
Abstract
We herein propose a nomenclature for renal calices and anatomical classification of the renal pelvis for endoscopic surgery. We prospectively collected data on a total of 270 patients (540 kidneys) who underwent CT-urography. We then constructed three-dimensional images of the renal pelvis and examined their morphologic classification. Forty-eight kidneys were excluded from this study because of severe hydronephrosis or large renal cysts. The remaining 492 kidneys were included. We systematically categorized each minor calix into five levels: top, upper, middle, lower, and bottom. The upper, middle, and lower calices were typically found in pairs: anterior and posterior. The most common total number of minor calices was eight (51%), followed by seven (30%). We also classified the form of the pelvis into type I: single pelvis (58%) and type II: divided pelvis (42%), according to the branch patterns of the renal pelvis. In type II, the renal pelvis is always bifurcated into the upper branch (top and upper) and lower branch (middle, lower, and bottom). Type I was subclassified into three types: type Ia (43%), the standard type; type Ib (4%), with a wide pelvis; and type Ic (11%), with a narrow pelvis. This anatomical classification can divide the renal pelvis into two major types (subdivided into four types) and name each minor calix. This simple classification enables to share common intrarenal information, thus leading to the development of concrete treatment strategies.
Introduction
O
At the same time, we are facing a dilemma in terms of the difficulty of applying conventional terminology to the description of the actual surgical findings in medical charts. It is no longer sufficient to simply write major calix; rather, each minor calix should be described. However, anatomical differences in the renal pelvicaliceal system make it difficult to describe the detailed ureteroscopic findings and share common information about the position of a stone or tumor, or the appropriate puncture site for a percutaneous approach. Currently, the nomenclature to describe the minor calix is not unified.
Thus, we analyzed a number of CT-urography images and proposed the nomenclature for each minor calix and simple morphologic classifications of the renal pelvis that are appropriate for actual endoscopic surgery.
Materials and Methods
The study subjects included 270 patients undergoing CT-urography as a detailed examination to determine the cause of hematuria or follow-up for patients with malignant tumors at our hospital during the period from January 2013 to September 2016. Patients with urolithiasis were excluded. Scans were taken at 7 minutes after the injection of a contrast medium for the urinary phase, and three-dimensional (3D) CT-urography images were reconstructed using the Synapse Vincent Version 3® 3D image analysis software program (Fuji Medical Systems, Inc., Tokyo, Japan). We examined the position of each minor calix and the branch patterns of the renal pelvis, and considered the morphologic classifications for the pelvicaliceal system.
To assess reproducibility of the developed classification system, three urologists (R.T., Y.K., and S.Y.) classified an additional 50 kidneys. The reproducibility was assessed using the free marginal kappa coefficient: a chance-adjusted measure of agreement using the online kappa calculator (available from
This study was performed in accordance with the ethical standards of the Declaration of Helsinki and was approved by the ethical committee of Tokyo Metropolitan Ohtsuka Hospital.
Results
Of the 270 cases with 540 kidneys that were included as study subjects, a total of 492 kidneys were analyzed. Forty-eight kidneys that were difficult to evaluate because of severe hydronephrosis or large renal cysts were excluded.
First, regarding the position of each calix, the standard most frequently observed positions were those classified into five levels beginning from the upper pole. These included the top (T), upper (U), middle (M), lower (L), and bottom (B), with the three mid parts, upper, middle, and lower, each arranged in anterior (A) and posterior (P) pairs (Fig. 1). The top and bottom levels constituted the compound calices, with the convergence of two to four small calices to form a single calix. When these compound calices were counted as one calix, the most common total number of calices was eight (51%, 252/492), followed by seven (30%, 150/492) (Fig. 2). In some cases, the upper, middle, or lower levels had only one calix; in others, they had three to four calices.
