
Abstract
Purpose:
To present the positive impact of technique standardization on successful outcome, fluoroscopy, and total operating time (TOT) shortening in a prospective study.
Methods:
Six experienced endourologists participated. To assess whether the adaptation of standardized surgical steps improved their methodology with time, 253 patients were prospectively divided in three consecutive 1-month groups. Patients underwent stent placement and exchange and total operating and fluoroscopy times (FTs) were recorded. All surgeons were unaware of their mean recorded results until the end of the study. At the end of the third month, we evaluated if the suggested technique standardization established a decrease for both FT and TOT. Statistical significance was set to p < 0.05.
Results:
Total operating and FTs were significantly reduced with time between all groups of patients. For stent placement, TOT showed significant reduction between Groups A and C (p < 0.001), while between other group comparisons did not reach significance. FT showed a significant reduction (p < 0.001) in all group comparisons. For stent exchange, TOT reached significant improvement (p = 0.003) between Groups A and C, whereas between other groups was insignificant. FT improvement was significant between Groups A and C (p < 0.001) and Groups B and C (p < 0.001), but insignificant between Groups A and B.
Conclusions:
Even in experienced hands, the adaptation of technique standardization results in significant decrease of total operating and FTs and it is independent from feedback regarding their time performance.
Introduction
A
Regarding medical fluoroscopy, there has been new insight in deleterious effects of radiation exposure that prompted medical professionals to reevaluate their current practice regarding radiation to their patients and themselves. 4 Herein, we present our prospectively collected results of a large multicenter cohort of patients with indwelling stents that were inserted or exchanged with standard surgical steps. Furthermore, we assess the impact of this standardization on successful outcome, fluoroscopy, and operating time.
Materials and Methods
After Institutional Review Board approval (IRB No: EE-2/39/6-6-2017) and written informed consent were obtained, 253 patients, 133 men and 120 women, aged 17 to 84 years (mean 47.7 years), with unilateral Double-J ureteral stents, were prospectively evaluated and treated by six experienced endourologists.
The indications for stent placement were pelvicalyceal and/or ureteral dilatation due to ureteral stones <10 mm planned for extracorporeal shockwave lithotripsy (SWL) (159 patients) and hydronephrosis of any other reason (94 patients). Evaluated operations were USP (194 patients) and ureteral stent exchange (USE) (59 patients). Combined procedures (e.g., antegrade and retrograde stent placement) were excluded. All procedures were performed by experienced endourologists, with at least fellowship in endourology, while fluoroscopy was performed by certified technicians.
Given that each surgeon has his own methodology in performing endourological procedures, all participating surgeons agreed to follow a frame of specific surgical exact steps (Table 1). Fluoroscopy time (FT) and total operating time (TOT) were recorded in seconds for every procedure and all assessed data were immediately recorded by an assistant. TOT was defined from the first maneuver of the surgeon (e.g., insertion of the cystoscope) until the last maneuver (e.g., catheter placement or cystoscope removal). In cases of bilateral procedures, each intervention per side was assessed separately.
USP = ureteral stent placement.
All patients with lithiasis preferred the option of initial management with stent placement combined with SWL (“spontaneous passage trial” for all stone fragments). 5 The inclusion and exclusion criteria are listed in Table 2.
The cohort of patients was prospectively divided in three 1-month consecutive groups: Group A consisted of the first 85 consecutive patients, Group B of the following 86 patients, and Group C of the remainder 82 consecutive patients, respectively. In Group A, 44 men and 41 women, aged 17 to 81 years (mean 46.5 years) were enrolled. Fifty nine patients underwent SWL, while 64 patients underwent USP and 21 USE. Group B consisted of 45 men and 41 women, aged 19 to 84 years (mean 49.2 years), where 55 patients underwent SWL, 66 patients underwent USP and 20 USE, respectively. Group C consisted of 42 men and 40 women, aged 17 to 81 years (mean 47.6 years), where 50 patients underwent SWL, 64 patients underwent USP and 18 USE, respectively (Table 3).
Bold type indicates statistically significant values.
SD = standard deviation; SWL = extracorporeal shockwave lithotripsy; USE = ureteral stent exchange.
