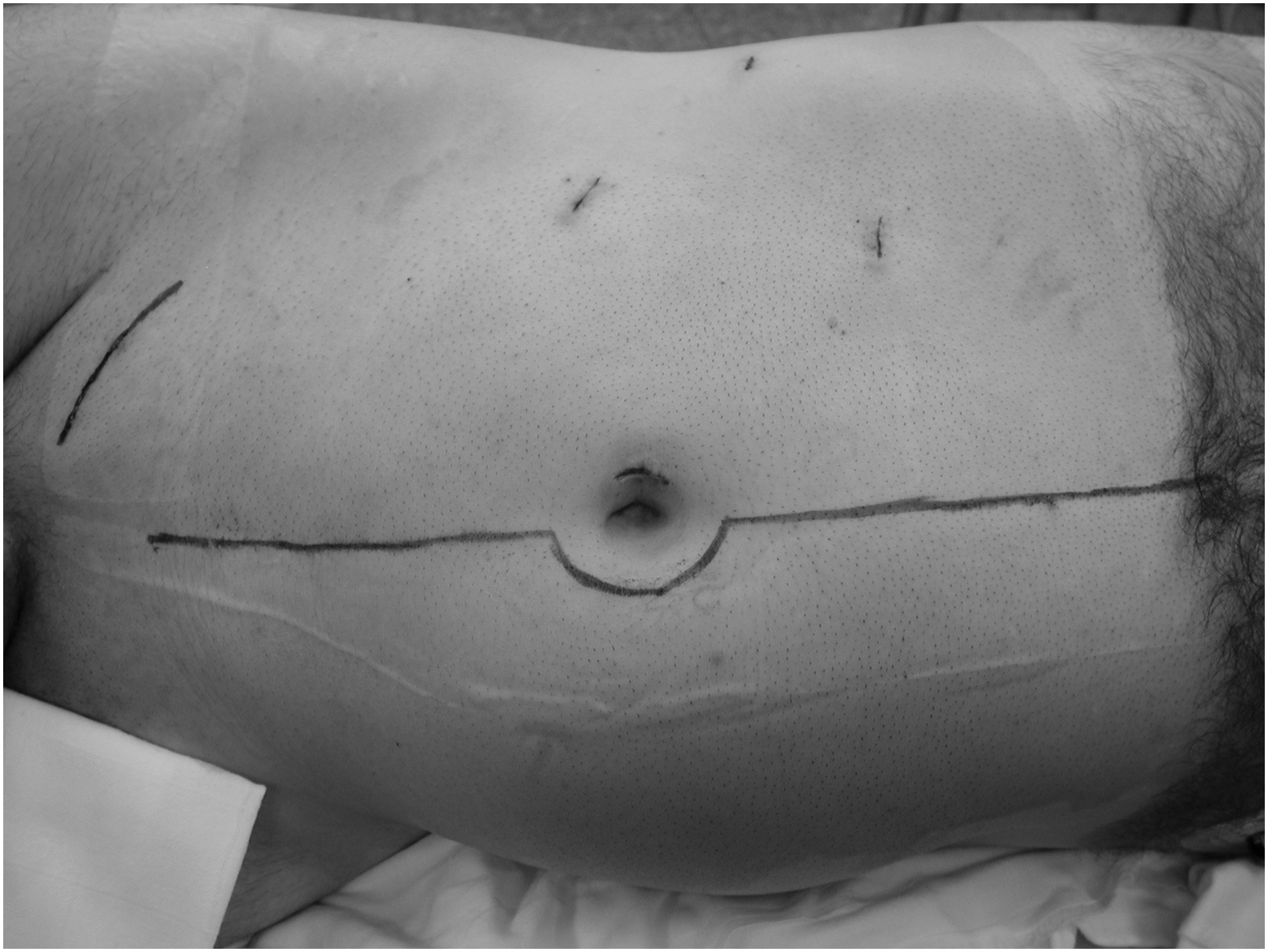
Patient positioning right side: The patient is placed in a lateral decubitus position. Camera trocar: lateral edge of umbilicus; surgical trocars: pararectal; trocar for assistant: anterior axillary line. For comparison, a line marks the incision of previous orchiectomy, and a second the typical incision for laparotomy.
Surgical Steps
Port position
The camera port is positioned at the umbilicus. Two working ports for the surgeon are placed in triangulation, lateral to the rectus muscle. A retraction port is placed in the right flank a few centimeters medial to the tip of the 12th rib (Fig. 1). For the left side, ports are placed in the same way, mirror inverted.
Technique
After a pneumoperitoneum is established through a standard approach, the surgeon starts by incising the line of Toldt for either a right or left dissection. For a right-sided dissection, the line of Toldt lateral to the ascending colon is incised in a standard manner from the hepatocolic flexure down to the cecum, to afford maximal exposure (Fig. 2). This incision is continued cranially lateral the duodenum to end in the foramen of Winslow. On the left side, the peritoneal incision is carried lateral to the descending colon, around the left flexure, and also includes the splenocolic ligament. Extra care is required to avoid pancreatic injury during this dissection.
