
Abstract
Introduction:
We set out to investigate whether general anesthesia with low ventilation (LV, respiratory rate ≤8/minute and tidal volume <500 mL) could reduce renal mobility and thereby facilitate improved retrograde intrarenal surgery (RIRS) compared with general anesthesia with standard ventilation (SV).
Materials and Methods:
All 60 consecutive patients who presented for RIRS in our department from September 1, 2017 to December 31, 2017 were prospectively randomized 1:1 into one group that was selected to receive SV and another that received LV. Significant factors influencing the study endpoints considered fragmentation rate (FR), removal rate (RR), processing rate (PR), and operating rate (OR), were statistically analyzed for the whole group as well as for comparison by level of surgeon expertise.
Results:
Univariate analysis revealed that LV was a significant factor in improving all endpoints. Some endpoints were also affected by the stone's volume, number, and density as well as the surgeon expertise. LV remained the single independent factor for FR, RR, and PR in the multivariate analysis. LV significantly improved all four of the fellows' endpoints (p < 0.05 for each) and positively influenced the expert's RR (p = 0.04), PR (p = 0.02) and OR (p = 0.04). The performance gap between the fellows and the experts narrowed under LV. The end-tidal CO2 was significantly higher in the LV group (50 vs 36 mm Hg; p < 0.0001), however, without any clinical significance. The overall stone-free rate (97%) and complication rate (5%) were not significantly different between the two groups. The patient's anesthesia-related safety was not affected by the mode of ventilation as evidenced by no need to convert from LV to SV during the procedures.
Conclusions:
LV during RIRS has a significant positive impact on the overall improvement of surgical performance and effectiveness. It does not negatively affect the patient's anesthesia-related safety and may contribute to considerably improving the performance of in-training endourologists.
Introduction
C
The surgeon's skills and experience are highly influential factors for executing an effective procedure. To achieve an even minimal level of proficiency in performing RIRS, a urologist reportedly needs to perform 40 to 60 procedures. 7,8 Models, hands-on courses, workshops, residency, and fellowship programs are widely available for this purpose. 7 They focus on preparing the urologist to perform the procedure, but do not consider the ventilation-related renal movements as a factor that may be changed. In our opinion, this issue warrants greater attention, as targeting an unpredictably mobile stone may negatively influence the effectiveness of the procedure.
There is a direct link between ventilation during general anesthesia and the mobility of the kidney during surgery, but surprisingly little appears in the literature with regard to the influence of ventilation on the execution of RIRS. We believe that modulating ventilation toward a respiratory-gated mode during general anesthesia, in cooperation with the anesthesiologist, to reduce renal movement may significantly enhance the execution and outcome of RIRS. We designed the present study to prospectively and randomly compare the effectiveness of RIRS performed under two ventilation modes, low rate-low tidal volume (low ventilation [LV]), and standard ventilation (SV).
Patients and Methods
The study was approved by the Institutional Review Board (IRB), and the participating patients signed informed consent. All patients presenting for RIRS from September 1, 2017 to December 31, 2017 were consecutively enrolled. The procedures were performed under general anesthesia with full mechanical ventilation, and the use of muscle relaxants while maintaining a steady stage 3 anesthetic status. 9 The patients were prospectively randomized 1:1 into two groups by means of the block randomization method that allows formation of comparison groups with equal numbers of patients. 10 One group was operated under ventilation rates and tidal volumes independently chosen by the anesthesiologist (SV), while the other group was operated under a ventilation rate of ≤8/minute and a tidal volume <500 mL (LV). LV was started before initiating the fragmentation and maintained along the stone removal process until the impression that a stone-free status was achieved. The anesthesiologists could convert from LV to SV any time if mandated by the patient's condition. In addition, there was a 2:1 allocation by the surgeon's expertise, that is, two fellows (accredited fellowship following 1-year program Endourological Society) to one expert (director of Endourological Society accredited fellowship program), to assess whether the ventilation mode had any impact on surgeons with different levels of endourologic experience.
