
Abstract
Objectives:
Urine cultures before secondary ureterorenoscopy (URS) are recommended to exclude bacteriuria, but results are often pending on the day of surgery. We sought to develop predictive models that reliably indicate the absence of bacteriuria in patients with indwelling ureteral stents based on readily available data.
Patients and Methods:
Records of patients undergoing secondary URS between 2014 and 2017 were assessed retrospectively. Patient characteristics, automated urinary sediment analysis, blood analyses, and results of urine cultures were analyzed using descriptive statistics, receiver operating characteristic curves, logistic regression, and model selection.
Results:
Of 462 patients, 101 (21.9%) had positive urine cultures. Urinary leucocytes, nitrite and pH, patient age and sex, and blood C-reactive protein (CRP) levels were associated with bacteriuria in logistic regression (p < 0.05), but did not sharply separate patients with and without bacteriuria. A multiple logistic regression model considering all six parameters and their interactions indicated a low probability of bacteriuria (8%) for 74% of the patients. Alternatively, recursive partitioning indicated low probability of bacteriuria (8%) if four criteria are simultaneously fulfilled (54% of the patients): Male, negative nitrite, urine leucocytes ≤1174/μL, and blood CRP ≤13 mg/L.
Conclusions:
Bacteriuria in patients with indwelling ureteral stents before URS can hardly be predicted based on single clinical or laboratory parameters. Although the combination of relevant predictors allows for exclusion of urinary tract infection with relatively high confidence in most patients, the residual diagnostic uncertainty calls for optimized organizational measures to assure availability of urine cultures before surgery.
Introduction
U
On the contrary, ureteral stents are also known to be predisposing for bacterial growth, colonization, and bacteriuria. 7,8 Therefore, EAU and AUA guidelines recommend preoperative urine cultivation and guided antibiotic treatment in patients undergoing secondary URS to prevent serious complications such as bacteremia and urosepsis. 1,9 Urine cultures, including antibiograms, represent the most reliable method to detect bacteriuria and the only way to guide targeted antibiotic treatment. As results of cultivation and susceptibility tests are available only after several days, patients are usually instructed to undergo urine analysis and culture before hospitalization for secondary URS.
Nevertheless, results of urine cultures are often pending on the day of surgery in clinical routine. This raises the question of postponement of the operation, which is in turn associated with organizational efforts and increased costs. Rapid tests for bacteriuria could help guide decisions in this situation; however, they have been widely abandoned in hospitals due to their clear limitations. Automated bacterial counting and direct microscopy are unreliable due to a low sensitivity and specificity and cannot discriminate bacterial contamination, colonization, and infection. 10 –12 Dipstick leukocyte esterase and nitrite tests are of limited use as leucocyturia is a normal finding in patients with ureteral stents and nitrite lacks sensitivity for the detection of infections not caused by Enterobacterales (formerly Enterobacteriaceae). 13 –15
Therefore, the quantity of leucocyturia and serum blood inflammatory markers are often used in clinical practice to guide decision-making, whether secondary URS can be safely performed or should be postponed until results of urine culture are available. To the best of our knowledge, these parameters have never been analyzed systematically so far.
In this study, we sought to identify instantly available parameters that allow for prediction or exclusion of bacteriuria in patients with indwelling ureteral stents and to assess to what extent predictive values can be improved by combining these parameters.
Patients and Methods
Study population
The study was approved by the local Ethics Committee (EKOS 2016-02181). Records of patients who underwent secondary URS for urolithiasis at our department between January 2014 and October 2017 and provided written informed general consent for data analysis were retrospectively analyzed. Only patients with available urine cultures and without proof of antibacterial activity in urine were included.
Assessed patient characteristics included age, sex, ASA (American Society of Anesthesiologists) score, diabetes mellitus, immune deficiency, and duration of ureteral stenting before secondary URS.
Laboratory examinations
In men, midstream urine samples were collected after cleansing with saline. In women, intermittent bladder catheterization was performed after topical disinfection with povidone iodine (Betadine®) solution or 0.1% octenidine solution (Octenisept®). Sample collection was repeated if epithelial cells in automated urinary sediment analyses exceeded 20/μL.
Laboratory assessment was routinely performed 1 day before secondary URS and included blood analyses (leucocytes [Lc; normal range 4–10 G/L], C-reactive protein [CRP; normal range <8 mg/L]), automated urinary sediment analyses (Lc [normal range <20/μL], pH, nitrite), and urine cultures.