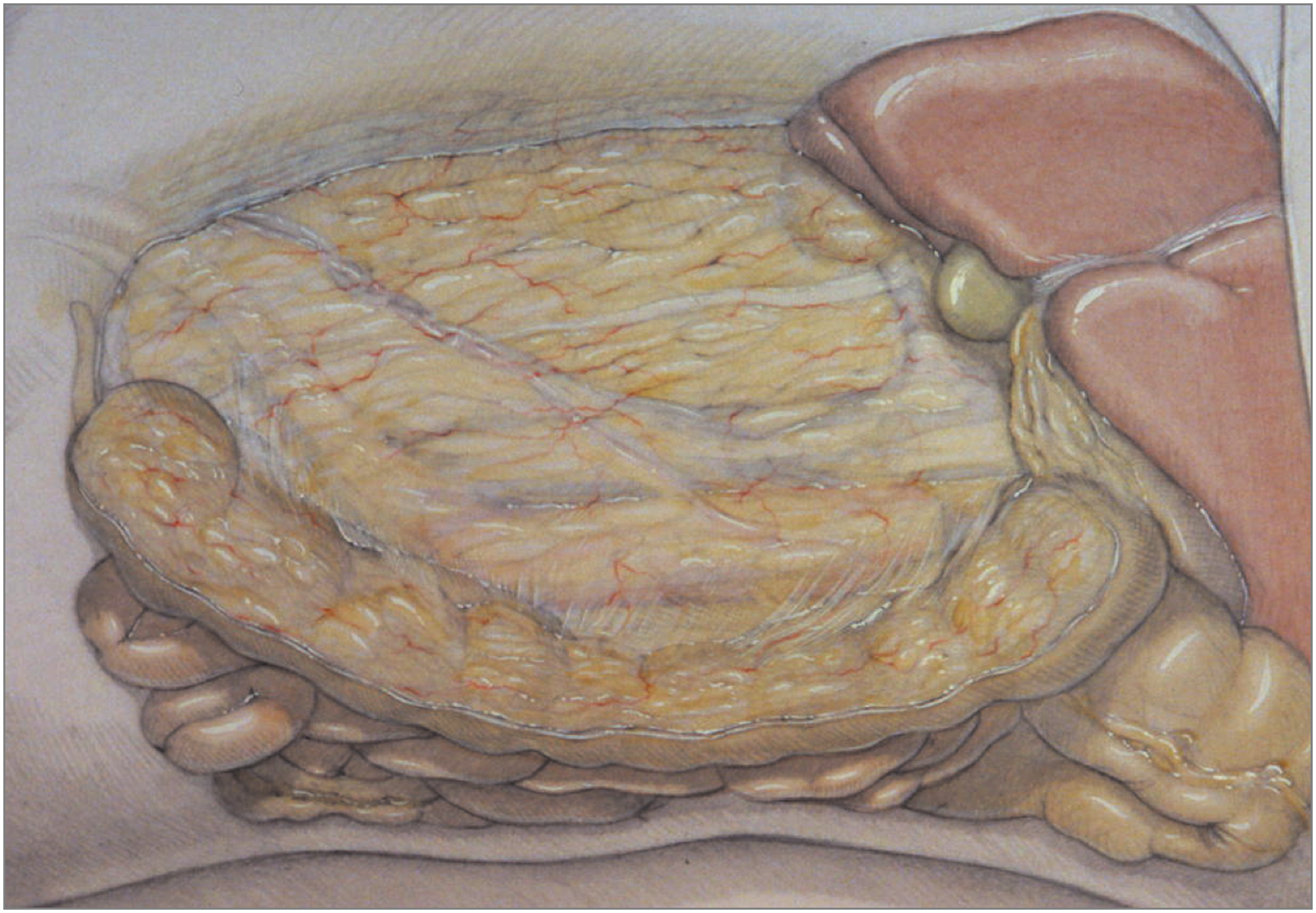
Approach right side: Wide dissection of the ascending colon, the root of the mesentery, and the duodenum together with the head of the pancreas allows for direct approach to the vena cava and aorta without further retraction of the bowel.
Then the major landmarks are identified, including the ureter laterally, the aorta or cava medially, and the renal hilar vessels cranially. As next step, the internal ring is identified. The spermatic cord remnant from the previous radical inguinal orchiectomy is dissected and completely excised.
Once the lateral border of the inferior vena cava is found, the plane leading to the psoas muscle is developed. The ureter is thus retracted laterally and all the lymphatic tissue between the ureter and the great vessels is excised, using the “split/roll” technique. Tissue within the confines of the template is resected using standard laparoscopic techniques of blunt and sharp dissection. Hemostatic clips are used liberally where lymphatic vessels are suspected.