Preoperative stenting was performed solely when there were urgent indications (e.g., intractable pain, infection, and renal failure). The procedures were performed with the patient in the lithotomy position, and with a safety guidewire (0.035″ Sensor™; Boston Scientific, Marlborough, MA) along a ureteral access sheath (11/13F × 36 cm Navigator™; Boston Scientific). The intrarenal collecting system was approached with either analog or digital 7.5/8.5F Flex X2™ ureteroscopes (Karl Storz, Tuttlingen, GE), and the stones were fragmented with a holmium laser using 365 nm fibers at 0.6 J and 20 Hz (Lumenis® MOSES Pulse™ 120H; Lumenis, Yokneam, Israel). The MOSES technology was not used to allow free mobility of the renal stones during laser application. Caliceal stones were treated in situ. Fragments with an estimated diameter of < 4 mm were extracted by baskets (1.9–2.4F Zero Tip™; Boston Scientific), until it was the operator's intraoperative impression that the patient was stone-free. At the end of the procedure, 7F, 24 to 28 cm Double-J stents with external strings (Pecuflex™; Boston Scientific) were placed for 5 to 7 days and then extracted by the patients. All patients were followed-up at 2 months with noncontrast computed tomography (NCCT), urinary culture analysis, serum creatinine measurement, and stone composition assessment.
The data collected for statistical analysis included demographics, side, American Society of Anesthesiologists (ASA) score, body mass index, stone size (largest diameter in mm), stone volume (mm3) as calculated by three dimensions on the preoperative NCCT, stone density (HU), number of stones (single vs multiple) and location (pelvis vs calyces), prestenting (yes vs no), expertise (fellow vs expert), mode of ventilation (SV vs LV), end-tidal CO2 at the end of the procedure, complications, and stone-free rate (SFR) at the 2-month visit. The endpoints considered as being dependent factors were: - fragmentation rate (FR), calculated as stone volume divided by fragmentation time (mm3/minute) - removal rate (RR), calculated as stone volume divided by basketing time (mm3/minute) - processing rate (PR), defined as stone volume divided by the entire stone processing time (mm3/minute) - operating rate (OR), defined as stone volume divided by operating time from the initial insertion of the cystoscope until the final placement of the Foley catheter in the bladder (mm3/minute)
Times for FR and RR were taken by an observer resident who used a digital timer. The PR time was calculated as the sum of FR and RR, and the OR time was that noted by the assistant nurse in the computerized file of the patient.
Descriptive statistical analyses were assessed by box plots presenting median, range and standard deviation. Distribution was analyzed depending on normality by either the Student t-test or Mann–Whitney U test. Levene's test was used for equality of variances and the t-test for equality of means. A univariate analysis was conducted by linear models to detect factors significantly associated with the study endpoints (significance considered at p < 0.05). Significant factors found by univariate analysis were tested in linear stepwise logistic regression models to define their independence and they were reported as p-values, odds ratios, and 95% confidence intervals. All statistical analyses were performed using SPSS (IBM Corp., released 2013, IBM SPSS Statistics for Windows, version 22.0; IBM Corp., Armonk, NY).
Results
A total of 192 ureteroscopic procedures were performed during the 4-month study period, and all 60 patients who were referred for RIRS (31%) were consecutively enrolled. The cohort was equally divided between patients who underwent general anesthesia with LV and those who received SV. Twenty-nine (48%) patients underwent preoperative stenting. The two study groups were similar in demographics, baseline clinical data, and surgeon expertise (Table 1). The mean ventilation rate and tidal volume were 11.2/minute and 515 mL, respectively, for SV and 6.2/minute and 419 mL, respectively, for LV. Descriptive statistics, including median, range, and standard deviation for fragmentation, removal, processing, and end-tidal CO2 are presented as box plots in Figure 1. The mean end-tidal CO2 at the end of the operation was significantly higher in the LV mode compared with the SV mode (50 vs 36 mm Hg; p < 0.0001). LV was significantly associated with increased effectiveness of FR, RR, PR, and OR by mm3/minute in the univariate analysis (Table 2). The mode of ventilation remained the sole independent factor associated with better FR, RR, and PR, but not OR, in the stepwise logistic regression analysis (Table 3). There were no other independent factors that affected our defined endpoints.