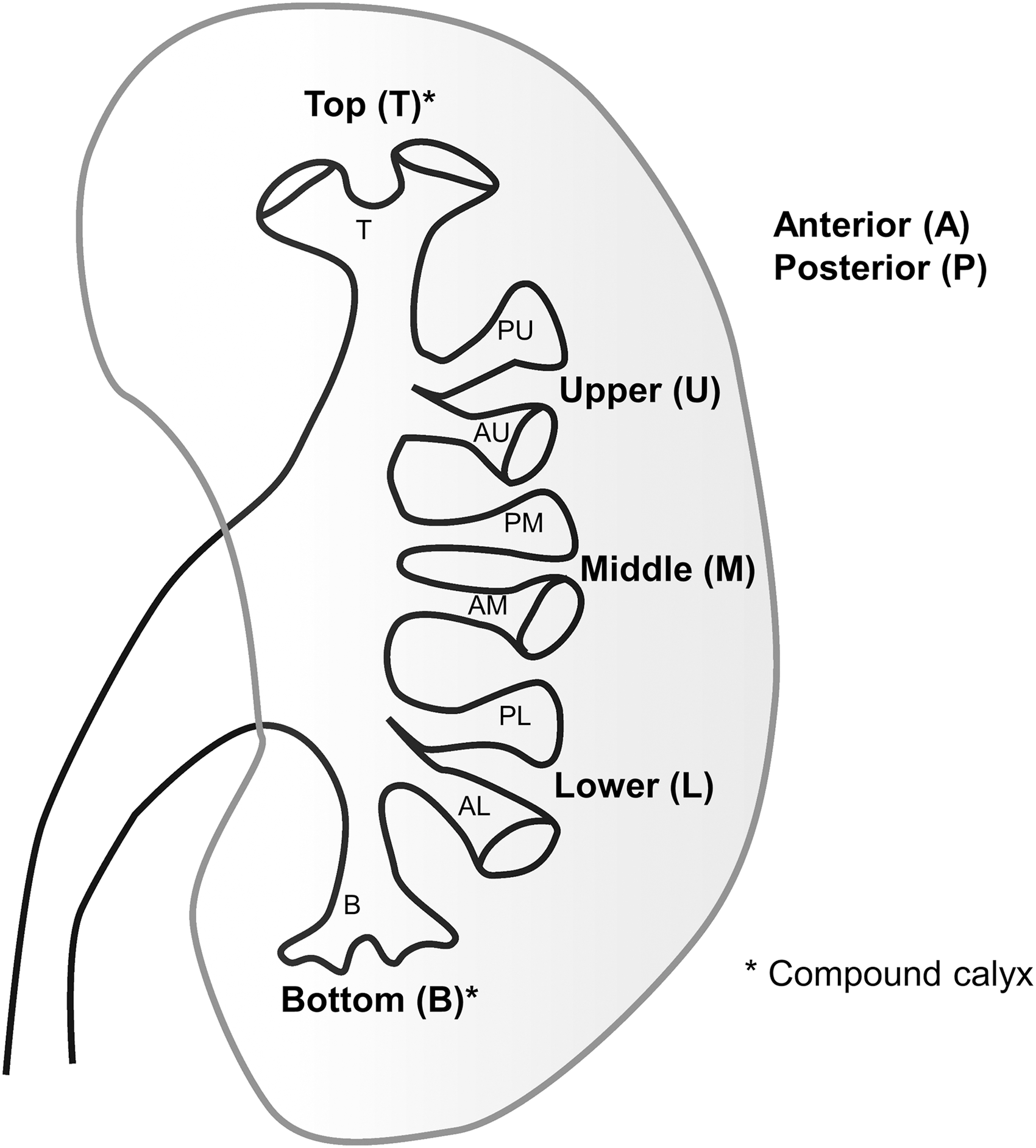
Nomenclature of renal calices: There are five classifications for each minor calix from the upper pole: top (T), upper (U), middle (M), lower (L), and bottom (B). U, M, and L in the mid kidney are arranged in anterior (A) and posterior (P) pairs.
