
Abstract
Introduction:
Pyelovenous/pyelolymphatic backflow from acute ureteral obstruction, manifesting radiologically as perinephric fat stranding (PFS), may result in elevated serum creatinine. Among patients with acutely obstructing ureterolithiasis, we evaluated the relationship between degree of PFS and changes in serum creatinine from baseline.
Methods:
Our tertiary care center's radiology dictation system (Fluency Discovery, M Modal) was queried for noncontrast abdominopelvic CT studies obtained in the Emergency Department for patients with obstructing ureteral calculi from 7/2015 to 4/2016. A single radiologist blinded to clinical data reviewed all CT scans and coded stone size, location, severity of hydronephrosis, and degree of PFS (none, mild, moderate, severe). For patients who met imaging criteria, a retrospective chart review was performed.
Results:
We evaluated 148 patients with mean age of 46 years (SD 14.6), 56.0% (n = 83) were male. On univariate analysis, moderate-severe perinephric stranding was associated with elevated creatinine from baseline (OR 2.93, p = 0.03). Mean creatinine increased as the severity of stranding increased (none Cr = 0.978 mg/dL, mild Cr = 0.983 mg/dL, moderate Cr = 1.165 mg/dL, severe Cr = 1.370 mg/dL; p < 0.01). An increase in creatinine from baseline was not associated with greater severity of hydronephrosis (OR 0.504, p = 0.189). There was no association between degree of PFS and severity of hydronephrosis, positive urine culture, stone location, or symptom duration (p > 0.05). On regression analysis controlling for positive urine culture and degree of hydronephrosis, there remained an association between elevated serum creatinine from baseline and moderate-severe PFS (OR 9.0, p = 0.01).
Conclusions:
Among patients with acute obstructive ureterolithiasis, moderate-severe PFS was associated with elevated serum creatinine from baseline. This elevated creatinine was not explained by the obstructed kidney alone, as there was no association between the severity of hydronephrosis and increased creatinine. Pyelovenous/pyelolymphatic backflow resulting in PFS may be a contributing factor to elevated serum creatinine in this setting.
Introduction
A
When patients present with ureterolithiasis in an acute setting such as the emergency department, serum creatinine is often elevated, thus prompting early stone intervention. While acute ureteral obstruction can lead to an increase in serum creatinine, the possible confounding contribution of pyelovenous and pyelolymphatic backflow to elevated serum creatinine has yet to be established. Furthermore, intervention may have historically been pursued due to the presence of PFS with concern for concomitant pyelonephritis.
We explored the relationship between the severity of PFS and changes in serum creatinine among those presenting with acute ureterolithiasis. Secondarily, we investigated potential associations between PFS and stone location, degree of hydronephrosis, requirement for surgical stone intervention, and the presence of concomitant urinary tract infection.
Methods
After obtaining Institutional Review Board approval, our tertiary care center's radiology dictation system (Fluency Discovery, M Modal) was queried for noncontrast CT abdominopelvic studies obtained in the emergency department for patients older than 18 years with obstructing ureteral calculi from 7/2015 to 4/2016. A single radiologist blinded to clinical data reviewed all CT scans and coded maximal diameter of stone in the axial plane, stone location, severity of hydronephrosis, and degree of PFS.
PFS was considered present only when it was ipsilateral to the acute ureteral stone. The amount of PFS was classified as none, mild, moderate, or severe (Table 1 and Fig. 1). 4 Severity of hydronephrosis was also classified as by the radiologist as none, mild, moderate, or severe.
