
Abstract
Purpose:
To evaluate trends in utilization of robotic assistance in partial nephrectomy (PN) and assess the association between cost and utilization.
Patients and Methods:
Using the 2009–2012 Nationwide Inpatient Sample database, we identified all adult (>17 years) patients undergoing PN for localized primary renal malignancy. Coding for robotic assistance (17.4 × ) began in the final quarter of 2008. The primary outcome was total hospital cost exclusive of physician fees. A multiple linear regression model was used to adjust for patient and hospital characteristics.
Results:
Between 2009 and 2012, there were 32,664 (58%) open, 3498 (6%) laparoscopic, and 20,350 (36%) robot-assisted partial nephrectomies performed in the United States. Between 2009 and 2012, the total number of partial nephrectomies semiannually increased by 93% (5114–9845) with robotic partial nephrectomies (RPNs) representing >80% of the increase. RPN increased from 1029 cases in the first half of 2009 to 4840 in the last half of 2012 and surpassed utilization of open nephrectomy. The proportion of all partial nephrectomies performed with robotic assistance increased from 20% to 49% during the same period. After adjusting for demographics, Charlson comorbidity index, and hospital region, RPN went from $1,464 (p = 0.009) more than open in 2009 to $456 (p = 0.28) less than open in 2012.
Conclusions:
Utilization of RPN surpassed open in 2012 in the United States. The difference in cost between the robotic and open approaches decreased during the study period and by 2011 was not statistically different.
Introduction
P
Risk factors for chronic kidney disease (CKD) are seen in up to 66% of patients treated for kidney cancer, and CKD is an independent risk factor for cardiovascular events and overall survival. 3,4 More people die from end-stage renal disease than any single urologic malignancy, making nephron-sparing techniques such as PN of increasing importance. 5 Recent reports show that the majority of small renal masses are treated with radical nephrectomy despite clinical practice guidelines advising PN. 6,7
Robotic assistance is associated with increased utilization of PN vs radical nephrectomy, and recent reports show cost neutrality when robotic assistance is used in surgeries requiring reconstruction such as pyeloplasty nephrectomy and PN. 8 –11 Robotic assistance provides increased dexterity, advanced imaging, and a shorter learning curve than the pure laparoscopic approach, making it appealing for PN where time-sensitive intracorporeal suturing of a highly vascular organ is required. 12,13 Our objective was to analyze the trends in cost and utilization of robotic partial nephrectomy (RPN) in a nationwide population-based dataset.
Patients and Methods
Database
The Nationwide Inpatient Sample (NIS) database, which is made available by the Healthcare Cost and Utilization Project (HCUP) of the Agency for Healthcare Research and Quality, 14 provides an annual 20% capture of all inpatient hospitalizations at community and academic hospitals in the United States. NIS is an administrative database, relying on International Classification of Disease version 9 (ICD-9) coding, that enables the study of trends in hospitalizations and associated costs over time and between regions. HCUP provides weights that are used to generate national-level estimates of hospitalization procedures and diagnoses. In addition, a cost to charge ratio is provided to calculate total hospital costs associated with the hospitalization, exclusive of physician fees. 15
Patients
Using the 2009 to 2012 NIS database, we identified all adult (>17 years) patients undergoing PN for primary renal malignancy using ICD-9 procedural code 55.4 and ICD-9 diagnosis code 189.0. Patients with known metastases to solid organs were excluded (197.0, 197.7, and 198.x). Robot-assisted cases were identified by ICD-9 modifier 17.4 × and laparoscopic cases were identified by 54.21 and 54.51. Cases not identified as robotic assisted or laparoscopic were considered open cases. As there was no option for identifying cases that convert between techniques, it was assumed that any case that converted to open was coded as an open case. Coding for robotic assistance (17.4 × ) began in the final quarter of 2008.