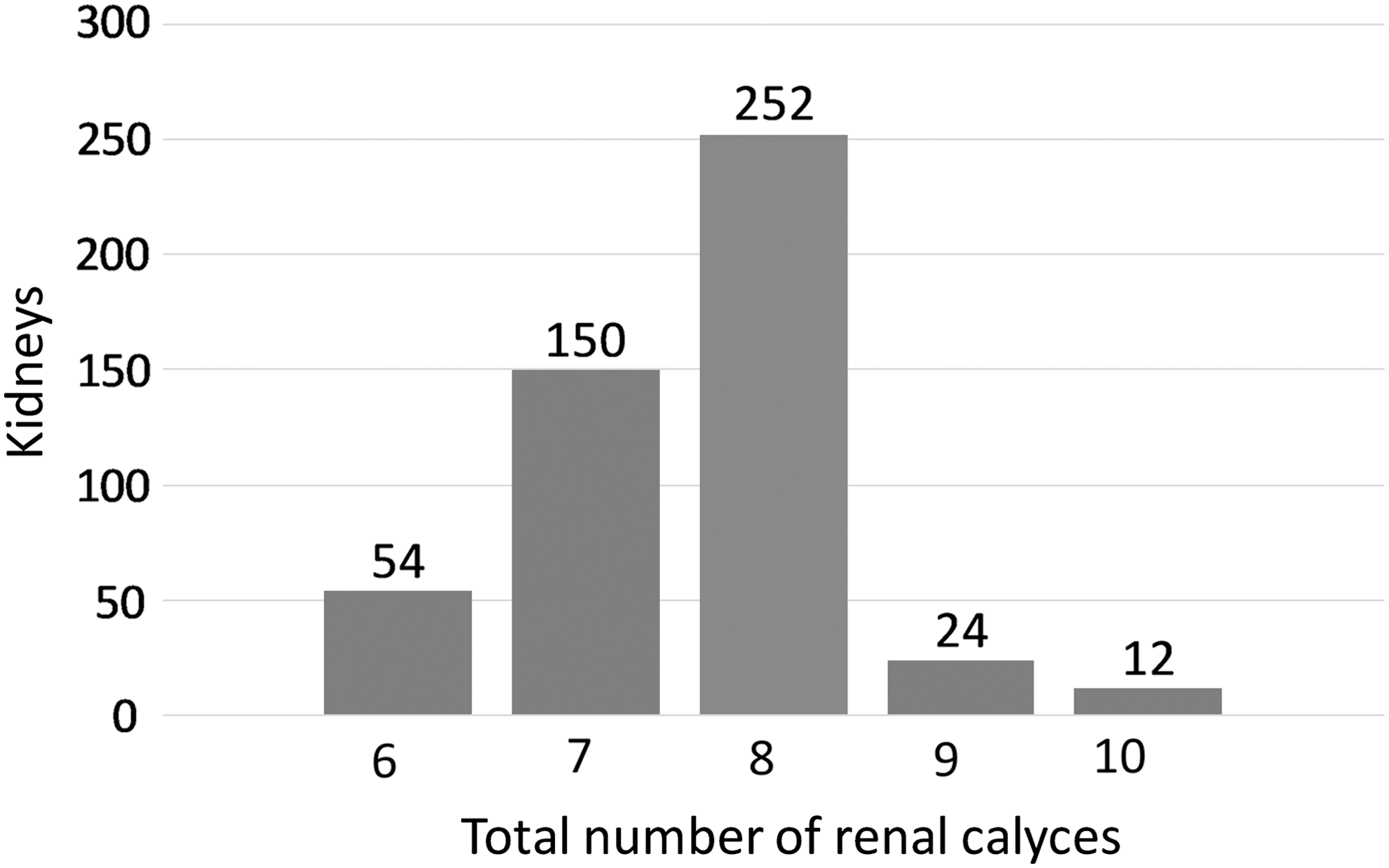
Graphic representation of the total number of renal calices.