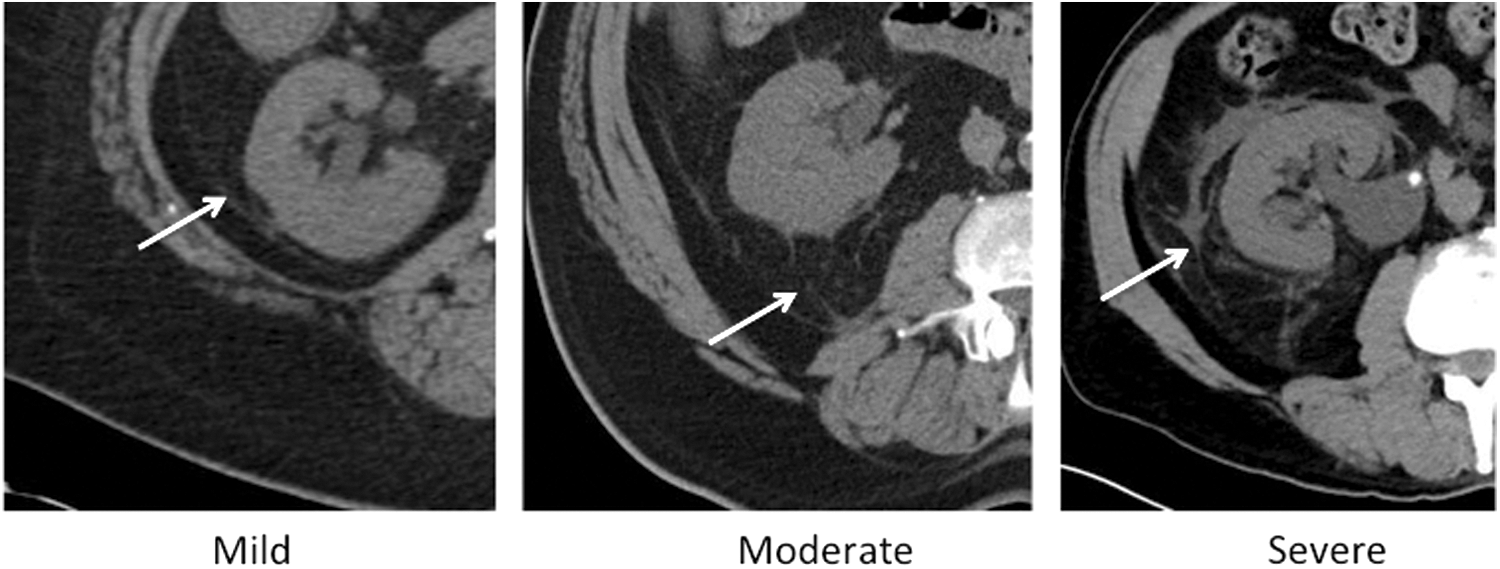
Examples of perinephric fat stranding grades on axial noncontrast CT scan. Arrow denotes perinephric fat stranding.
PFS = perinephric fat stranding.
For patients who met imaging and clinical inclusion criteria, a retrospective chart review was performed. Patients with bilateral ureteral stones, ureteral stents, or percutaneous nephrostomy tubes, and those with nonobstructing renal or bladder calculi were excluded. Clinical data included baseline patient characteristics, urinalysis and urine culture, serum creatinine, requirement for hospital admission, and endoscopic stone management. A urinalysis was considered to be suggestive of infection if there were greater than 5 white blood cells per high-powered field and at least small leukocyte esterase or positive nitrite. Elevated serum creatinine was defined as ≥10% increase from baseline, which accounted for greater variance in creatinine values than could be attributed to degree of laboratory error at our institution.
Data analysis was conducted using PASW Statistics 18 software (SPSS, Inc., Chicago, IL). The degree of PFS was grouped into a dichotomous format according to the clinical similarities of none and mild vs moderate and severe PFS. Continuous variables were reported as mean and standard deviation if they followed a normal distribution, and a two-sample t-test was utilized for statistical analysis. Categorical data were reported as counts and percentages. Binomial variables were compared using the Pearson chi-square univariate analysis. Logistic regression analysis was utilized to evaluate the relationship between various patient variables and the degree of PFS. A p-value of <0.05 was considered statistically significant for all analyses.
Results
We evaluated 148 patients with CT evidence of unilateral ureteral calculi who presented to the emergency department. Mean patient age was 46.0 years (SD 14.6 years) and 56.0% were male (n = 83). Mean creatinine at the time of presentation was 1.06 mg/dL (SD 0.38 mg/dL), which was significantly higher than the baseline creatinine of our study population at 0.85 mg/dL (SD 0.23 mg/dL; p < 0.001). Mean stone size was 4.8 mm (SD 3.0 mm) and 57.4% (n = 85) were located in the distal half of the ureter. The majority of patients had symptoms for less than 1 day, 52.7% (n = 78). Urinalysis was suggestive of infection in 31.1% (n = 46) and among the 79 patients with urine culture data available, 21.5% (n = 17) were positive. Radiologic evidence of hydronephrosis was present in 82.4% (n = 122). Moderate to severe hydronephrosis was present in 16.2% (n = 24), while 30.4% (n = 45) had moderate to severe PFS (Table 2).
Baseline serum creatinine available for n = 100 patients.
Urine culture available for n = 79 patients.