For automated sediment analysis, a Cobas u601 (Sysmex, Horgen, Switzerland) was used, and microscopic analysis was performed with KOVA counting chambers (Axonlab, Baden, Switzerland). Urine was cultivated following established protocols. By standard, 0.001 mL of urine was used to inoculate a Columbia agar (“sheep blood” agar) and a BD BBL™ CHROMagar™ Orientation agar (Becton Dickinson, Franklin Lake, NJ). Analytical sensitivity was therefore 1000 cfu/mL. After streaking, media were transferred to incubators with 36°C aerobic (Orientation agar) or CO2 enriched (Columbia agar) atmosphere. To provide a timely result, media were inspected for growth after 18 to 20 hours of incubation. If Columbia agar was negative (i.e., no growth), incubation was prolonged by 1 day to ensure detection of slow growing organisms. Based on the bacterial growth on Columbia agar, semiquantification of growth extrapolated to 1 mL was done (e.g., 1000, 104, 105 and >106 cfu/mL). Identification was done with MALDI-ToF using the latest version of spectrum database (Bruker Daltoniks, Bremen, Germany). Monomicrobial growth or growth of two uropathogenic bacteria in relevant numbers (i.e., at least 104 cfu/mL) was rated as clinically significant. Growth of typical commensal species or growth of more than two species was reported as “urethral flora” or “mixed flora” according to the European guidelines for urinalysis and not defined as UTI. 16
Statistical analyses
For descriptive analyses, continuous variables are summarized as medians and interquartile ranges (lower and upper quartiles) and categorical variables as the count and percent. Relationships between 11 potential predictors and presence of bacteriuria were analyzed using simple and multiple logistic regression. The sample size of our study (462 patients, 101 with bacteriuria) was adjusted to this number of predictors. Urine and blood leucocytes as well as blood CRP were analyzed log-transformed because of strongly skewed distributions. Besides fitting a model with all predictors, best model selection was performed by comparing the Akaike information criterion (AIC) of models with all possible combinations of 0 to 11 predictors (either including or excluding each of them in turn) to determine the model with the lowest AIC. This model was subsequently expanded by including two-way interaction terms for all pairs of predictors, followed by backward selection of the most significant interactions (p < 0.05) based on type-II likelihood-ratio tests; a more conservative selection criterion was applied here to limit the number of interaction terms included. The predictive values of the best simple and multiple logistic models were evaluated with receiver operating characteristic (ROC) curve statistics.
As an alternative approach that might be simpler to implement in clinical practice, data were also analyzed with recursive partitioning, a flexible, nonparametric method that subdivides the data set into several subsets with distinct probabilities of bacteriuria presence based on simple dichotomic classification rules.
All statistical analyses were performed in the R programming language (version 3.2.3), using the function ctree in R package party for recursive partitioning.
Results
Patient characteristics and laboratory findings
A total of 462 patients could be included in the analysis, of whom 101 (21.9%) showed significant bacteriuria as defined above. Patient characteristics and laboratory findings are reported in Table 1. Typical UTI pathogens were found in the majority of positive urine cultures with Escherichia coli (22.6%), enterococci (21.4%), Klebsiella sp. (9%), Pseudomonas aeruginosa (6.0%), and Candida sp. (10.7%) representing the most frequent species. Antibiotic resistance rate was highest for ampicillin (42%), while rates for antibiotics used frequently for intraoperative prophylaxis in endourology were 37.5% for cotrimoxazole, 24.2% for ciprofloxacin, and 23.5% for cefuroxime.
p-Values from Wilcoxon rank sum tests comparing the two patient groups are reported for numeric parameters (upper part of the table); p-values from chi-squared tests for association between each parameter and bacteriuria are reported for categorical parameters (lower part of the table); percentages refer to the total number of evaluable patients without or with bacteriuria.
Numbers of patients with available data slightly differed for individual parameters; the range is given.
ASA = American Society of Anesthesiologists; CRP = C-reactive protein; IQR = interquartile ranges; Lc = leucocytes.