Next, according to the branch patterns of the pelvis, the morphology of the pelvis was classified into two major types: type I, single pelvis (58%, 286/492); and type II, divided pelvis (42%, 206/492) (Fig. 3). The type II pelvis was bifurcated into two branches, the upper branch (top and upper) and the lower branch (middle, lower, and bottom). The bifurcation point was always between the upper and middle. If the branch point was inside the straight line between the top and bottom, the pelvis was considered to be type II. In addition, type I was subclassified into three subtypes (Ia, Ib, and Ic) according to the width of the pelvis (Fig. 4). The type Ia subtype was the most frequently observed standard morphology (43%, 212/492). The type Ia formed a typical funnel-shaped pelvis and a middle calix was usually located in front of the axis of the renal pelvis. In type Ia, the width of the pelvis was typically about three times larger than that of the ureteropelvic junction (UPJ). The type Ib subtype was a wide pelvis morphology (4%, 20/492). The type Ib formed a large box-shaped pelvis and usually had more minor calices in the mid kidney. If the width of the pelvis was 5 to 10 times larger than the width of the UPJ, the pelvis was considered to be type Ib. The type Ic subtype was a narrow pelvis morphology (11%, 54/492). The type Ic formed a slim line-shaped pelvis. If the width of the pelvis was 1.5 to 2 times larger than the width of the UPJ, the pelvis was considered to be type Ic. Table 1 shows a summary of our classifications. Figure 5 shows representative images of CT-urography for each type.
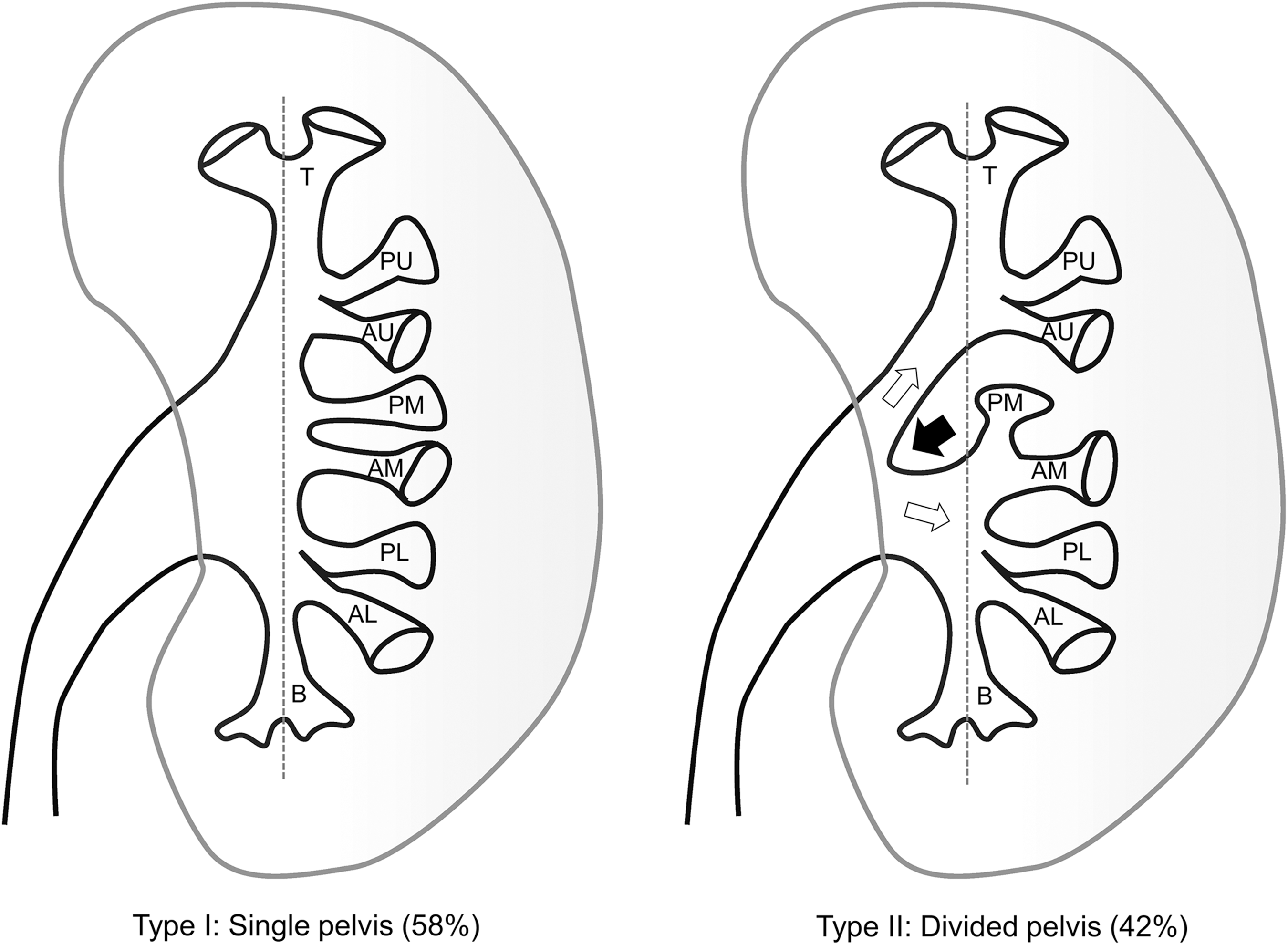
The two major types of renal pelvis: type I and type II. Black arrow represents the bifurcation point of pelvis. White arrows represent the upper and lower branches.
