
Abstract
Objective:
Renal pelvic pressure (RPP) is expected to rise during percutaneous procedures. A very small tract size was expected to bring high RPP, and super-mini percutaneous nephrolithotomy (SMP) uses a 14F sheath, which is even smaller than that used in mini-percutaneous nephrolithotomy, so the RPP in SMP was more worrisome. Interestingly, the sheath had suction, which aimed to decrease the RPP, so we measured the RPP in an in vivo model to explore the relationship of implying negative pressure through the sheath with the RPP.
Methods:
Seventy-four consecutive patients were enrolled for RPP measurement during SMP between April 2016 and July 2017. Prospective RPP measurements were recorded using the MINDRAY-PM9000 monitor by connecting its baroceptor of the invasive blood pressure channel to a retrogradely inserted renal pelvic open-ended ureteric catheter. RPP data were collected each second by a computer program. All data were evaluated statistically with SPSS 13.0 software.
Results:
During SMP with a 14F irrigation–suction sheath, the average RPP was 19.51 ± 5.83 mm Hg. The median accumulative time of RPP ≥30 mm Hg was 55 (3–345) seconds. Postoperative fever was recorded in four patients (5.4%). A receiver operating characteristic -curve analysis showed that when suction pressure was set to 0.03 Mpa (≈230 mm Hg), irrigation pressure between 200 and 250 mm Hg, and the irrigation flow to 320 mL/minute, the accumulative high RPP was more likely <50 seconds, and the sensitivity and specificity were 75.0% and 66.7%, respectively.
Conclusions:
The RPP in SMP remains <30 mm Hg. Controlling the pressures as well as the flow of irrigating saline is important for the safety and efficiency of percutaneous procedures.
Introduction
P
Super-mini percutaneous nephrolithotomy (SMP) was developed in this current form to address many of these deficiencies. The sheath is small to decrease bleeding risk. Suction is applied through the sheath to immediately remove stone fragments, combined with sufficient irrigation to quickly wash out the stones and mintain low RPP. 9
Little is known about RPP and cumulative RPP time during SMP and any correlation it might have with the postoperative outcomes. We measured the RPP during SMP to determine whether it will maintain a low RPP and/or improve the incidence of postoperative infectious complications.
Patients and Methods
After approval of the Institutional Ethics Committee of the First Affiliated Hospital of Guangzhou Medical University and between April 2016 and July 2017, 74 consecutive patients (48 men and 26 women, with a mean age of 45.74 ± 13.44 years) were enrolled. Informed consents were taken from the involved patients. Included cases were 18 years or older with symptomatic renal calculi that is 25 mm or less and American Society of Anesthesiologist (ASA) anesthesia scores of 1 or 2. Patients with preoperative symptoms of infection (fever, chills, rigors, etc.), hydronephrosis, previous kidney transplant or urinary diversion, or congenital anomalies that may affect the RPP were excluded. All patients had undergone a definitive diagnosis preoperatively by non-contrasted computed tomography (NCCT) of the urinary tract. Any patient with positive preoperative urine culture was treated with appropriate antibiotics according to the culture antibiogram for 3 to 5 days. All patients with negative urine cultures were given a single prophylactic dose of broad spectrum antibiotics on call to surgery. The data collected from these patients included demographic characteristics; stone data (size, location, and composition); and operative and recovery parameters.
The stone burden was calculated from NCCT by multiplying the largest diameter of the largest stone (or the sum of diameters in the case of multiple stones) by the largest width. Operation time was recorded from the first percutaneous puncture to the completion of stone removal. Hospital stay was rounded to the nearest whole day from the day of surgery to the day of discharge. Rate of hemoglobin (Hb) drop was assessed by subtracting the postoperative Hb level from the preoperative one. Primary stone-free rate (SFR) and final SFR was assessed by KUB (kidney, ureter, and bladder radiograph) or ultrasound at day 1 and urinary tract NCCT at 1 month after the operation, consecutively. Stone-free status was considered if no stones were visible on corresponding imaging modality. Removal of Double-J stent was done in an outpatient setting after 2 weeks (in case a Double-J stent was inserted). Bleeding severity was judged by the treating physician, and transfusions were administered according to local practice guidelines. Complications were recorded according to the modified Clavien classification system. 10
SMP technique
We have published our SMP technique in previous publications. 9,11 Briefly, under general anesthesia and with the patient in the lithotomy position, an open-ended 5F ureteral catheter was advanced into the renal pelvis under direct vision. Then prone position was attained. Percutaneous puncture, under either fluoroscopic or ultrasonic guidance, to the desired calyx was done using an 18-gauge coaxial needle. After successfully gaining access, dilatation of the tract was carried out with a 10F fascial dilator (a one-step dilatation) over a guidewire. Then an irrigation–suction straight sheath, with an obturator, was advanced over a guidewire and introduced into the pelvicalyceal system. The guidewire was then removed, and the “handle” was connected to the straight sheath. The irrigation port of the irrigation–suction sheath was connected to an irrigation pump, the oblique tube of the sheath was connected to the specimen collection bottle, and the bottle was connected to the negative pressure aspirator.