Postoperative Care
Lymphocele formation may occur postoperatively. This is especially true after postchemotherapy retroperitoneal lymphadenectomy (PC-RLA). For this reason, placement of a drain must be avoided. Drainage leads to rapid closure of the peritoneum, possibly resulting in lymphocele formation. Without drainage, leaking lymphatic fluid will continuously drain into the peritoneal cavity keeping the peritoneal incision open. The resulting chylous ascites is much easier to handle than a lymphocele. To reduce the lymphatic flow after surgery to a minimum, all patients get special medium chain triglycerides (MCT) diet postoperatively for up to 6 weeks. The routine postoperative care includes regular blood testing, mobilization, and wound care.
Indications
Nonseminomatous germ cell tumor clinical stage I
The European Association of Urology (EAU) and the European Germ Cell Cancer Consensus Group (EGCCCG) recommend risk-adapted treatment in their guidelines for clinical stage I (CS I) nonseminomatous germ cell tumor (NSGCT), which is defined as tumor involvement that is limited to the testis, normal serum tumor markers after inguinal orchiectomy, and no retroperitoneal lymph node metastasis. 2 For patients with vascular invasion in the tumor, PEB chemotherapy is the treatment of choice, and for those without vascular invasion, surveillance should be chosen 3,4
RLA in CS I patients is preserved for patients who are not suitable for chemotherapy or surveillance in the risk-adapted treatment concerning the EAU guidelines. 3 Also, the EGCCCG suggest RLA only for patients who do not agree to or qualify for the options mentioned before. 5 These recommendations are in contrast to those in the United States. The National Cancer Institute suggests postorchiectomy surveillance to be the standard treatment option. In contrast, RLA in NSGCT CS I has proven to be the most sensitive and specific method for testicular cancer staging and, therefore, to help for choosing the best treatment option for the patient. In 30% of patients, testicular metastases are found. This leads to an upgrading in staging to stage II disease. 6
Surgical template in CS I