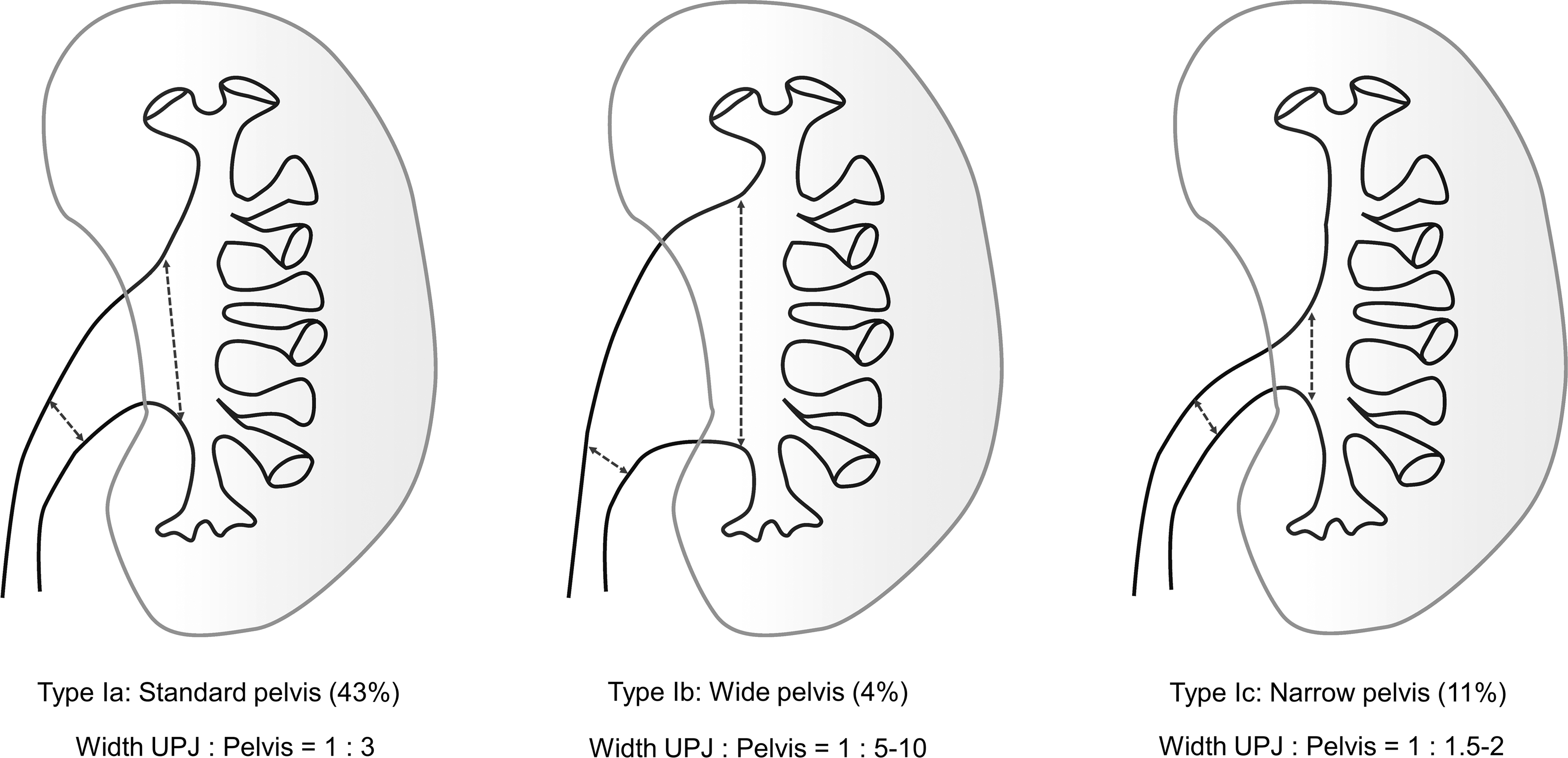
The three subtypes of type I: type Ia, type Ib, and type Ic.