All endourologists participated in all groups. Moreover, in cases of patients with repeat procedures in different groups, all procedures were performed by the same surgeon. All procedures were performed under conscious sedation and on outpatient basis, unless the patient was already hospitalized for any other reason.
Although there are no data available, we hypothesized that 1 month would be a sufficient period of time for an experienced endourologist to adopt the specific surgical exact steps and further improve his methodology. All surgeons were unaware of their mean recorded results until the end of the study. At the end of the third month, we were able to evaluate whether the aforementioned “automation” in methodology was an advantage to establish a decrease for both FT and TOT, without the risk of bias since the surgeons had no feedback of their performance. With the certain sequence of steps, needless and time-consuming maneuvers can be avoided, leading to FT and TOT improvement. Data from all three groups were compared and changes in successful outcomes, FT and TOT were analyzed.
Our standardized surgical key-steps are detailed in Table 1. We avoided continuous imaging during the advancement of the wire and we reserved fluoroscopy only for cases where resistance was encountered and/or to check the correct position of the wire, like management strategy of guidewire placement in pregnant women. 6 We typically employed hydrophilic-coated nitinol wires, which allow ease of passage and usually do not injure the ureter as the nonhydrophilic wires could do, suggesting a less traumatic tip. 7
We usually use stents of 6F diameter, since there are considered superior to other sizes in terms of stent migration and stent related symptoms (SRS). 8,9 Regarding proper stent length, which we consider as an important parameter, we preoperatively choose the proper stent length by using the body habitus of each patient. 10 We avoid additional procedures and radiation exposure intraoperatively, while by choosing the proper stent length we cause less discomfort to our patients since longer stents cause SRS, especially if they cross the urinary bladder's midline. 11
Fluoroscopy
Fluoroscopy was performed by certified technicians only. All persons within the operating room were using lead aprons, thyroid collars, and lead glasses and every staff member exposed to ionizing was provided with radiation badges. The badges were checked in a weekly basis to inform the surgeon in case of excessive exposure since none of the participants was aware of the FT. All C-ARM units were equipped with audible signals generated during pedal depression.
Statistical analysis
The analysis of variance was used to determine statistical significance when the distribution was normal. Post hoc comparisons used the Bonferroni method. When the distribution was not normal and when standard deviations differed significantly, the nonparametric Mann–Whitney test was used. Normality was tested by using the Kolmogorov–Smirinov technique. Nominal data were compared using the Chi-Square test. All calculations were carried out by using the SPSS 17.0 for Windows. Statistical significance was set to p < 0.05. Data were expressed as mean ± standard deviation.
Results
There was no significant difference between the three groups regarding age (p = 0.532), sex (p = 0.75), side (p = 0.96), etiology (SWL, other) (p = 0.73), procedure (USP or USE) (p = 0.88), or success rate (p = 0.81). Mean FT in the whole cohort was 47 seconds, while mean TOT was 870 seconds. JJ stents were placed on the right side in 134 patients and on the left in 119. Furthermore, 159 patients underwent stent placement due to SWL and 94 patients underwent stent placement due to any other reason, while USP was performed in 194 and USE in 59 cases, respectively. All cases of USP and USE have been successfully performed. None of the personnel had to suspend practice due to radiation overexposure.
Mean TOT in the whole cohort was 870 seconds and was significantly different between Groups A and B (p = 0.001), between Groups B and C (p = 0.028) and between Groups A and C (p < 0.001), respectively. The mean TOT was 1068, 846, and 690 seconds in Group A, B, and C, respectively. The FT was significantly different (p < 0.001) in all group comparisons (Group A vs Group B, Group B vs Group C, and Group A vs Group C). The mean FT was 64, 47, and 29 seconds in Group A, B, and C, respectively. In simple words, in the whole cohort of patients, we noticed a progressively decreasing TOT and FT with time, suggesting that standarization of certain surgical steps led to TOT and FT decrease.
Regarding USP, the TOT showed significant reduction between Groups A and C (p < 0.001), while between Groups A and B and between B and C there was a nonsignificant reduction in TOT. Regarding FT, there was a significant improvement (p < 0.001) in all group comparisons (Group A vs Group B, Group B vs Group C, and Group A vs Group C).