The suction (negative pressure) was almost always kept at 0.03 Mpa (equivalent to 230 mm Hg), and the irrigation fluid pressure was routinely set between 200 and 250 mm Hg, The irrigation fluid was delivered through the irrigation channel of the sheath. A one-way flow was created as the inflow coming out of the irrigation channel of the sheath was immediately aspirated through the suction conduit of the sheath, becoming an outflow. Stone fragmentation was accomplished using either holmium laser or a small pneumatic lithotripter. The tiny pulverized stone fragments passed around the scope and evacuated through the oblique arm. If the stone fragments were too large to pass around the scope inside the sheath, the scope could be withdrawn slowly to proximal to the bifurcation, creating an unobstructed channel for evacuating larger fragments. At the end of the procedure, a single fluoroscopic image was obtained to assess the stone-free status. A Double-J stent could be placed when appropriate. After making sure no stone residuals were left behind, the sheath could be removed and the wound sealed with absorbable gelatin. For patients with bleeding or extravasation, a nephrostomy tube should be placed.
Measurement of RPP in vivo
After the retrograde insertion of an open-ended ureteral catheter, it was connected to an invasive blood pressure channel of PM9000 patient monitor (Mindray Medical Corporation, Shenzhen, China) with a baroceptor. Then the baroceptor was fixed onto the same level of the renal pelvis; after zero adjustment, the measurement of RPP was started. During the operation, the pressure of the micro Computer Control (MCC) Perfusion Pump was kept as stable as possible, between 200 and 250 mm Hg. The infusion flow ranged from 180 to 500 mL/minute. A computer collected the RPP data each second.
Statistical analysis
Statistical analysis was performed using SPSS software, version 13.0. Continuous normally distributed data were recorded as mean ± standard deviation. Medians with ranges were used for data that were not normally distributed. Categorical variables were compared with the chi-squared test or Fisher's exact test. Receiver operating characteristic (ROC) curves were constructed to evaluate the predictive value of the parameters for high RPP (above 30 mm Hg) more than 50 seconds during SMP. p < 0.05 was considered statistically significant.
Results
Seventy-four patients underwent SMP with the 14F irrigation–suction sheath. Patient and stone demographics are shown in Table 1. Complete stone clearance was achieved in 67 out of the 74 patients (90.5%). The mean operative time was 39.28 ± 24.40 minutes, which ranged from 8 to 110 minutes. Postoperative fever (>38°C) occurred in 4 patients (5.41%) and was resolved by adding intravenous antibiotic to the management (Clavien grade II). Two patients suffered postoperative transient hematuria and resolved spontaneously without further intervention (Clavien grade II). No other complications beyond grade II were noted. Other operative and postoperative findings are shown in Table 2.
BMI = body mass index; PCNL = percutaneous nephrolithotomy; SD = standard deviation; SWL = extracorporeal shockwave lithotripsy; URS = ureteroscopy.
MAP = magnesium ammonium phosphate; SFR = stone-free rate.
All data related to RPP are shown in Table 3. During SMP with a 14F irrigation–suction sheath, the average RPP was 19.51 ± 5.83 mm Hg. The median accumulative time of high RPP (≥30 mm Hg) was 55 (3–345) seconds. The area under the ROC curve was 0.78 (95% confidence interval, 0.640–0.927) (Fig. 1). A cut-off irrigation flow of 320 mL/minute is required to have an accumulative high RPP (≥30 mm Hg) for <50 seconds duration (given that the suction pressure is about 0.03 Mpa [∼230 mm Hg] and irrigation pressure is between 200 and 250 mm Hg). The sensitivity and specificity were 75.0% and 66.7%, respectively.