The template of dissection in CS I has to include all primary landing sites of the tumor and, therefore, differs according to the side of the primary. Also, the spermatic vessels are removed in their entire length. The best description of these templates has been provided by Weissbach and Boedefeld (Figs. 3 –5). 7 It has to be realized that the template for a left tumor does not include the interaortocaval space. In the United States, often the unilateral left template includes the interaortocaval space, which is in contrast to the template described by Weissbach and Boedefeld. 7 This leads to damage of both sympathetic nerves. First, nerve sparing was described by Donohue et al. 8 using such a large left template. However, they changed their template in terms of sparing the interaortocaval space in their more recent publications. Hence nerve sparing is provided by the template without compromising oncologic outcome. 9
Template right side.

Interaortocaval dissection without transection of lumbar vessels.
Template left side.
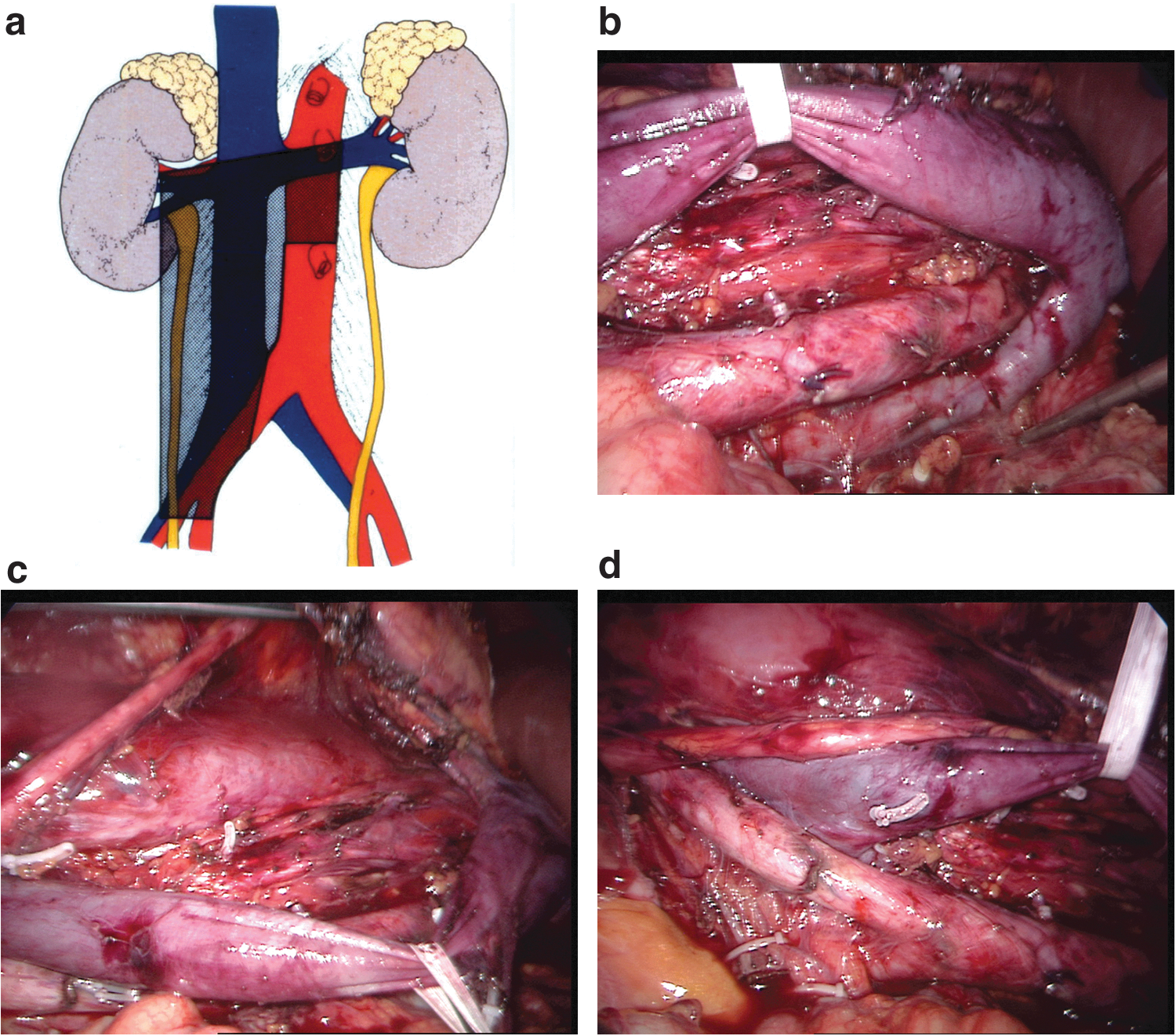
Only two publications address the question whether or not the primary landing site also includes the lymphatic tissue behind the lumbar vessels, the vena cava, and the aorta in stage I testicular carcinoma. 10,11 They both clearly show that the primary landing sites are invariably located ventrally, whereas metastases dorsal to the lumbar vessels result from further tumor spread. Therefore, removal of the tissue behind the lumbar vessels, the aorta, and the vena cava is not required in unilateral RLA for CS I (Fig. 4a, b).
Loss of antegrade ejaculation is the most common long-term complication of RLA. This problem can be overcome by performing either a unilateral template dissection or nerve-sparing RLA. When performing a right template dissection, the right postganglionic fibers, which originate from the right sympathetic chain to travel underneath the vena cava and through the interaortocaval space, are destroyed while all fibers of the left side remain intact. With a left template dissection, all left postganglionic fibers traveling along the left side of the aorta are destroyed, whereas the right fibers remain intact as long as the interaortocaval space is not approached. Complete unilateral destruction of the sympathetic nerve does not result in loss of antegrade ejaculation as long as the contralateral nerve remains intact. Therefore, when adhering to the described templates, unilateral RLA for CS I does not result in loss of antegrade ejaculation, and additional nerve sparing is not required. 12