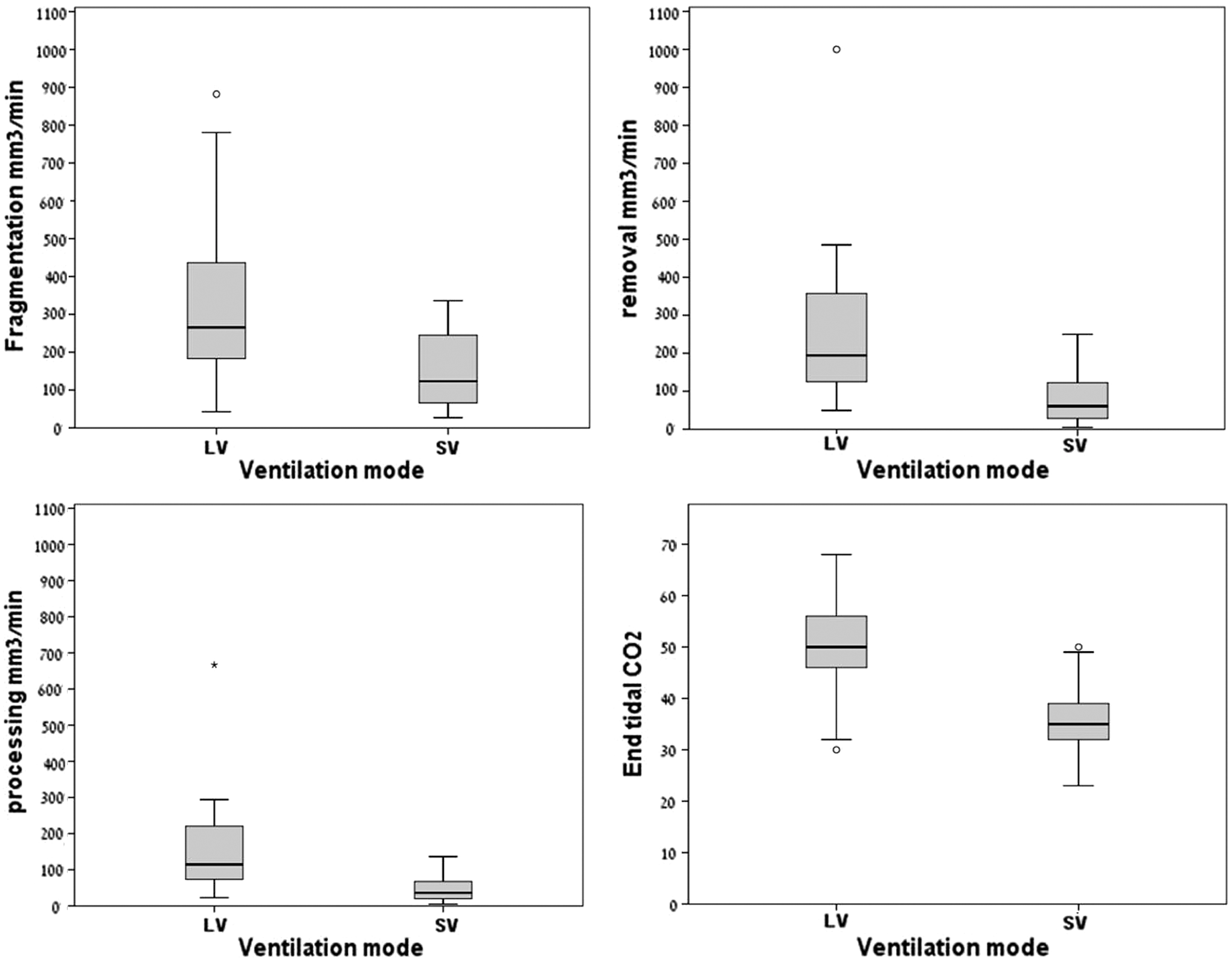
Box plot analyses displaying overall medians, ranges, and standard deviations for the comparison groups. LV = low ventilation; SV = standard ventilation.