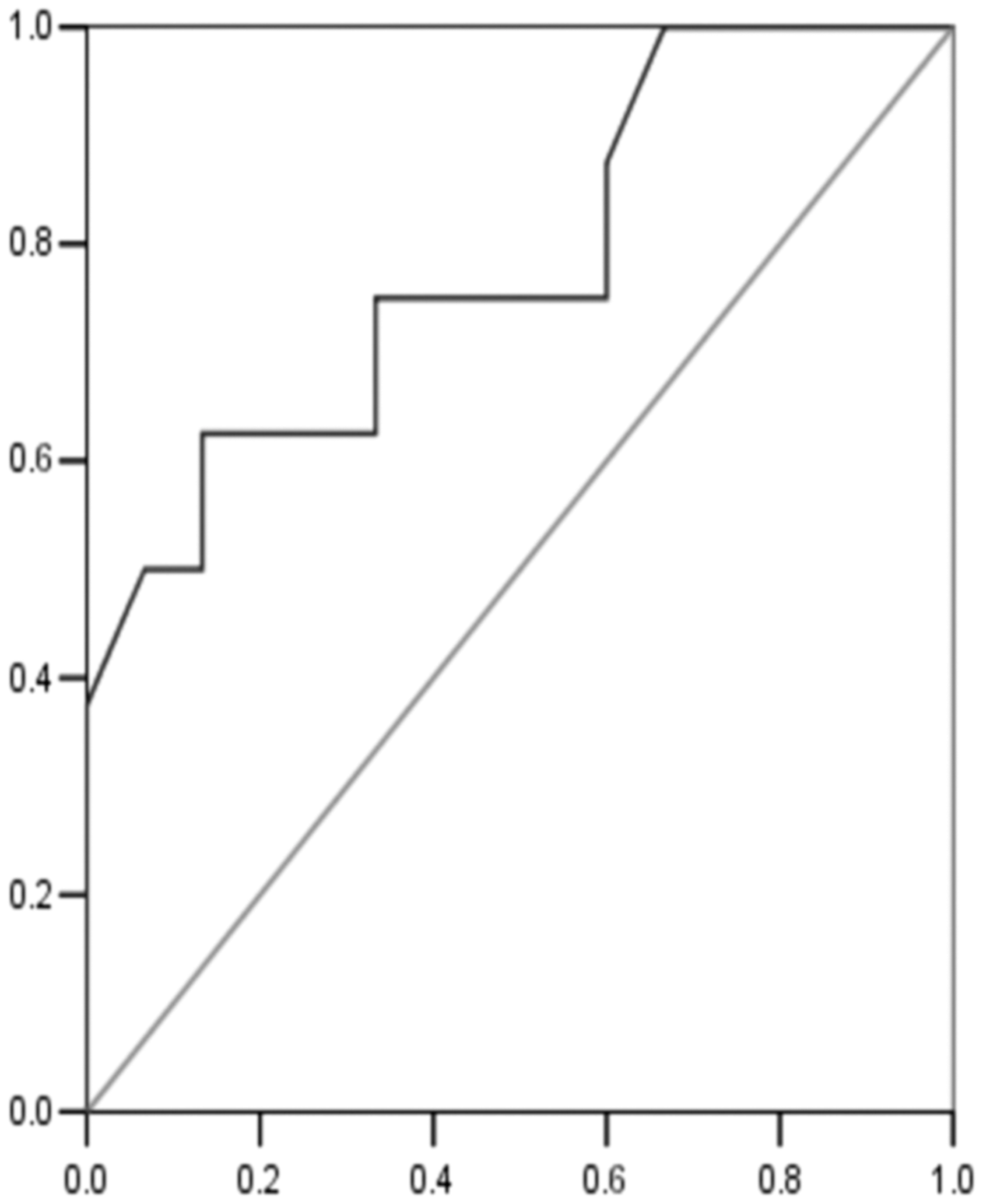
Receiver operating characteristic curve based on the flow of the pump during super-mini percutaneous nephrolithotomy with irrigation-suction 14F sheath index as an indicator of having accumulative renal pelvic pressure ≥30 mm Hg for more than 50 seconds.
The computer generated the sum of high RPP (≥30 mm Hg) readings in the cases.
RPP = renal pelvic pressure.
Further analysis suggested that postoperative fever did not correlate with gender (p = 0.09), age (p = 0.3), infectious calculi (p = 0.42), postoperative serum white blood cell count (p = 0.28), operations longer than 90 minutes (p = 0.14), or one occurrence of RPP ≥30 mm Hg during the operation (p = 0.81). The presence of preoperative urinary tract infection (p = 0.04), mean RPP ≥20 mm Hg (p = 0.01), and accumulative time of high RPP ≥30 mm Hg for ≥70 seconds, meanwhile, had contributed to the postoperative fever occurrence (Tables 4 and 5).
Bold values indicate p value ≤ 0.05.
Bold values indicate p value ≤ 0.05.
UTI = urinary tract infection; WBC = white blood cell.
Discussion
The results of our study using an in vivo model employing patients undergoing SMP has demonstrated that RPP generally remains lower than the backflow level (30 mm Hg) in the course of SMP, with a starting mean of 9.27 ± 3.68 mm Hg that rises after commencement of the procedure to 19.51 ±5.83 mm Hg. About 79.7% (59/74) of patients got at least one reading above 30 mm Hg, and their mean operative RPP (20.51 ± 8.35 mm Hg) still below the threshold. Those elevations in intrarenal pressure were having a computer generated median accumulative time of 55 (3–345) seconds.