The right-sided template
The upper limit of dissection is the renal pedicle (Fig. 3a–d). The right lateral limit is the ureter, and the left lateral limit is the ventral surface of the aorta. Note that this vessel is exclusively dissected above the inferior mesenteric artery (IMA). The lower limit of dissection is the crossing of the ureter with the iliac artery. 1 The gonadal vessels are removed in their entire length from the internal inguinal ring to their opening in the vena cava.
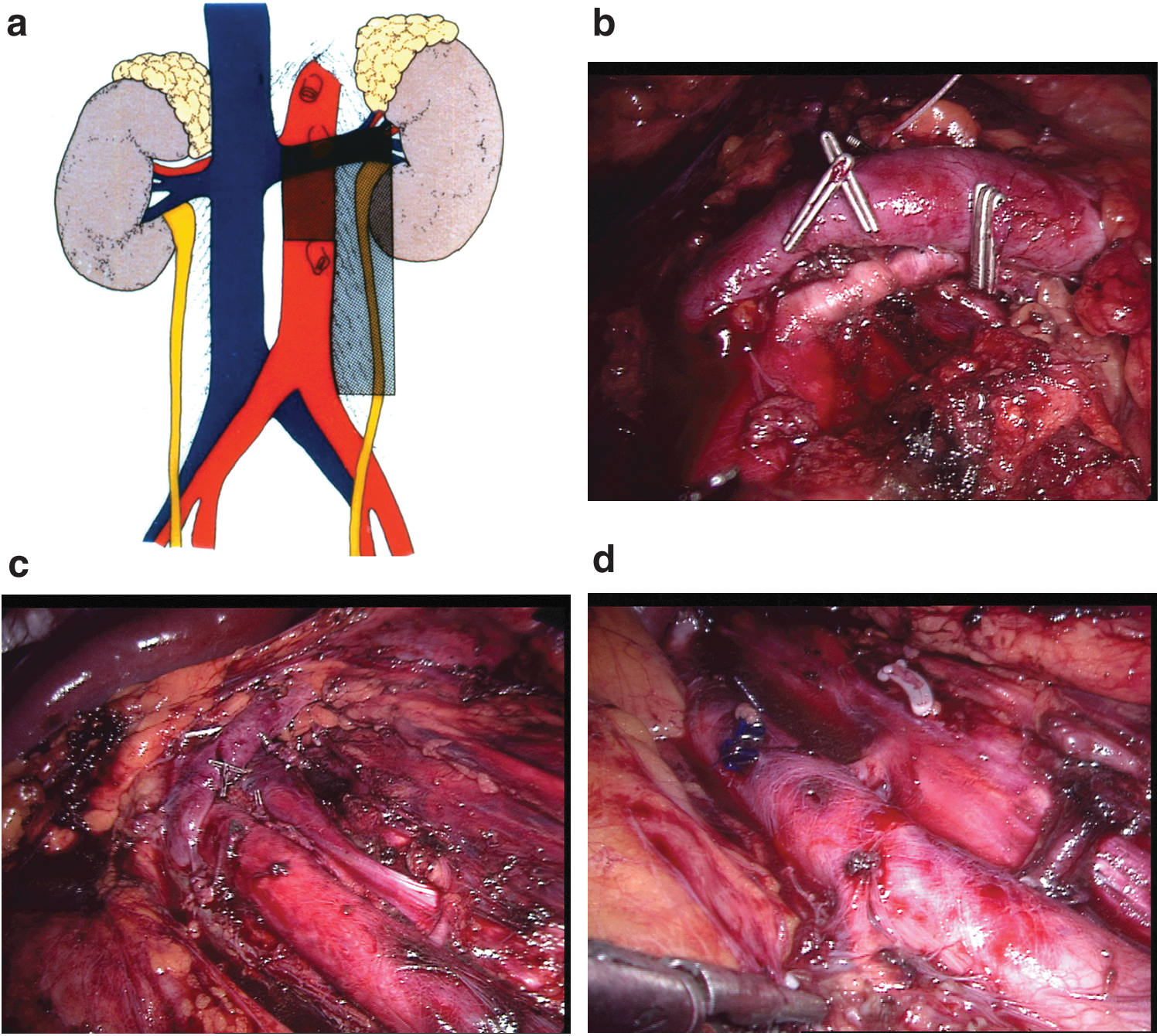
The left-sided template
The tissue ventral to the aorta is removed between renal artery and separation of the IMA (Fig. 5a–d). The IMA and all ventral tissue below are spared. All tissue left lateral to the aorta between renal artery and crossing of the ureter with the external iliac artery is dissected. Note that the interaortocaval tissue is preserved. 1 The gonadal vessels are removed.
NSGCT clinical stage IIa without elevated tumor marker (S0)
In all advanced stages of NSGCT, initial cisplatin-based chemotherapy is the standard of care. 3,13,14 Only in patients with very small lymph nodes (<2 cm) and negative tumor markers, the EAU suggests surveillance for 6 weeks. Then a CT scan should be repeated to clarify whether the lesion is stable, shrinking, or growing. 3 In case of a stable or progressive lymph node without marker evaluation, teratoma or metastasis has to be considered. In this situation, RLA should be performed with the same template as for CS I. 14
PC-RLA in advanced seminomas
A residual tumor after platin-based chemotherapy smaller than 3 cm almost never contains viable cancer and, therefore, PC-RLA is an overtreatment. 15 Even in lesions bigger than 3 cm, only in 12%–30% viable cancer was found. 16 –18 FDG-PET scan was affiliated in the EAU guideline for patients with residual tumors bigger than 3 cm to clarify viability. However, the scan must not be performed before 6 weeks after the last course of chemotherapy to reduce false positive rates. 19,20 In patients with a positive FDG-PET scan, PC-RLA is indicated. However, PC-RLA for seminoma is technically very difficult because of the severe desmoplastic reaction of the tumor on chemotherapy. Therefore, because of the rarity of the indication, only little experience exists with PC-RLA by means of laparoscopy.