Outcomes and variables
The primary outcome of interest was total hospital costs associated with hospitalization for a procedure. Variables included in the analysis included patient-based, hospital-based, and hospitalization-associated characteristics. The Charlson comorbidity index (CCI) was calculated using the methods of Deyo et al. 16 Inpatient complications were evaluated by organ system using previously established methods. 17,18 NIS requires that any presented data be based on at least 11 patients, and thus, some complications did not meet this requirement and were included only in the binary “postoperative complication” variable. These complications included vascular, neurologic, and wound infection complications.
Total charge is the amount the hospital billed for the case, and total cost reflects estimated costs to the hospital for hospitalization. Fixed costs associated with robot acquisition and maintenance are not applied to patients in a uniform manner throughout the country, and thus, we are unable to assess the impact that robot-specific costs have on our analysis. All variables were evaluated for completeness and only race and cost were missing >10% of data. Both are known to be missing with high frequency in the NIS database because of certain states not reporting these variables. In our study, race was missing for 18% and cost was missing for 11% of patients. As cost was missing nondifferentially, specific to institutions and states, we included cost as the primary outcome of the linear regression model.
Statistical analyses
Using HCUP methodology, patient discharge weights were applied to data to estimate national incidence of partial nephrectomies. 14 Descriptive analyses were performed using Pearson's chi-squared test and analysis of variance. Multiple linear regression was used to evaluate hospital costs associated with hospitalization for PN for 2009–2012 and then individually for each year to examine whether costs attributed specifically to the robotic approach changed over the study period. Variables included in the model were surgical approach (open, laparoscopic, and robotic assisted), demographic characteristics, CCI, hospital region, and discharge quarter. The multiple linear regression model only used cases performed between the final quarter of 2008 and 2012 to account for the lack of robotic coding before this time. General estimating equations were used to adjust for confounding from year of surgery and the hospital in which the surgery was performed. A priori significance was set at p < 0.05 and all statistical tests were two sided. All statistical analyses were performed using Stata 12.1 (Stata Corp. LP, College Station, TX). Institutional review board exempt status was granted for the conduct of this study.
Results
Between 2009 and 2012, 56,512 patients underwent PN for primary renal malignancy. A total of 32,664 (58%) of these were open cases, 3498 (6%) were laparoscopic cases, and 20,350 (36%) were robot-assisted PN. Between 2009 and 2012, the total number of partial nephrectomies performed in the United States semiannually increased by 93% (5114–9845) with RPNs representing >80% (3811/4731) of the increase. RPNs increased by 370% (1029–4840) semiannually, and the proportion of all partials performed with robotic assistance increased from 20% to 49% (Fig. 1). Table 1 shows demographic information. Open partial nephrectomies (OPNs) tended to have more minorities (p = 0.01), a higher Charlson score (p < 0.001), more northeast patients (p < 0.001), more rural patients (p < 0.001), and less private insurance (p < 0.001). The majority of PNs were performed in urban teaching centers, and the majority of cases had private insurance listed as the primary payer. As shown in Table 2, median length of stay was 1 day longer for the open compared with laparoscopic and robot-assisted PN cohorts (p < 0.001).

Changes in utilization of open, robotic, and laparoscopic partial nephrectomy from 2009 to 2012.
Percentages are rounded so will not add to exactly 100 in each instance.
As all patients had known malignancy, the lowest possible CCI score was 2.
CCI = Charlson comorbidity index; SD = standard deviation.
Accidental intraoperative puncture of an organ or blood vessel.
IQR = interquartile range; NR = not reportable because of too few cases.
Seventeen percent of OPN cases developed an in-hospital postoperative complication compared with 14% of laparoscopic and 10% of robot-assisted PN (p < 0.001). The most common complications among open and laparoscopic patients were digestive complications at 3% to 4% compared with 1% for robot-assisted PN (p < 0.001). Cardiac complications occurred in ∼1% of all patients, regardless of surgical approach (p = 0.051). Accidental intraoperative puncture of an organ or blood vessel occurred in 2% of OPN, 2% of laparoscopic partial nephrectomy (LPN), and 1% of robot-assisted PN (p < 0.001). One hundred twenty-seven OPN patients died.