The four types: type Ia, type Ib, type Ic, and type II. Each type is represented by an illustration of the case with a total of eight renal calices. Representative images of CT-urography are also presented. Black dotted arrows represent the width of UPJ and pelvis. White dotted line represents the straight line between top and bottom.
If you are unsure whether a pelvis should be classified as type I or type II, draw a straight line between the top and bottom. When the branch point is inside the straight line, it is usually considered to be type II.
UPJ = ureteropelvic junction.
Among the 227 cases in which both the right and left kidneys could be evaluated, the right and left kidneys had the same morphology in 139 cases (61%).
The reproducibility of this classification was assessed using the free marginal kappa coefficient. The inter-rater agreement of the procedures was 0.91 (percentage of overall agreement, 93.3%), indicating “adequate” inter-rater agreement (kappa >0.70). The most common area of disagreement was between type Ia and type Ic.
Discussion
With recent advances in endoscopic instruments, ureteroscopy has become an essential technique in urologic examinations. Although the rate of ureteroscopic surgery is rapidly increasing, anatomical study of the pelvicaliceal system is a “forgotten domain,” which has not been updated for more than a quarter of a century. 9,10 At present, urologists are facing a dilemma in that although the latest ureteroscopes enable them to observe the entire upper urinary tract, the surgical findings cannot be sufficiently described. In other words, the lack of a generalized nomenclature for each minor calix—a specific and reproducible description method that can be commonly understood by everyone—prevents the sharing of accurate information.
We herein propose a nomenclature based on the analysis of a number of 3D CT-urography images, which classifies each minor calix into five levels: top (T), upper (U), middle (M), lower (L), and bottom (B), with the upper, middle, and lower levels each further divided into anterior (A) and posterior (P) pair arrangements. The morphology of the renal pelvis is classified into two major types: type I, with single pelvis, and type II, with a divided pelvis. The type I morphology has three further subclassifications, wherein type Ia describes the most common, funnel-shaped pelvis, type Ib describes a wide box-shaped pelvis, and type Ic describes a slim line-shaped pelvis. We identified the reproducibility of our classification by calculating the kappa coefficient and proved that it was adequate (kappa >0.70).
In 1901, Max Brödel, a medical illustrator, reported the anatomy of the renal pelvis and vessels, along with many precise illustrations. 11 He clearly described two types of renal pelvis: the true pelvis and the divided pelvis. He also illustrated the ideal forms of these two types with eight calices. These two illustrations were absolutely consistent with our proposed type I and type II morphologies. We also agree the most common total number of renal calices is eight. Although Brödel did not consider the nomenclature for each renal calix, we explain the variation in the total number of renal calices counting the uppermost and lowermost compound calices as one calix (top and bottom), with some variation in the number of calices in the mid-kidney (upper, middle, and lower). To the best of our knowledge, there has not been any study on this topic and we have first reported the ratios of the two morphologic types of pelvis and the total number of renal calices.
In the type II morphology, the bifurcation point is always between the upper and middle levels. Figure 6 shows a case of double ureter. In the case of double ureter, the upper ureter always has fewer calices than the lower. This rule indicates that the upper and lower branches in type II are consistent with the upper and lower ureters in double ureter, respectively. Thus, from an embryologic point of view, we are confident of the rationale to distinguish between type I and type II in our classification.

Image of a double ureter case.