Regression on single predictors
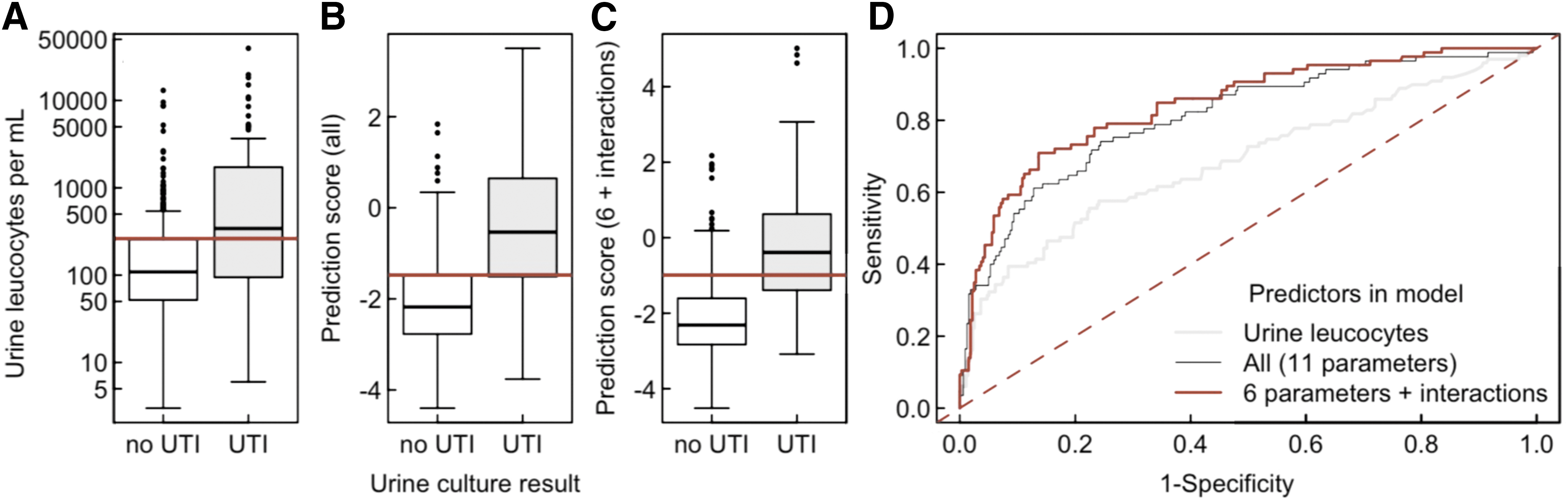
Eight predictors (i.e., urinary Lc, nitrite and pH, patient age, sex, ASA score, blood Lc, and CRP levels) were found to be significantly associated with bacteriuria in simple logistic regression analyses (Table 2). However, according to ROC statistics, even the most significant predictor (urinary Lc) did not allow a sharp separation of patients with and without bacteriuria, as supported by an area under the curve (AUC) of 0.688 (Table 3) and a poorly defined optimal cut point of 262 Lc/μL (Fig. 1). Bacteriuria could be excluded with an 87% probability using this cut point, but only 68% of the patients had an Lc-count below this threshold. For the remaining 32% of patients, presence of bacteriuria would be predicted, but actually occurred only with 40% probability (Table 3).
Distribution of predictor values among patients without and with bacteriuria
Separate regression models were independently fitted for each parameter.
Based on a model including all parameters, the effect deviance for each parameter was calculated as the increase in residual deviance when removing this parameter from the model (type-II tests). The effect deviance is smaller than in univariable models if parameters are correlated, so that their contribution to the prediction of bacteriuria is partly redundant.
Odds ratios refer to a one-unit increase of numeric parameters to a 10-fold increase of log10-transformed parameters and to the comparison of categories as indicated for categorical parameters.
p-Values were derived from the asymptotic chi-squared distribution of the effect deviance.
Provided for the two most significant predictors of bacteriuria in univariable models, a model including all parameters assessed, and the selected best model including six predictors and the significant two-way interactions.
Not available for a categorical predictor.
The optimal cut point is the value maximizing sensitivity+specificity, except for urine nitrite, for which it was set as presence or absence of nitrite.
The cut point refers to the probability of presence of bacteriuria as predicted by the model.
AUC = area under the curve.
Regression on multiple predictors
In a multiple logistic regression model, including all potential predictors but no interactions, six of the eight predictors identified by univariate analyses remained statistically significant (Table 2). The same six parameters were included in the model with smallest AIC identified by model selection. If two-way interactions were added to this model, those between urine Lc, blood CRP, and gender were clearly significant, indicating that the predictive value of these three parameters is interdependent. For example, blood CRP has a different impact on the prediction in males and females.