Mean serum white blood cell count was significantly higher for those with moderate to severe PFS (12.20 × 109/L, SD 4.20 × 109/L) compared with those with none to mild PFS (10.09 × 109/L, SD 3.14 × 109/L; p = 0.018). Fevers were present more frequently in patients with moderate to severe PFS compared with those with none to mild PFS (6.7%, n = 3 vs. 1.0%, n = 1; p = 0.049).
Ultimately, 32.4% (n = 48) of patients were admitted to the hospital. Of the 29.7% (n = 44) of patients who required endoscopic stone management, 56.8% (n = 25) had a ureteral stent placed and subsequently underwent staged ureteroscopy, while 43.2% (n = 19) were managed with primary ureteroscopy (Table 2). For patients with evidence of urinary infection, a full course of appropriate antibiotics was administered and a negative urine culture was obtained before ureteroscopy.
Overall, there were no greater odds of operative intervention for patients with moderate to severe PFS compared with those with none to mild stranding (OR 1.71, 95% CI 0.81–3.60; p = 0.157). In a subanalysis, a greater proportion of patients admitted to the hospital with concern for infection had moderate to severe PFS (n = 7, 63.6%) compared with none to mild PFS (n = 4, 36.4%; p = 0.005). Additionally, a greater proportion of patients who underwent operative intervention due to concern for infection had moderate to severe PFS (n = 7, 58.3%) compared with those with none to mild PFS (n = 5, 41.7%; p = 0.042).
On univariate analysis, moderate to severe PFS was associated with elevated serum creatinine from baseline (OR 2.93, 95% CI 1.07–8.04; p = 0.033). Further, mean creatinine at the time of presentation significantly increased as the severity of stranding increased (Table 3). An increase in creatinine from baseline was not associated with greater severity of hydronephrosis (OR 0.50, 95% CI 0.18–1.42; p = 0.189). There was no association between degree of PFS and severity of hydronephrosis, positive urine culture, stone location, or symptom duration (Table 4).
Stone location evaluated as proximal vs distal ureter.
Symptom duration classified as ≤1 day vs >1 day.
On multiple regression analysis controlling for positive urine culture and degree of hydronephrosis, there remained an association between elevated serum creatinine from baseline and moderate to severe PFS (OR 9.0, p = 0.012) (Table 4).
Discussion
Prior studies have evaluated PFS with respect to pyelonephritis or as a sign of acute obstruction due to a ureteral stone. In this study, we describe a previously unexplored association between the severity of PFS and changes in serum creatinine from baseline among patients with acutely obstructing uretererolithiasis.
Renal physiology is altered in the setting of ureteral obstruction. Unilateral ureteral obstruction results in alternations in renal blood flow, creatinine clearance, and the processing of electrolytes. Obstruction leads to increased renal tubule pressure and decreased GFR. While the renal unit can initially compensate with vasodilators, sustained ureteral pressure ultimately results in increased afferent arteriolar resistance, decreased ureteral pressure, and decreased renal blood flow after 24 hours of obstruction. 5,6 The severity of this process depends on the degree and duration of obstruction. Furthermore, urinary concentrating ability decreases as a result of downregulation of vasopressin-mediated aquaporins, downregulation of sodium transporters, diminished urinary acidification, and decreased potassium secretion. 7 –9 Grossly, the collecting system becomes dilated within 42 hours of obstruction with edematous changes to the renal parenchyma after 7 days. 10
PFS can be associated with acute ureteral obstruction and therefore is often identified on CT during workup for ureteral calculi. We stratified PFS according to severity as none, mild, moderate, or severe, based on assessment by a single radiologist according to prespecified definitions. Previous studies have utilized a similar grading scale of severity that is largely based on the degree of linear areas of perirenal soft tissue attenuation. 4,11,12
PFS has value as a secondary sign of acute obstruction from ureteral stones. The positive predictive value of PFS for acute ureteral obstruction has been described as 92%. This is similar to other secondary signs of acute ureteral obstruction including ureteral dilation and collecting system dilation with positive predictive values of 92% and 93% respectively. 3 Similarly, PFS was largely present in our study cohort, as 79.7% of patients had at least mild PFS in the setting of acute ureterolithiasis.