Median unadjusted total costs were $12,497 for open, $12,457 for laparoscopic, and $13,878 for robot-assisted PN (p < 0.004) (Table 2). As shown in Figure 2, costs associated with the open and robot-assisted approach have become more comparable with time and the proportion of cases being performed with robotic assistance is increasing, while the proportion of laparoscopic cases remains relatively constant in the study period. After adjusting for costs associated with preoperative factors and discharge quarter, the robotic approach during the 2009–2012 time period was independently associated with a $848 increased cost to the hospital (p = 0.004) compared with open, while the laparoscopic approach was associated with a nonsignificant $172 decreased cost (p = 0.736) (Table 3). In 2009, the adjusted hospital costs associated with RPN compared with OPN were $1464 (p = 0.009). However, in 2012, the RPN technique was associated with a nonsignificant decrease of $456 (p = 0.28) when compared with the open technique.
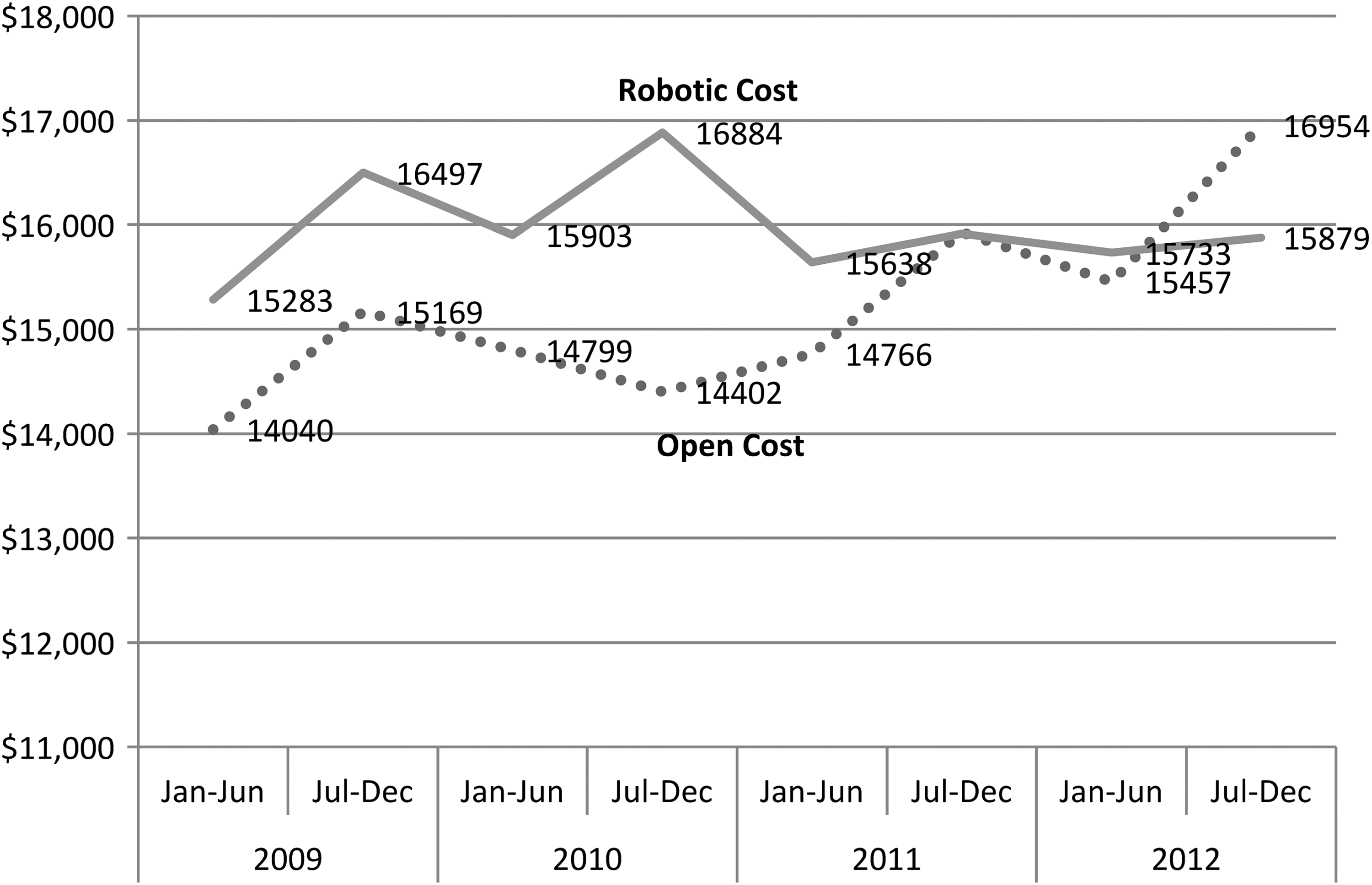
Changes in hospital cost for open and robotic partial nephrectomy from 2009 to 2012.
CI = confidence interval.
Discussion
In 2009, the Institutes of Medicine listed comparative effectiveness studies of robot vs traditional surgical approaches as a priority, and numerous studies have since evaluated cost and clinical outcomes of robot assistance. 