Thus, the best model to predict bacteriuria would include six parameters and three interactions (Fig. 1 and Table 3). A simple instruction allowing for creation of an Excel®-based (Microsoft Corp., Redmond) bacteriuria risk calculation tool for patients with ureteral stents based on this model is provided in Figure 2.
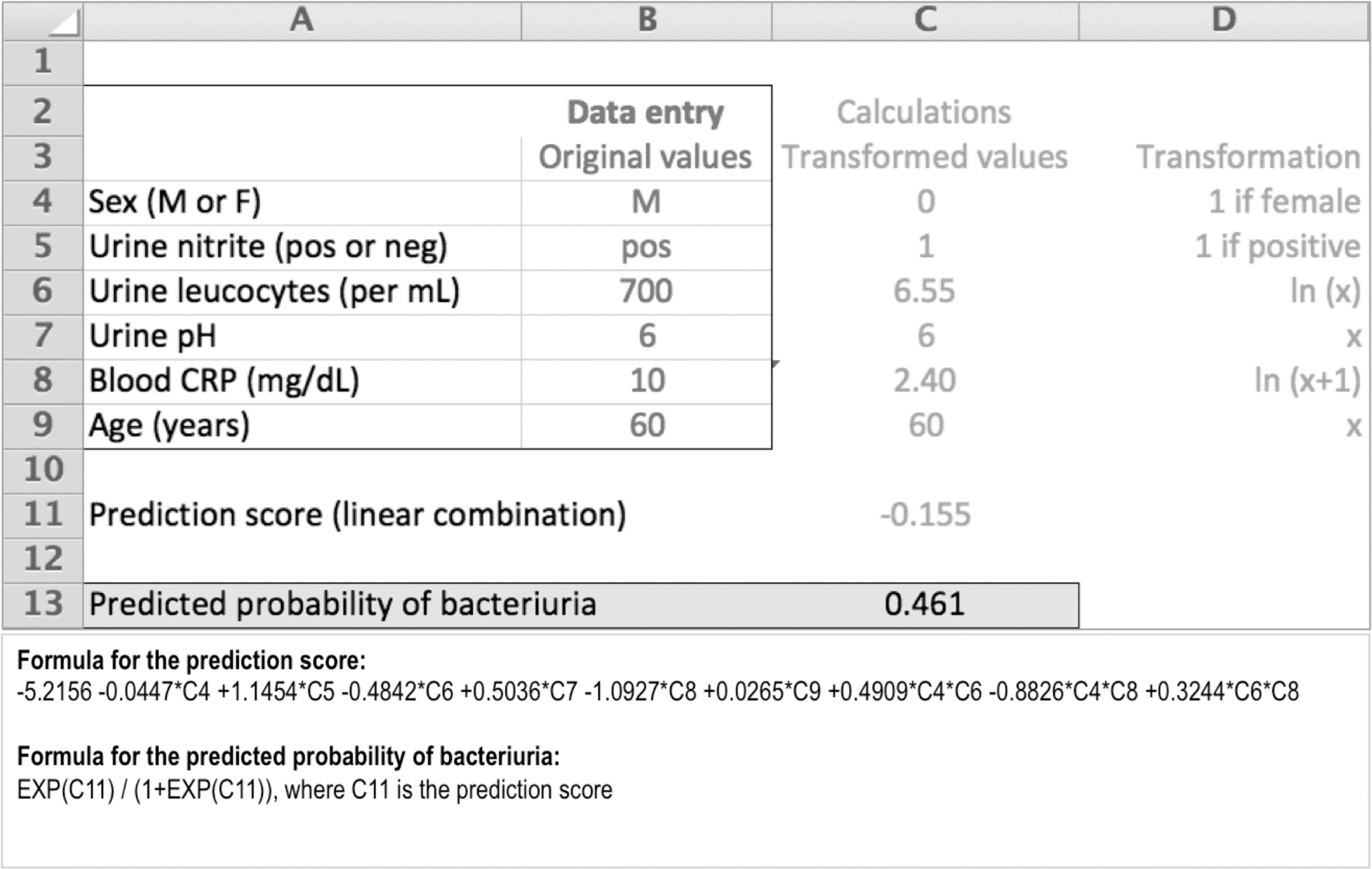
Bacteriuria risk calculation tool for patients with ureteral stents based on a model with six predictors and three interactions. (File can be prepared in Excel® using the provided formulas or obtained from the corresponding author.)