On univariate and multiple regression analysis, we found that patients with moderate to severe PFS had greater odds of elevated creatinine from baseline. Furthermore, mean serum creatinine significantly increased as the severity of PFS increased. Yet, there was no association between the severity of hydronephrosis and elevated creatinine in our study cohort. Therefore, the observed increase in creatinine with more severe PFS may not be explained by acute obstruction of the renal unit alone. Certainly, unilateral ureteral obstruction can lead to increased creatinine, however, this depends on multiple factors including severity of obstruction, duration of obstruction, and overall baseline renal function. Given that our analysis did not identify an association between severity of hydronephrosis and elevated creatinine, this was utilized as an internal control when evaluating the influence of PFS on elevated serum creatinine from baseline.
In the setting of an acutely obstructing ureteral calculus, PFS may result from pyelovenous and pyelolymphatic backflow, thereby leading to an increase in serum creatinine. The severity of PFS may therefore be considered when interpreting the significance of an elevated creatinine. This particularly applies to patients with moderate to severe PFS, in whom abnormally elevated serum creatinine may be secondary to both acute renal unit obstruction in addition to pyelovenous and pyelolymphatic backflow.
Previous studies that have evaluated PFS in relation to the likelihood of stone passage have shown inconsistent results. Parekattil and colleagues developed a model to predict stone passage among patients presenting to the Emergency Department with renal colic. On univariate analysis, more severe PFS was associated with greater odds of spontaneous stone passage within 2 weeks. However, after controlling for stone location, stone size, and severity of hydronephrosis, there was no longer an association between severity of PFS and stone passage. 13 Further, a retrospective analysis by Takahashi and colleagues of 34 patients with CT evidence of a single ureteral calculus showed that PFS was more severe among those experiencing spontaneous stone passage. 4 An additional retrospective study of 51 patients with ureteral calculi by Boulay and colleagues found no difference in successful conservative management vs interventional treatment for patients with mild, moderate, or severe PFS. 11 In our overall evaluation of 148 patients, PFS severity was not associated with progression to surgical stone intervention.
We found no association between PFS and positive urine culture. Fukami and colleagues further explored the relationship between PFS and pyelonephritis. 14 In this case–control study, after adjusting for age, sex, and renal function, PFS had a sensitivity, specificity, and positive likelihood ratio of 72%, 58%, and 1.7% respectively for diagnosing acute pyelonephritis. Therefore, PFS was not useful in the diagnosis of acute pyelonephritis. Additionally, our findings suggest that PFS in the setting of acute ureteral obstruction may not be a reliable marker for infection, as there was no association between PFS severity and positive urine culture.
In a subanalysis, our data did suggest that a greater proportion of patients with moderate to severe PFS underwent operative intervention or were admitted to the hospital specifically due to concern for infection. Despite the absence of an association between urine culture results and severity of PFS, the presence of PFS and the observed leukocytosis in the moderate to severe PFS cohort may raise suspicion for infection at the time of initial presentation leading to operative intervention or admission to the hospital. It is important to acknowledge that our findings are limited by small sample sizes for the subpopulation of patients being admitted or undergoing operative intervention with concern for infection. This is particularly so for patients presenting with fevers (none to mild PFS n = 1, moderate to severe PFS n = 3).
While we provide insight into the relationship between PFS and serum creatinine, our study is limited by the experience of a single institution and the retrospective design. Furthermore, we were unable to quantitatively evaluate other factors that may influence serum creatinine such as dehydration from nausea and emesis that may further limit the ability to tolerate oral hydration and quantity of nonsteroidal anti-inflammatory use for pain before presentation to the emergency department. When patients presented to the emergency department, multiple interventions were often initiated including intravenous hydration, nonsteroidal anti-inflammatory medication, and even ureteral stent placement. Therefore, identification of particular interventions and their effect on subsequent creatinine values in an effort to identify the etiology of elevated creatinine is beyond the ecological data available in this retrospective analysis. However, we did compare baseline serum creatinine and creatinine at the time of presentation with acute ureterolithiasis in an effort to establish an internal control. It is plausible that infected urine may be upstream of a completely obstructing ureteral stone with the possibility of a false negative urinalysis or urine culture. However, this study was intended to assess the clinical picture as it is available to the urologist when evaluating a patient with an acute ureteral stone in the emergency department setting. Finally, our study design allowed for evaluation of factors associated with PFS based on hypothesized mechanisms rather than determining causality.
Conclusions
Moderate to severe PFS in the setting of acute obstructive ureterolithiasis is associated with an elevation in serum creatinine from baseline. Therefore, the hypothesized mechanism of pyelovenous and pyelolymphatic backflow that results in PFS may be a contributing factor when interpreting elevated serum creatinine in this setting.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest or disclosures related to this article.