19 However, looking at the cost of RPN as a function of increasing utilization or time has rarely been done. Temporal effects of robotic assistance on cost in a population-based sample have been difficult to study as ICD-9 codes have only recently added a robotic designation. Our results demonstrate that cost neutrality was achieved for RPN during the first full 3 years of robot-assistance designation in ICD-9 codes.
Between 2009 and 2012, the total number of partial nephrectomies performed in the United States increased by 93%, with RPNs representing >80% of the increase according to the NIS dataset. During that time the number of RPNs increased by 370%, and the proportion of all partials performed by robotic assistance more than doubled from 20% to nearly 50% (Fig. 1). LPNs decreased from 10% to 6% of all partials during the same time. The rapid adoption of RPN is remarkable when compared with the slow adoption of LPN. After the introduction of LPN in 1993, the utilization of LPN increased to only 9.7% over the next 15 years. 20,21 The rapid adoption of RPN that we report in this study is likely explained by improved dexterity, advanced imaging, and a shorter learning curve than LPN. 12 Interestingly, studies show that access to robotic technology is associated with the selection of partial over radical nephrectomy on adjusted analysis. 8,10 These findings might represent situations where, without access to RPN, surgeons and patients favor a minimally invasive technique (laparoscopic nephrectomy) over a more invasive but nephron-sparing procedure (OPN) to remove small renal masses. We feel the procedural selection (PN vs radical nephrectomy) should depend on patient and tumor factors rather than surgical technique.