Recursive partitioning
Recursive partitioning showed that the combination of urine nitrite and Lc, gender and blood CRP can be used to easily group patients into three categories (Fig. 3) with a probability of bacteriuria of 8% (low), 27% (intermediate), and 60% (high) respectively. Therefore, using these categories, predictive values similar (i.e., negative predictive value [NPV] 92% and positive predictive value [PPV] 60%) to those of the model with six parameters, and three interactions can be achieved if no prognosis is made for patients in the intermediate category. However, the latter represented 27.4% of the study population. Rating an intermediate probability as either predicted absence or predicted presence of bacteriuria would reduce NPV to 85.6% and PPV to 39.3%, respectively.
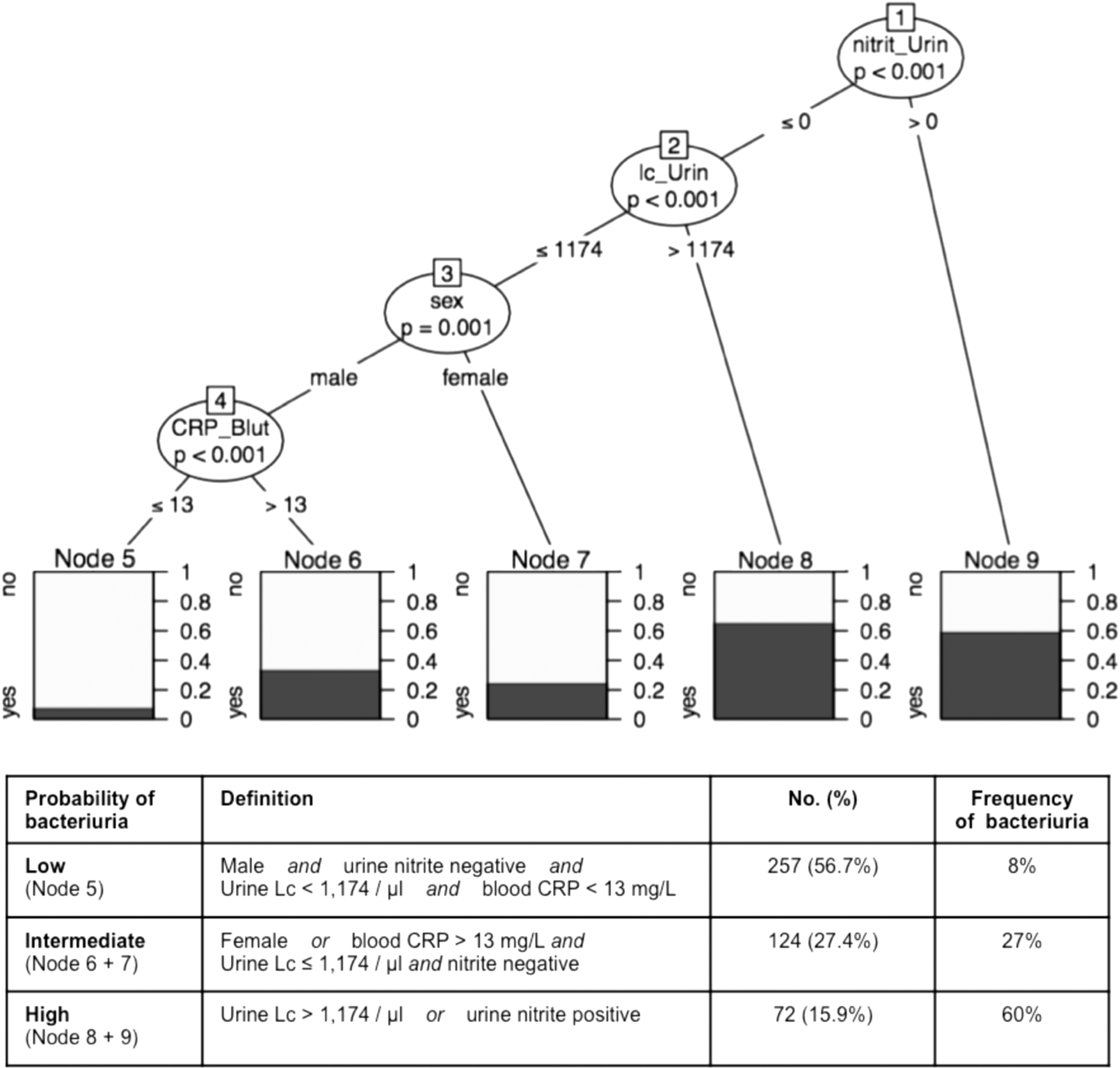
Partitioning tree for the presence or absence of bacteriuria. (The tree illustrates how the data set was split at specific cut points of the predictors. Resulting data subsets represent groups of patients with distinct bacteriuria probabilities. p-Values at each split indicate the significance of the relationship between the predictor and presence of bacteriuria among the patients considered at this split. Splitting criteria are indicated on the branches.)