ASA = American Society of Anesthesiologists; BMI = body mass index; LV = low ventilation; SD = standard deviation; SV = standard ventilation.
Boldface indicates statistically significant values.
FR = fragmentation rate; OR = operating rate; PR = processing rate; RR = removal rate.
A second analysis was designed to evaluate the influence of the ventilation mode by surgeon expertise. The results showed that LV did not influence the expert's FR (p = 0.11), but that it significantly improved his RR (p = 0.04), PR (p = 0.02), and OR (p = 0.04). The overall operation time was significantly shorter when the surgery was performed by the expert (44 vs 54 minute for the fellow, p = 0.04). The expert performed significantly better than the fellow in the SV mode, however, the fellow's performance was significantly improved in the LV mode, thus reducing the gap between him and the expert who maintained only a slight lead (Table 4). The overall SFR was 97%, and there was no significant difference between the two study groups. The two patients with residual stones were retreated endoscopically. There were three (5%) complications, including two urinary tract infections (Clavien–Dindo grade II) and one readmission for stent insertion in a patient with stones' road (Clavien–Dindo grade IIIb). None of the patients in the LV group developed side effects or complications related to the higher levels of end-tidal CO2, and there were no conversions from LV to SV related to CO2 accumulation, all confirming the absence of any threat to patient safety.
Boldface indicates statistically significant values.
Discussion
Treatment of moving organs requires the application of maneuvers to reduce and control organ motion to focus the therapy on the point of interest (e.g., tumor, stone, and vessel,), while avoiding any reduction in the delivery of effective therapy and damage to the surrounding structure. This issue was initially addressed in the development of safe and effective methods for stereotactic ablative body radiotherapy delivered to the lung, liver, pancreas, adrenals and kidneys. 11 Lessons learned from these studies using computed tomography, magnetic resonance imaging, or ultrasonography for assessing respiratory-related kidney movements during various modes of spontaneous respiration showed that kidneys move up to 50 mm in the craniocaudal axis, 8.2 mm in the anteroposterior axis, and 6.2 mm laterally. 11 –14 This renal motion is of critical significance when treating renal stones, and it had been addressed in the field of urology mainly in relationship to extracorporeal shockwave lithotripsy (SWL). 15 –21 Studies that assessed stone movements during SWL that were carried out on patients who were solely under analgesia while spontaneous respiration was maintained revealed that respiration-related stone movements ranged from 7.7 ± 2.9 to 40 ± 11 mm. 15,16 Sorensen and colleagues 17 ultrasonographically measured stone mobility in 10 patients undergoing SWL under general anesthesia and reported a respiration-related stone movement of 15 ± 3 mm, resulting in a 40% rate of shockwave-missed stone. The discrepancies in these measurements are probably the result of different imaging methods that had been used for assessing stone movement. However, the facts remain that this stone motion influences the results of SWL, and that the success rates are improved with less stone movement. 15 –17
Various methods of reducing respiratory-related renal and, subsequently, stone motion were assessed to improve the success rate of SWL. Honey and colleagues 18 studied the use of compression belts, while Bohris and colleagues 19 proposed the use of specially designed compression plates that do not limit the delivery of shockwaves. Both of those groups reported significant improvement in SFRs when using those methods. Another reported way of reducing respiratory-induced renal motion during SWL was the use of high-frequency jet ventilation (HFJV). 21,22 One retrospective study that compared HFJV to spontaneous ventilation in 91 SWL-treated patients showed a significant reduction in the number of shockwaves needed for fragmenting the stone when the patients were under anesthesia with HFJV (median, 2000 vs 3000, p = 0.0001). 22