During the 3-year span, the unadjusted cost difference between RPN and OPN decreased to essentially 0 (Fig. 2). On adjusted analysis, the difference in cost between RPN and OPN went from plus $1,464 (p = 0.09) in 2009 to minus $456 (p = 0.28) in 2012 (Table 3). The decreasing cost difference between RPN and OPN could be because of increasing utilization and increasing number of surgeons who have overcome the initial learning curve. Factors affecting cost such as operating room time, complications, and blood loss improve during the initial learning curve. 22 In our study, both complication rate and length of stay were lower for RPN vs OPN. While the actual cost of RPN did not decrease during the study period (Fig. 2), it did hold steady during a period of rising healthcare costs in both this study and in general. On adjusted analysis, each 6-month period was associated with an increase of $142 (p < 0.001). Also, since the start of the recession in 2007, the adjusted health spending in the United States rose by 17.2%. 23
Numerous studies have evaluated cost in PN with differing results. Mir and colleagues built a cost model based on data published before 2011 and found LPN to have the lowest cost at $10,311, while OPN ($11,427) and RPN ($11,962) cost more. 24 The capital cost (purchase and maintenance) of the robot was included and calculated at $1,214 per case by amortizing the robot over 7 years (300 cases per year). At our institution, a $1,500 capital-cost fee is added to all surgeries with robotic assistance for accounting purposes. Additional costs for robotic instruments were included at >$1,000 per case. In a single-institution analysis of 325 RPNs, LPNs, and OPNs performed in 2009 and 2010, Laydner and colleagues found RPN to be $632 more than LPN, but not statistically more expensive than OPN. 11 However, this was not matched on tumor size and capital costs were not included. More recently, Hughes and colleagues 25 found similar costs for RPN and OPN at both 1 and 3 years after surgery. They evaluated 2173 patients who underwent OPN, LPN, or RPN and included downstream recovery costs. There were fewer inpatient admissions and hospital bed-days at the 360-day mark for RPN than OPN. The robotic approach was associated with a nonsignificant reduction in cost at 3 years (£2,122 vs £2,889, p = 0.57). Unfortunately, patient factors were not adjusted for.
While robotic assistance has failed to demonstrate consistent improvements in clinical outcomes for radical prostatectomy, recent studies show improved clinical outcomes for RPN over LPN and OPN. 26 Wu and colleagues in a recent meta-analysis reported RPN was associated with fewer Clavien 1–4 complications when compared with OPN. 27 When comparing LPN to OPN in an unmatched sample of 1800 partial nephrectomies, Gill et al. noted increased complications for LPN. 28 In another meta-analysis, Mir and colleagues also reported that RPN had fewer complications compared with both LPN and OPN. 24 However, the studies included in the meta-analysis were not matched as evidenced by differing tumor sizes in the RPN, LPN, and OPN groups (2.9, 2.7, and 4.0 cm, respectively). Long and colleagues compared RPN with LPN in a dataset of intermediate to complex tumors that were matched. They found LPN was associated with an increased rate of conversion to radical nephrectomy (11.5% vs 1%) and a higher decrease in percentage estimated glomerular filtration rate in experienced hands. 29 In the present study, overall complications were lower for RPN (10%) compared with LPN (14%) and OPN (17%), although we were unable to control for tumor size (Table 2).
The findings in the present study support the hypothesis that robotic assistance is of increased benefit in surgeries requiring reconstruction. For example, Yang and colleagues recently reported that robotic assistance in radical nephrectomy is associated with an increased cost of around $3,500 or 30% when compared with the pure laparoscopic approach. 30 They speculate that robotic assistance for an extirpative procedure without complex resection or intracorporeal suturing does not provide a surgical advantage. However, in cases such as PN where resection and reconstruction occur while trying to limit ischemia times, benefits are seen.
Limitations of population-based studies include dependence on individual hospitals for coding accuracy. This could result in undercoding of minimally invasive procedures for which modification codes are required. It is also outside of the scope of the database to explain why the costs of OPN increased in the final period of this study to approach that of RPN. While it may partly be due to nationwide increases in the cost of delivering surgical care, it could also be due to surgeon selection leading to more complex cases being performed open. NIS does not contain pathologic data causing tumor-specific matching or adjusting to be impossible. It is also important to note that conclusions in this article are based on costs reported by each hospital as reimbursement amounts are not available. However, this is one of the first nationally representative studies to explore utilization of and costs associated with RPN, particularly with regard to how they have changed over recent years.
Conclusions
The utilization of robot-assisted PN more than doubled during the 4-year study period and was responsible for >80% of the increased number of partial nephrectomies performed in the United States. On adjusted analysis, RPN became cost neutral when compared with OPN during a period of increasing utilization.
Footnotes
Author Disclosure Statement
No competing financial interests exist.