Discussion
Rapid test methods for bacteriuria suffer from clear limitations and have been abandoned widely in clinical practice, in particular to reduce unnecessary antibiotic treatments. As results of urine cultures are sometimes pending at the day of surgery, we assessed rapidly available clinical and laboratory parameters that might allow for an early prediction of bacteriuria in patients with indwelling ureteral stents undergoing secondary URS and tried to maximize predictive values by combining the most suitable predictors.
Different parameters were found to significantly correlate with the presence or absence of bacteriuria. In general, PPV were rather low for stand-alone parameters with urine nitrite representing the most accurate one (PPV 56%, but only for 11% of patients and associated with low NPV) and could be hardly improved using complex models (PPV 58% for model with six parameters and three interactions, 60% for recursive partitioning) (Table 3).
In contrast, relatively high NPVs were found. Thus, bacteriuria could be excluded with an 87% probability solely by urine Lc below a cut point of 262/μL. However, Lc counts below this threshold were only found in 68% of patients. The NPV could be improved to 92% by using a model including all of the assessed parameters, but for even fewer patients (65%).
As a similar quality of prediction could be achieved for more patients by reducing this model to six parameters and three interactions (Table 3), we provide a simple instruction allowing for creation of an Excel-based (Microsoft Corp.) bacteriuria risk calculation tool for patients with ureteral stents based on this model (Fig. 2). This calculation tool can be used to estimate the risk of bacteriuria in patients with indwelling ureteral stents at a minimum effort and was able to exclude bacteriuria with a 92% probability in 74% of the included patients.
In addition, we used recursive partitioning to define parameters and cut points that can be easily applied in clinical routine (Fig. 3). This approach allows for instant categorization of patients into three groups with substantially diverging probabilities for bacteriuria based on the presence or absence of four risk factors.
Similar to the statistical model described above, these probability categories are not supposed to avoid routine performance of urine cultures, but might allow a better estimation of the present risk of bacteriuria in an individual patient and, therefore, support decision-making in cases where urine cultures are pending at the day of surgery.
Considering concomitant relevant factors such as the patient's general condition and stone burden and location, selected patients with a low risk of bacteriuria as predicted by the developed model or probability categories might be considered for surgery despite pending urine cultures, whereas surgery should be definitely postponed in patients assigned to the intermediate and high probability group.
However, infectious complications caused by URS occur frequently (e.g., postoperative urosepsis in up to 7.4%) and patients with a positive preoperative urine culture have been shown to be at a significantly higher risk of developing postoperative urosepsis. 17 Considering the potential degree of severity of such complications and the residual diagnostic uncertainty of all prediction parameters and models, our data clearly outlines that prediction of bacteriuria based on clinical or laboratory parameters in patients with indwelling ureteral stents before URS should not substitute for urine cultures.
Our study has limitations that have to be addressed. Data were assessed retrospectively coming along with the limitations of such trials. Although ureteral stents are frequently causing symptoms similar to those triggered by UTI, such symptoms might represent another predictor of positive urine cultures. As presence or absence of these symptoms had not been documented systematically, it was not possible to include them into our analysis. Inclusion of automated bacterial counting and direct microscopy, which have been shown to have a low sensitivity and specificity if used exclusively 10 –12 into the analyses, might have the potential to improve prediction of bacteriuria. However, as such methods are not performed routinely at our institution for reasons outlined above, these data were not available. In addition, bacterial colonization of ureteral stents was not assessed in our patients and therefore the analyzed predictors are not transferable to results of stent cultures, which can differ significantly from those of urine cultures as shown elsewhere. 18 The study was performed at a single institution, and external validation would improve its reliability.
Conclusions
Bacteriuria in patients with indwelling ureteral stents before URS can hardly be predicted based on single clinical or laboratory parameters. Combination of relevant predictors allows for exclusion of UTI with relatively high confidence in most patients. Nevertheless, the residual diagnostic uncertainty calls for optimized organizational measures to assure availability of urine cultures before surgery.
Footnotes
Author Disclosure Statement
No competing financial interests exist.