PC-RLA in advanced NSGCT
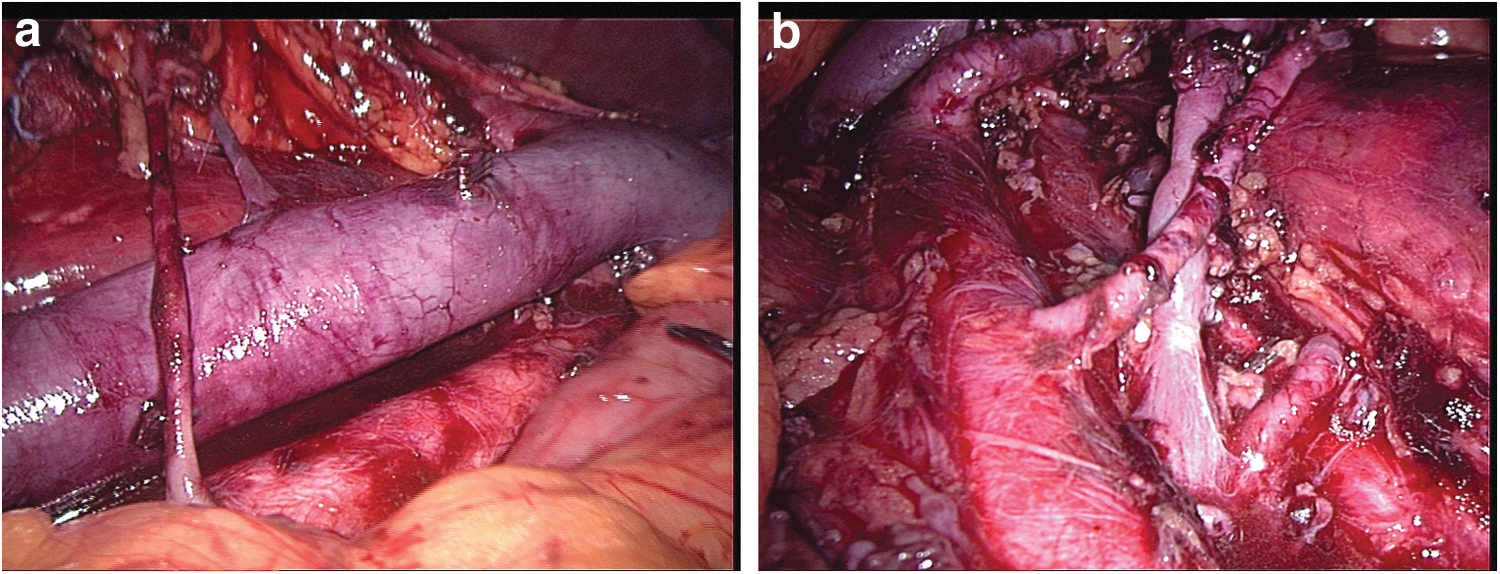
In the case of any visible residual mass and marker normalization, surgical resection is indicated 3 (Fig. 6). Even in patients with lesions <1 cm, there still is an increased risk of residual cancer or teratoma. 21 Mature teratoma was found in up to 22% and viable cancer in 9.4%. 22 In cases with teratoma in the primary orchiectomy specimen, these numbers increase to 41% and 16%. 23 Therefore, PC-RLA for residual tumors smaller than 1 cm may be considered for patients with teratoma in their primary histology analysis. 24

Right residual tumor after chemotherapy for NSGCT. The tumor closely sticks to the vena cava. Small venous branches may lead to a lesion of the vena cava during dissection.
The role of surgery in this setting is a matter of controversy. The EGCCCG and Ehrlich et al. from Indiana University suggest that patients with residual masses <1 cm can safely be observed. 5,25
Surgical template in PC-RLA
Unilateral template
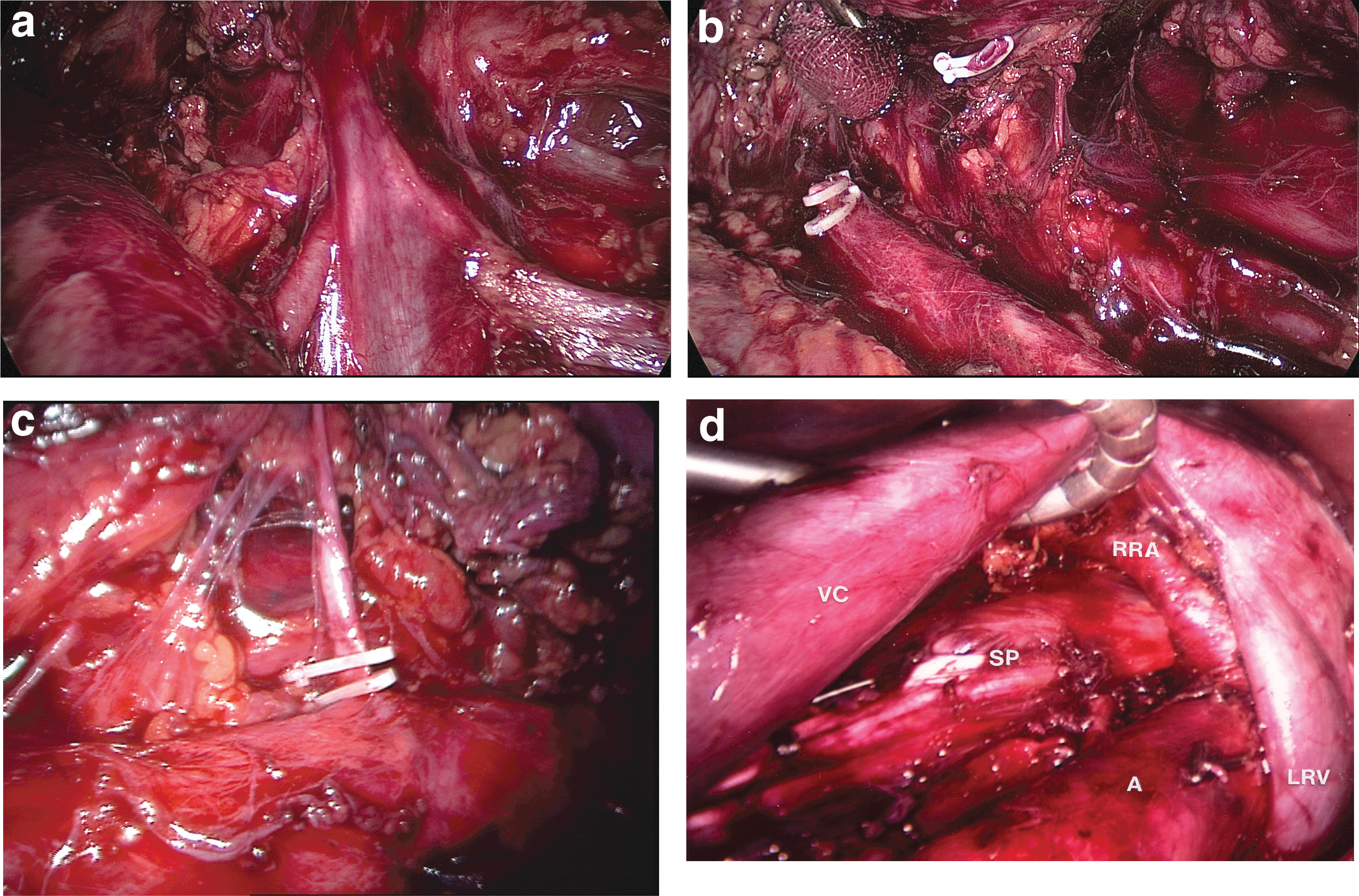
In the 1980s, when patients presented with high-volume residual disease, it was common to perform a full bilateral template dissection. In contrast, this procedure leads to damage of the sympathetic trunks, hypogastric plexus, and the postganglionic efferent nerves, and is an overtreatment for many patients. The best indication for minimal invasive PC-RLA is a small residual tumor. In this situation, PC-RLA can be restricted to a unilateral template similar to CS I. 26 The technique of PC-RLA is very similar to that of RLA for CS I. However, unilateral PC-RLA necessitates clipping and transection of the lumbar vessels within the template to remove the tissue behind which may contain small metastases not detectable with imaging techniques (Fig. 7a–d). Selection of patients suited for a unilateral template dissection is crucial. One has to make sure that the given tumor was metastasizing to a unilateral primary landing site only without further spread to the secondary or even tertiary lymph node station. Such further spread makes a full bilateral dissection mandatory. Therefore, unilateral PC-RLA should be restricted to residual tumors not larger than 5 cm. And for this assessment not only the tumor size of the residual tumor matters, but also the tumor size and unilaterality before chemotherapy has to be taken into consideration. 24,27