The classification proposed by Sampaio in 1988 is currently the most widespread morphologic classification of the pelvicaliceal system. 10 Sampaio classified the pelvicaliceal system into two major groups (A and B) with two subtypes in each major group (A1, A2, B1, and B2), based on the renal calix that the urine produced in the mid-kidney passes through. The reason why Sampaio's classification is not sufficiently widespread is probably because it is difficult to intuitively understand and because it is not practical for endoscopic surgery. 12,13
We believe that our classification will be useful for the planning of endoscopic treatment strategies for large renal stones according to the type. For example, in a complicated case involving a staghorn stone requiring percutaneous nephrolithotomy (PCNL), patients with a type II (divided pelvis) morphology may require an upper pole tract because a rigid nephroscope cannot access the upper branch through the lower pole tract (Fig. 7). Recently, Sofer et al. studied the accessibility of the upper calix through a lower calix tract during supine PCNL. 14 They concluded that an acute angle between the lower calix and the upper calix is the single independent factor associated with accessibility. Although typical photographs showing an acute angle case and a wide angle case are presented in the article, these cases precisely fit the type I and type II morphologic classifications of our system. In general, upper pole access and multiple tracts are risk factors for complication in PCNL. The Clinical Research Office of the Endourological Society analyzed the outcomes of PCNL with upper pole access. 15 They concluded that patients should be carefully selected and informed about the higher risk of morbidity associated with upper pole access. We agree with their conclusions and emphasize the rationale for distinguishing between the type I and type II morphologies in our classification system. We also believe the significance of subclassification in type I. Type Ib, which resembles the shape of UPJ stenosis, should be distinguished from the other, because of its difficulty of spontaneous passage of stone fragments or dust. Thus, when we perform ureteroscopic lithotripsy in the case of Type Ib, we should extract almost all stone fragments as possible. The dusting technique may not be appropriate for type Ib because the dust may deposit on the bottom. In contrast, type Ib is easy to access when we perform PCNL. In the case of type Ic, which has a small pelvis, we should take an attention not to damage the pelvic wall by relatively larger size tract in PCNL. When we perform ureteroscopy in the case of type Ic, the procedure may be cramped and a Double-J stent may not form a proper loop in the pelvis.
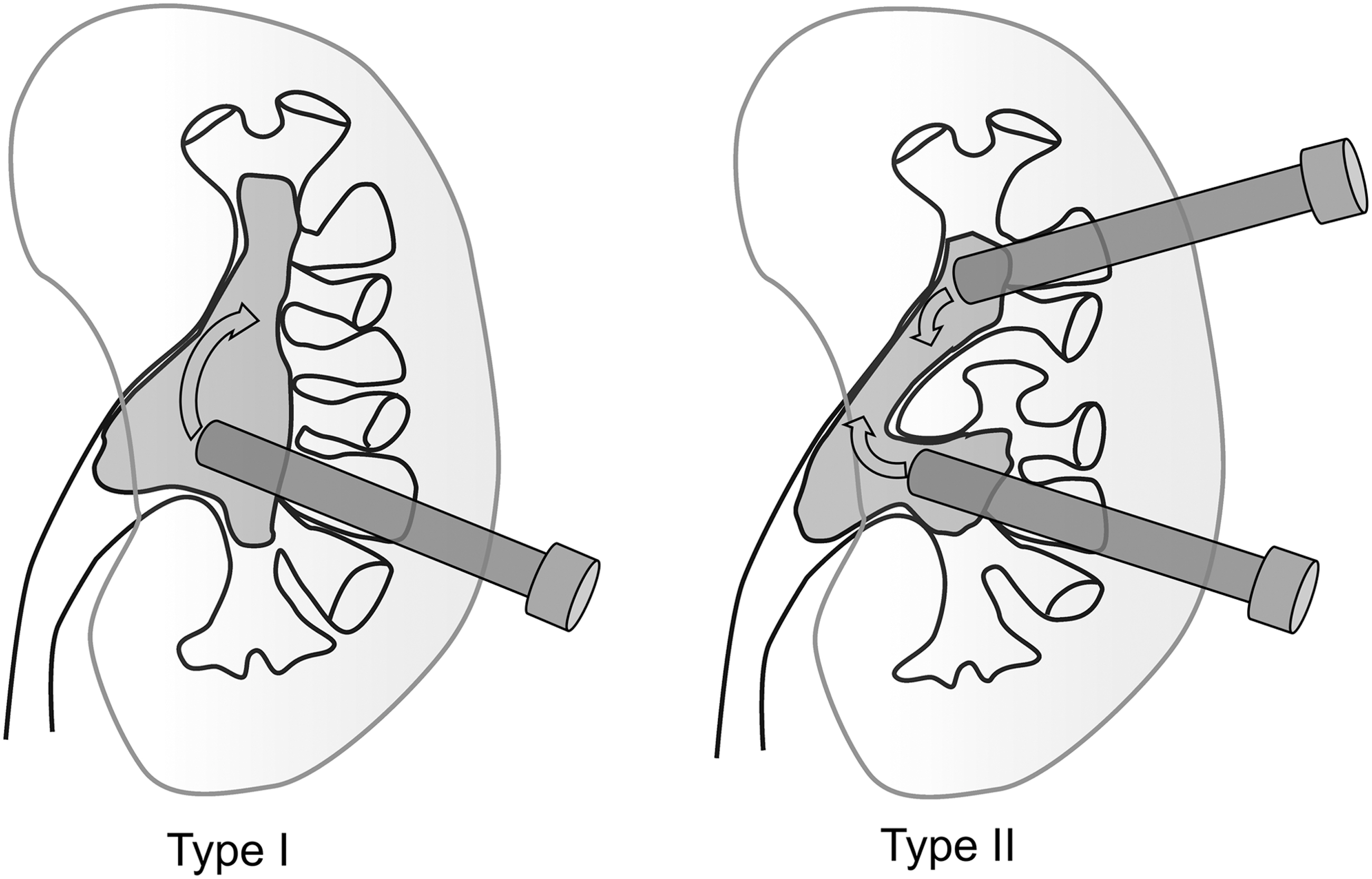