Regarding USE, the TOT reached significant improvement (p = 0.003) between Groups A and C, whereas between all other groups the improvement was nonsignificant. The FT improvement was significant between Groups A and C (p < 0.001) and Groups B and C (p < 0.001), but nonsignificant between Groups A and B (Table 3, Fig. 1). Practically, for both simple endourological procedures, a significant improvement with time was proven, when all endourologists of our study got familiar with and adopted certain suggested methodology.
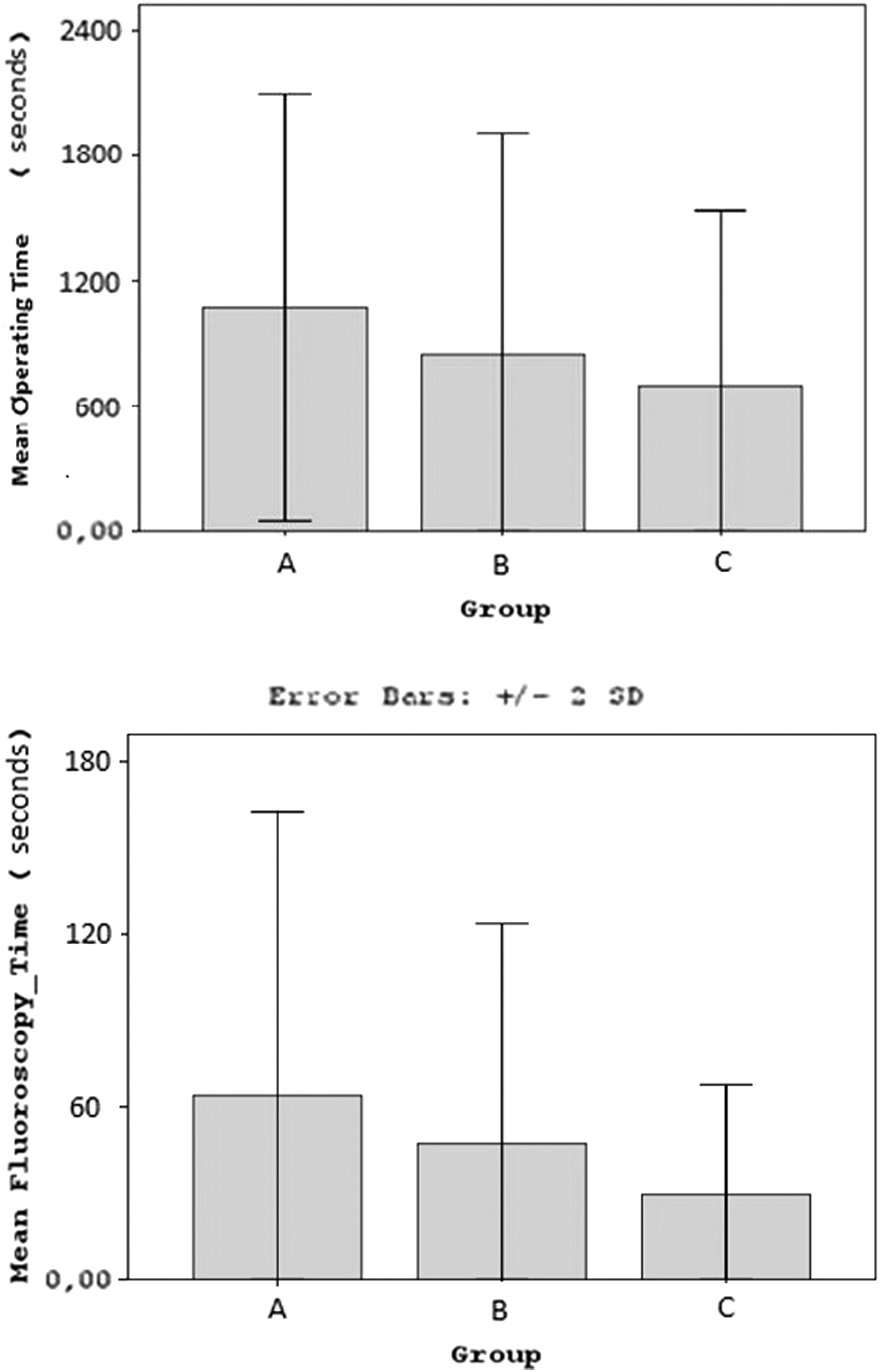
Total operating time and fluoroscopy time improvement in Groups A, B, and C.