Similar to SWL, RIRS is performed in a moving surgical environment. As such, the surgeon encounters similar difficulties in targeting mobile stones. The stone motion in RIRS is caused by the holmium laser's photoacoustic retropulsion as well as by the respiratory-related renal motion. A novel and promising technology named MOSES (Lumenis) was developed to significantly reduce stone migration related to holmium laser retropulsion. 23 However, ways to change the ventilation mode to improve RIRS outcomes have not been studied in depth. Preliminary results presented at the Worlds Congress of Endourology 2017 revealed a trend toward shorter operative time and better SFRs when using HFJV in comparison to standard assisted ventilation during RIRS. 24 Emiliani and colleagues 25 reported the feasibility and potential advantage of complete interruptions of ventilation to stop renal movements during RIRS. Their technique involves general anesthesia, preparation with 100% oxygen for few minutes, followed by up to 5 minutes of apnea that facilitates treatment in a nonmoving kidney. Although published as a point of technique without a formal assessment of a study group, those authors reported no complications related to increased levels of end-tidal PCO2.
To the best of our knowledge, no other studies have addressed the problem of renal motion during RIRS. As such, our study contributes important and novel data in support of the rationale that reducing the ventilation rate and the tidal volume will result in decreased kidney and subsequently stone motion and may improve the effectiveness of RIRS. We observed that LV significantly increased fragmentation, removal, processing and ORs, as well as reduced operative time. Our explanation for failing to show that LV independently influenced OR is that, in addition to treating stones, RIRS includes the steps needed to achieve adequate access to the stone. These steps are sometimes difficult to accomplish with limited expertise, such as the identification of ureteral orifice obscured by prostatic enlargement, the presence of a narrow ureter, the presence of impacted stone at the pelvi-ureteral junction, and more. In some of the cases in the current work, the preparatory steps were performed by the expert until the ureteroscope was properly positioned for initiating fragmentation, and only then was the procedure transferred back to the fellow and continued as dictated by randomization. This inevitable attitude probably contributed to blurring of the proper effect of LV on OR.
The benefit of LV was especially prominent in improving the fellows' performances. In our opinion, this finding indicates that dealing with a moving stone in the intrarenal collecting system is the most advanced skill required for performing an effective RIRS. It is possible that the relatively small number of cases operated by the expert in our series did not allow for a reliable assessment of LV impact on his performance.
We are aware that this study has several limitations, such as the relatively small number of patients in the two groups and the lack of performing a sample size calculation. These limitations were the result of our intent to conduct the study in a prospective randomized way and within a limited period of time. Another potential limitation is our not having collected data on radiation exposure. One may expect that improving stone fragmentation and removal effectiveness and shortening the operative time may result in reduction of intraoperative fluoroscopy time. This issue warrants assessment in further studies. Despite these limitations, we believe that this study contributes to better understanding of stone motion during a respiratory cycle and may thereby help in further development of systems for stone tracking and controlled triggered laser firing systems gated to the ventilation phases. Finally, close cooperation with the anesthesiology team is a prerequisite for the achievement of reliable LV modes.
Conclusion
We were able to show that LV during RIRS appears to have a strong positive impact in improving the effectiveness of kidney stone treatment. LV did not negatively affect patient safety during anesthesia, and we suggest that it may considerably improve the performance of the in-training of future endourologists.
Ethical Statement
IRB approval was obtained for this study and patient informed consent was obtained before undergoing the procedures.
Footnotes
Author Disclosure Statement
No competing financial interests exist.