Pyelovenous backflow is likely to happen above renal pressures of 30 to 35 mm Hg. 12 The elevation of RPP above the threshold for pyelovenous backflow and the duration of that elevation are among the factors that may result in postoperative fever, sepsis, and systemic inflammatory response syndrome. 8,13,14 Little is known in the literature about an accumulative time of elevated RPP above which postoperative fever is likely to occur. Zhong and colleagues identified a significant rise in postoperative fever when the sum of risings in the RPP (more than 30 mm Hg) is ≥50 seconds in MPCNL and, in the same series, the accumulative time of high RPP (>30 mm Hg) for size 14F peel-away sheath was more than 315 seconds. 8 In this study the sheath is metallic and the suction is applied through the sheath, yet despite having less accumulative high pressure time for the same sized sheath, the RPP in SMP is still higher than that in MPCNL of larger sizes. This can be mainly attributed to the high flow provided by the irrigation–suction sheath of the SMP, especially if there were manipulations in the upper ureter, as the ureteric catheter with the sensor for the pressure is placed in that area.
Moreover, some other factors can be considered responsible for the intermittent rise in the RPP in SMP. As the irrigation outflow goes through the interspace between the scope and the metallic sheath driven by the negative pressure of the suction with almost nothing passing through the ureter, temporarily elevated pressure readings tend to occur when tiny stone gravels accumulate around the nephroscope, inside the sheath, and obstruct the outflow. This could be managed by frequent withdrawals of the nephroscope back into the sheath to allow for the efflux of those gravels. The pressure also gets higher on passing through a narrow infundibulum, but this was not frequent due to the small caliber of the nephoscopy.
On the other hand, maintaining sufficient perfusion is critical for good visualization while performing a PCNL procedure. Surgeons tend to increase saline flow and the pressure of the pump whenever they face difficulties in visualization, which can be a result of having bleeding in most instances. But increasing the pressure and flow will increase the accumulated time of high RPP and the accumulated absorption of fluids and toxins. In our series, the suction pressure was set to about 230 mm Hg, the pump pressure was kept between 200 and 250 mm Hg, and the resultant flow of the irrigating fluid ranged between 180 and 500 mL/minute.
A ROC curve analysis for our values using a cutoff value of 50 seconds for the accumulated high RPP (≥30 mm Hg) confirmed that the most suitable flow, provided that the suction pressure is 230 mm Hg and irrigation pressure of 200 to 250 mm Hg, is 320 mL/minute, around which the accumulated high RPP time is most likely to remain at a procedure time <50 seconds. As a result, the percentage of postoperative fever, 5.4% (four patients), was low. This may stress out the importance of applying negative pressure by using the suction and also having a very small nephroscope. nephroscopy Similar benefits were reported by Yang and coworkers for controlling RPP using suction through the sheath in mini-PCNL. 15
Assuming a cutoff value of RPP to be 30 mm Hg or above for a backflow to happen resulting in absorption of toxins and bacteria would be erroneous or incomplete. it is apparent from our data that the correlation for one reading of RPP ≥30 mm Hg (p = 0.81) is not significant. While having a mean RPP ≥20 mm Hg and more frequent occurrences of high RPP (≥30 mm Hg) for ≥70 seconds during the operation (p = 0.016) would prove that high RPP for longer durations is required to have enough bacterial and toxin loads to cause postoperative infection.
Of note, another technical advantage of the SMP with negative pressure effect is that the stone and its gravels are brought closer to the sheath, minimizing the need for excessive manipulation to chase the stone fragments. As a result, this decreases the chance of having bleeding from imprudent movements with the sheath and decreases the chance of having renal pelvic mucosal injuries that may increase the systemic absorption.
Conclusion
RPP generally remains lower than the level required for a backflow (30 mm Hg) during SMP via 14F irrigation–suction sheath. Less perfusion and higher suction pressures are likely to control the RPP within safe levels. Moreover, controlling the pressure and flow of irrigating saline is essential to maintain the best working environment. Those requirements can be met with the SMP in treating moderately sized renal stones.
Footnotes
Acknowledgments
This work was financed by grants from the Guangzhou Science Technology and Innovation Commission (Nos. 201607010162, 201604020001, and 201704020193); the National Natural Science Foundation of China (Nos. 81670643, 81600542, and 81570633); and the Collaborative Innovation Project of Guangzhou Education Bureau (No. 1201620011).
Author Disclosure Statement
No competing financial interests exist.