Bilateral template and nerve-sparing dissection
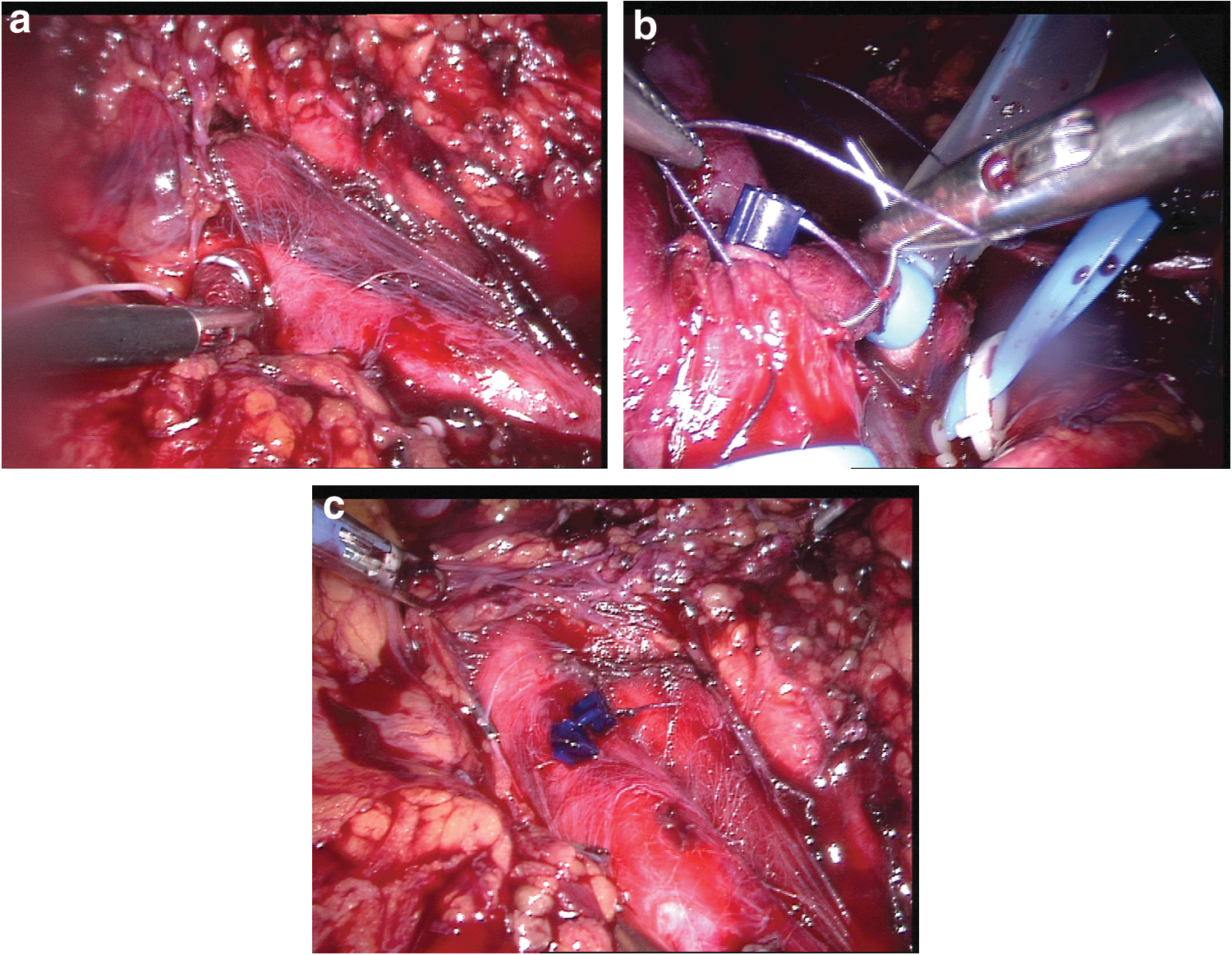
When bilateral tumor spread has to be suspected and for residual tumors larger than 5 cm, a bilateral template is obligatory. To preserve antegrade ejaculation in bilateral dissection, nerve sparing becomes essential. Steiner et al. 28 were the first to describe bilateral laparoscopic PC-RLA. The sympathetic trunk and postganglionic nerves were identified and spared. Ejaculation was preserved in 85.7% (Fig. 8a, b). Surgery was started with the patient in right lateral decubitus position. After completion of the right template, the patient was repositioned for left RLA. In a recent publication, a supine robotic approach is described, which allows for bilateral PC-RLA in one setting without repositioning. 29

Troubleshooting
Hemostasis is the problem that the surgeon faces most frequently during laparoscopic RLA. For this reason, exposure is the key to prevent complication. Special care must be taken while approaching the opening of the right gonadal vein, as this structure is very friable and can tear off easily. Furthermore, while splitting the tissue overlying the aorta in the cephalad direction, the surgeon should be aware of the crossing left renal vein, as this structure could be inadvertently injured. Similarly, accessory arteries to the kidney might be encountered during the dissection between the aorta and the kidney; their severing can result in troublesome bleeding and potential loss of renal function (Fig. 9a–d).
Lower pole artery.
The first action in case of sudden bleeding is to apply pressure using an instrument. If available, a small surgical sponge held with a traumatic grasper is best for this purpose (Fig. 10a). This will stop the bleeding similar to the finger of the surgeon in open surgery and allow the laparoscopist to gain time and thus gain better exposure, assess the situation, and adopt an optimum strategy. The surgeon should not hesitate