
Abstract
Introduction:
Urinary stone disease (USD) has known associations with the gut microbiota. Approximately 80% of kidney stones contain oxalate as a primary constituent and diverse oxalate-degrading bacteria exist within the human gut, which may protect against USD. Although bacteriotherapy represents a promising strategy to eliminate oxalate and reduce the risk of USD, oxalate-degrading probiotics have had limited success. To identify limitations of oxalate-degrading probiotics and refine development of bacteriotherapies to prevent USD, we review the literature associated with the gut microbiota and USD.
Materials and Methods:
A literature search was performed to identify publications that examine the role of oxalate-degrading bacteria or the whole gut microbiota in oxalate metabolism and the pathophysiology of USD. We conducted a meta-analysis of studies that examined the association of the whole gut microbiota with USD. In addition, we evaluated the gut microbiota of healthy individuals and those with comorbidities related to USD using publically available data from the American Gut Project (AGP).
Results:
Studies on Oxalobacter formigenes reveal that colonization by this species is not a good predictor of USD risk or urinary oxalate excretion. The species of oxalate-degrading bacteria used in probiotics and duration of administration do not impact efficacy or persistence. Studies focused on the whole gut microbiota reveal broad shifts in the gut microbiota associated with USD and a diverse microbial network is associated with oxalate metabolism. AGP data analysis demonstrated a strong overlap in microbial genera depleted in diseased individuals among USD and comorbidities.
Conclusions:
The associations between the gut microbiota and USD extend beyond individual functional microbial species. Common shifts in the gut microbiota may facilitate the onset of USD and/or comorbidities. The successful development of bacteriotherapies to inhibit USD will need to incorporate strategies that target a broad diversity of bacteria rather than focus on a few specialist species.
Introduction
U
Oxalate, the predominant compound in 70%–80% of kidney stones, 4,5 plays a key role in the stone formation. The urine of stone formers is more supersaturated with calcium oxalate than healthy subjects, 6 and oxalate concentrations 25 times higher in the papilla of stone formers than in the urine have been reported, contributing to the formation of calcium deposits. 7 Hyperoxaluria, typically defined as urinary oxalate excretion values that exceed 40 mg per day, is considered a significant risk factor for USD. 8,9 Oxalobacter formigenes, an oxalate-degrading specialist of the human gut, 10 has been negatively associated with USD. 10 –13 This species uses oxalate as its sole energy source and thrives in the presence of the oxalate anion. 14 Although other oxalate-degrading species have also been isolated, 15,16 many exhibit growth inhibition in the presence of oxalate, making the importance of these species for oxalate metabolism in humans unclear.
One hypothesis for the role of the microbiome in the inhibition of USD has been that specific functional bacteria, such as the oxalate-degrading specialist O. formigenes, degrade considerable amounts of dietary and endogenous oxalate, which helps to prevent calcium oxalate crystallization in the kidneys. 17 However, although probiotics based on O. formigenes or a mixture of other oxalate-degrading bacteria reduce urinary oxalate levels, the bacteria and their function are often lost soon after administration of probiotics ceases. 18 –23 Furthermore, the association of O. formigenes and USD/urinary oxalate is highly variable. Although the negative association between USD and oxalate-degrading bacteria clearly reflects a role for the gut microbiota in preventing USD, the variability in regard to colonization status, association with urinary oxalate, and effect of oxalate-degrading probiotics necessitate an alternative hypothesis.
Urolithiasis has been increasingly recognized as a complex systemic illness. Studies have linked USD to a variety of cardiovascular risk factors (hypertension, diabetes, and metabolic syndrome), chronic kidney disease, and asthma. 24 –26 Interestingly, the increase in USD incidence corresponds to similar increases for its comorbidities, all of which have known associations with the gut microbiota. 27 –32 These corresponding trends indicate that broad systemic changes to the gut microbiota, rather than loss or variation of specific functional bacteria, may promote USD and comorbidities. Furthermore, although multiple factors, such as socioeconomic status, diet, host genetics, metabolism, and pharmaceuticals, have been implicated in the incidence of USD, all of these factors are also strongly associated with the gut microbiota. 33 Thus, an alternative hypothesis for the contribution of the gut microbiota to USD is that the gut microbiota is an intermediate link between the multifactorial causes of USD and the manifestation of the disease (Fig. 1).

Hypothetical pathways that link the multifactorial origins of USD through the gut microbiota. Factors on the left are hypothesized to influence the structure and function of the gut microbiota in a way that facilitates USD. USD = urinary stone disease.
The purpose of this review is to examine the evidence that supports or refutes the alternative hypotheses that the gut microbiota provides protection against USD through (1) specific functional bacteria or (2) diverse microbial networks. Such a review of the literature will identify the limitations of using oxalate-degrading bacteria as probiotics and help to refine more effective and persistent bacteriotherapy strategies for the prevention of USD.