Illustrations showing an accessibility from lower pole tract to the upper pole during percutaneous nephrolithotomy for staghorn stone in type I and type II.
Currently, several regular follow-ups by ureteroscopy are required for conservative surgery for upper tract urothelial tumors. 4 Thus, it is important to accurately and reproducibly describe the position of the original tumor in medical charts. We believe that the use of our classification system enables the specific and reproducible description of surgical findings.
This study is associated with some limitations. First, CT-urography may not reproduce the renal pelvis precisely. Thus, we excluded cases that were difficult to evaluate because of hydronephrosis or large renal cysts from this study. Second, although our statistical analysis indicated the reproducibility of our results, a boundary exists between each morphologic type, which would be judged subjectively by the evaluator. However, there would be no morphologic classification without a boundary in any field. Third, the clinical usefulness of our classification system requires further investigation. Many endoscopic surgeries were performed upon kidneys with some morphologic abnormality, not normality. We always check the morphology of the pelvis during lithotripsy and find that the types do not change, even if severe hydronephrosis occur. In the case of severe hydronephrosis or complete staghorn stone, divided pelvis (type II) is still divided. Also, the same comment can be said in the subclassification of type I. Type Ib is not a deformity caused by hydronephrosis because each calix is not expanded. Regarding type Ic, some patients with struvite form complete staghorn stone in the shape of type Ic. In this way, our proposed classification can be applied to clinical use including some anatomical deformities. However, the exception case in our classification is horseshoe kidney. The horseshoe kidney is caused by another embryologic abnormality. As a next step, we are planning to validate our findings in a multicenter study and to examine the impact of each morphologic type on the treatment outcome.
Conclusions
This anatomical classification system can name each minor calix and divide the renal pelvis into two major types: types I (single pelvis) and II (divided pelvis) based on the branch patterns. Type I is subdivided into three types (Ia, Ib, and Ic) based on the width of the single pelvis. We once again recognized the correctness of Brödel's findings and proposed a simpler and practical classification. This classification system enables the sharing of common intrarenal information, thus leading to the development of concrete treatment strategies.
Footnotes
Author Disclosure Statement
No competing financial interests exist.