to add an extra 5-mm trocar to manage the situation, as this might make the difference between a laparoscopic procedure and a conversion. We have always a so-called emergency suture ready on the table. This is a 4–0 polydioxanone (PDS) suture about 5 cm in length bolstered with a LapraTy clip (Ethicon Endosurgery, Cincinnati, OH) at the end. Everything is prepared to allow one quick stitch. Then the suture is held with tension that reduces or even stops the bleeding, allowing for more precise stitches (Fig. 10b, c). The use of tissue sealants such as fibrin glue might also be very helpful; however, they are inappropriate for arterial bleeding. Clips have to be handled with care because they may increase the lesion.
Management of acute bleeding:
In PC-RLA, we may be confronted with very dense tissue adherent to the vena cava and/or aorta, so that a lesion of these vessels becomes likely. Placement of a tourniquet around the vena cava or aorta below and above the tumor to be removed allows for a safe resection in this potentially dangerous situation, since in case of a sudden lesion of these vessels, the resulting bleeding can easily be stopped by cinching the tourniquets to allow for easy repair 30 (Fig. 11a, b).

Vascular tourniquet.
A delayed bleeding is a rare event, and in our experience it occurred only once after a left PC-RLA for seminoma (Fig. 12a, b). We recommend a second look laparoscopy, and in our limited experience also including second look laparoscopy for hemorrhage because of other surgeries, it was never a problem to stop the bleeding, but rather a problem to find it (Fig. 12c–d).

Delayed bleeding.
Recommended Video from Videourology
1. Videourology 2016; Vol. 30, No. 5
Robot-Assisted Retroperitoneal Lymph Node Dissection for Nonseminomatous Germ Cell Tumor in the Postchemotherapy Setting
Michael T. Marshall, Jonathan H. Berger, Haidar M. Abdul-Muhsin, Sean P. Stroup, Derweesh Ithaar H., Michael E. Woods, James Porter, Erik P. Castle, James O. L'Esperance
Footnotes
Supplementary Video
Click here for Supplementary Video: MASTER_SALK_Lymphadenectomy_H264_1080p_4Mbit_AAC_320Kbit
Author Disclosure Statement
No competing financial interests exist.