Materials and Methods
We performed comprehensive searches in Ovid Embase (1974–January 2018), Ovid MEDLINE (1946–January 2018), Cochrane CENTRAL (1946–January 2018), Scopus (1996–January 2018), and Web of Science Core Collection-Science (1965–January 2018) for calcium oxalate urinary stones, gut microbiota, oxalate metabolism, oxalate-degrading bacteria, and probiotics. Article titles and abstracts were reviewed to identify publications evaluating the role of the gut microbiota in oxalate metabolism and the pathophysiology of USD, as well as the bacteriotherapies to inhibit USD. Non-English language articles, abstracts, book chapters, and editorials were excluded and only used to identify primary sources. All relevant publications were categorized by subtopic and selected for inclusion based on relevance to the scope of this review.
For articles that examined the association between the whole gut microbiota and either USD or oxalate metabolism, we performed a meta-analysis to determine which bacterial genera were common across studies. Primary sources of data were used when available. 34 –39 Otherwise, results reported in the article were used. 40,41 For primary data, differential abundance analysis of operational taxonomic units (OTUs) from healthy and USD groups was identified with the DESeq2 algorithm. 42 From the differentially abundant OTUs, heatmaps were constructed to illustrate OTUs from different genera enriched in either healthy or USD groups between the studies. Only those genera found in more than one study were included in heatmaps. To evaluate potential common interactions between the gut microbiota and USD/comorbidities, we used publically available data associated with the American Gut Project (AGP), which is a comprehensive open-source and open-access microbiome 16S rRNA reference dataset. 43 We identified OTUs associated with cardiovascular disease, obesity, diabetes, and kidney disease using differential abundance analysis from a total of 88 individuals for each group in comparison to 88 individuals randomly selected among those who self-identified as both healthy and not having any of the comorbidities listed above. The sample number was chosen based on the smallest group size in the dataset (individuals with kidney disease). For cardiovascular disease, obesity, and diabetes, 88 individuals were randomly selected from each group within the database. Random samples were selected by sorting samples in metadata files by the healthy or diseased variables, and then selecting the first 88 samples with the correct metadata classification. In addition to the meta-analysis of comorbidities, we incorporated data from the meta-analysis regarding USD patients to identify common microbial genera that were depleted in individuals with USD or a comorbidity.
Results
The role of oxalate-degrading bacteria
In 1980, using media that contained oxalate as a sole source of carbon and energy, Dawson et al. 44 isolated a strictly anaerobic bacterium that relied exclusively on oxalate as a substrate to obtain energy. This isolate was later described as O. formigenes by Allison et al. 45 Since that time, numerous oxalate-degrading bacteria from mammalian sources have been described, such as Lactobacillus, Bifidobacterium, Enterococcus, Clostridium, Eggerthella, Providencia, Streptococcus, and Leuconostoc genera. 14
The primary focus of research surrounding oxalate-degrading bacteria has been on the oxalate specialist O. formigenes. For the purposes of this review, the research on oxalate-degrading bacteria can be broken down into two categories: (1) the colonization of O. formigenes in healthy and USD patients (Table 1) and (2) the effect of oxalate-degrading probiotics on urinary oxalate (Table 2). In regard to O. formigenes colonization, 24 studies ranging from 1989 to 2018 were chosen for inclusion. Colonization by O. formigenes ranged from 11% to 100% in healthy individuals and 0% to 100% in patients with USD, with a significant group difference in 9 out of the 11 studies that statistically compared groups. 11,12,39,46 –50 In addition, colonization by O. formigenes had a significant impact on urinary oxalate excretion in 7 of the 13 studies that reported the result. 10,11,48,49,51 –54 Finally, all four studies that investigated the impact of antibiotics on O. formigenes colonization demonstrated reduction in the colonization rates, making the widespread use of antibiotics a real concern since O. formigenes is susceptible to the most common antibiotics used in clinical practice. 11,50,55,56 Some of the factors that may contribute to the wide range of results reported include disparate study distributions of patient age 57 and comorbidities 12 or differences in detection technique (culture-based, polymerase chain reaction [PCR] with primers associated with the oxalyl-CoA decarboxylase gene from O. formigenes [oxc], or high-throughput sequencing). 58 –62
Significant difference in colonization rate (significance), association between colonization and Urox, and colonization and ATB is given.
Only colonization of 12-year-old children indicated here.
Colonization status affected urinary oxalate in recurrent stone formers but not first-time stone formers.
Only significant difference in urinary oxalate for individuals with USD that were also colonized by O. formigenes.
ATB = antibiotic; ND = not determined; NS = not significant; PCR = polymerase chain reaction; S = significant; Urox = urinary oxalate excretion; USD = urinary stone disease.
Here, we indicate whether experiments were done in humans or rodents (population), the study design, the duration of probiotic administration (duration), persistence of probiotics after administration ceased (persistence), and the effect of probiotics on Urox.
Highly dependent of dietary oxalate.
Persistence was only maintained with dietary calcium levels at 0.01%.
There is only a significant difference in low calcium diet.