Discussion
This study is the first in the literature to evaluate the effectiveness of standardized surgical steps on TOT and FT in the widely performed procedures of USP and USE that can be done even in an outpatient's basis. The original idea was based on the study of Veneziano et al. that described a reliable and replicable methodology toward standardized simulation training in endourology that can be followed to further develop training/assessment protocols for several surgical procedures. 12
The amount of radiation that the patient is exposed to during fluoroscopy is dependent upon FT, distance between the patient and the X-ray source, and the functional parameters of the fluoroscopy machine (kVp, mA). 13 Apart from the patient, urologists, technicians, and nurses are also exposed to radiation primarily from patient scatter. 14 Effective shielding with lead aprons and thyroid collars should be mandatory for all personnel. Although most urologists wear a lead apron (97%) the usage of thyroid shields and lead glasses is less (68% and 17.2%, respectively). 15 The fluoroscopy dose and time should comply with the “as low as reasonably achievable” (ALARA) principal. 16 This is feasible by decreasing the usage time, maximizing the distance from the source, providing adequate shielding, and with technical adjustments. 17 Recording of the FT is relatively easy and definitely reflects radiation exposure for the surgeon, paramedics, and patient.
In our study, participating endourologists were strictly adherent to the ALARA principle and absolute use of effective shielding, thus highlighting the importance of compliance with protective equipment as having an effect on radiation exposure. This particular practice combined with the progressive adoption of the suggested exact surgical steps led to a significant decrease to FT and radiation exposure. Despite protective measures taken worldwide, although with a relatively low rate of compliance, 15 the frequency of fluoroscopy usage plays a major role in the exposure rates of many practicing urologists, since fluoroscopy is becoming utilized by urologists at a continuously increasing rate. 18 This rise in use, along with the high proportion of working time spent within three feet-distance from patients and X-ray source 19 has caused practicing urologists to experience increasing radiation exposure. Taking the aforementioned into account, our results are of utmost importance, additionally because none of the participating endourologists had any feedback regarding FT.
In a recent study where surgeons were provided with feedback of their fluoroscopy utilization, a 24% reduction was found in FT (p = 0.002) despite unchanged TOT. 20 Ritter et al. 21 demonstrated that experienced surgeons reduced their median FT up to 55% after being informed about their fluoroscopy manners, while they significantly reduced both TOT and FT for USP and USE. Interestingly, in the same study inexperienced surgeons were not able to reduce both TOT and FT significantly. 21
FT improvement can be achieved by cumulative experience, even in residents, in relatively more difficult procedures. 22 Even in already experienced hands, the standardization of surgical technique seems the key-point to further significantly improve TOT and FT, which was obvious for all three groups of patients and it was irrelevant of feedback regarding the performance. The fact that the surgeons did not know their FT and TOT excluded the risk of bias in their practice to be quicker. Furthermore, it should be stressed that the mean TOT and FT values of our study were slightly smaller and concerned more patients in comparison with the ones of the recent study of Ritter et al., 21 thus amplifying statistical significance.
Nevertheless, our study has several drawbacks. We evaluated relatively easy endourological procedures. However, even in such cases expected to be simple and not time consuming, a great variety of difficulty exists resulting in a wide range in TOT and FT. 21 Furthermore, the participants did not know their TOT and FT and given that, although experienced, they could perform fluoroscopy more frequently. In our study the fact that surgeons did not know their performance excluded the risk of bias in our evaluation. Also, since our study was multi-center, all procedures were not performed by the same surgeon, resulting in a variability of maneuvers, although the surgical steps were standardized. Lastly, we evaluated only FT to estimate radiation exposure.
However, the reduction of FT is not the only parameter to reduce the effects of ionizing radiation (e.g., chosen functional parameters of C-ARM, collimation, distances from the X-ray source, protection systems (including gloves), use of ultrasonography, use of magnet stents, etc.).
Conclusions
Standardization of the surgical technique of USP and USE results in significant improvement of TOT and FT, which was found to be independent from the feedback regarding these parameters.
Footnotes
Author Disclosure Statement
No competing financial interests exist.