Urinary oxalate levels initially fell, but returned to baseline while still taking probiotics.
RCT = randomized controlled trial.
Given the strong negative association between colonization with O. formigenes and USD/urinary oxalate, several studies have examined the effect of O. formigenes probiotics on urinary oxalate in both rodents and humans, as well as probiotics composed of facultative oxalate-degrading bacteria. From 12 studies utilizing O. formigenes, 8 studies saw a significant reduction in urinary oxalate (Table 2). 13,20,63 –69 However, the only three randomized, placebo-controlled, double-blinded studies with O. formigenes probiotics, which were conducted with primary hyperoxaluria (PH) patients, did not show any effect of the probiotic on urinary oxalate excretion. 22,23,70 Despite the effectiveness of O. formigenes probiotics, the bacteria were rapidly lost in four of the five studies that quantified persistence of the bacteria after cessation of the probiotics. 20,64 –66 From 11 studies involving lactic acid bacteria, 8 reported a significant reduction in urinary oxalate (Table 2), 15,19,21,37,56,71 –73 whereas one prospective single-arm study 74 and two randomized, placebo-controlled studies did not. 8,18 Regarding persistence of colonization, two of three studies reported a loss of bacteria and/or function in <2 weeks. 37,72 However, in those studies that involved fecal transplants from a wild mammalian mammal that consumes a high oxalate diet, the persistence was maintained at least 1 week and up to 9 months. 35,37 The efficacy of probiotics does not appear to be associated with the duration of administration or the type of oxalate-degrading bacteria given. However, in one study that directly compared fecal transplants to oxalate-degrading bacteria, both efficacy and persistence were greater for the fecal transplant preparation. 37 Overall, several conclusions from the above studies are apparent: (1) O. formigenes is highly sensitive to antibiotics; (2) colonization by O. formigenes is typically higher in healthy individuals than in USD patients, but with high variability between studies; (3) the association between colonization by O. formigenes and urinary oxalate excretion is unclear; (4) the species of oxalate-degrading bacteria and duration of probiotic administration do not appear to impact efficacy and/or persistence; (5) oxalate-degrading probiotics were effective in 14 of the 20 studies examined in this study, with the bacteria and their function typically lost after administration ceases; and (6) patients with PH may not respond to O. formigenes probiotics.
The role of the whole gut microbiota
Several factors have warranted studies that examine the broader contributions of the gut microbiota to oxalate metabolism and USD. First, although colonization by O. formigenes is typically higher in healthy individuals compared to USD patients, colonization in the healthy population can be as low as 11% 75 with colonization as high 100% in the USD population. 76 These data indicate that the presence of O. formigenes alone is not a good predictor of stone risk. The second factor that warrants broader microbiome studies is the inconsistency in probiotic study results. Although probiotics usually reduce urinary oxalate, they are not always effective. Furthermore, colonization by probiotic bacteria is typically transient. Finally, there is a strong negative association between antibiotic use and the loss of O. formigenes. Antibiotics have a broad negative effect on gut bacteria that extends beyond O. formigenes.
The gut microbiota is composed of as much as 10 13 bacteria that reside primarily in the colon. 77 Within this gut microbiota, there is considerable individual variability associated with a diverse array of environmental factors such as diet, 34,78 age, 33 activity levels, 79 antibiotic use, 61 geography, and health status. 80 Furthermore, microbial populations within the gut exist in functionally integrated, symbiotic networks, rather than as isolated functional species. 81 Given the level of microbial diversity and functional integration within the gut microbiota, it is possible that the contribution of the gut microbiota to the prevention of USD and to oxalate metabolism extends beyond oxalate-degrading bacteria alone.
To determine if the contribution of the gut microbiota to oxalate metabolism and USD extended beyond that of O. formigenes and other oxalate-degrading bacteria, we conducted a meta-analysis of studies that used high-throughput sequencing of the gut microbiota associated with these phenotypes (Fig. 2). From the literature, a total of five studies associated with USD were chosen, 38 –41 and four studies associated with oxalate metabolism. 34 –37 Primary sources of data were used for meta-analysis when available. Three studies did not meet this requirement, and the results as reported by the authors were used. 40,41 The meta-analysis revealed that, although results were variable between studies, there were genera commonly associated with both healthy individuals and oxalate metabolism. In the healthy and oxalate metabolism group, Coprococcus and Oscillospira were the most frequent genera. Bacteroides were the most common genera in both USD and healthy patients (Fig. 2). Results also indicate that there may be a greater diversity of bacteria enriched in healthy individuals than in patients with USD. Interestingly, although Oxalobacter sp. was commonly associated with oxalate metabolism, it was only enriched in healthy individuals in one of the four studies examined. In contrast to studies involving O. formigenes probiotics, one study using fecal transplants saw an increase in the diversity and relative abundance of Oxalobacter sp. and other Oxalobacteraceae after cessation of fecal transplants and a dietary oxalate washout period. 37
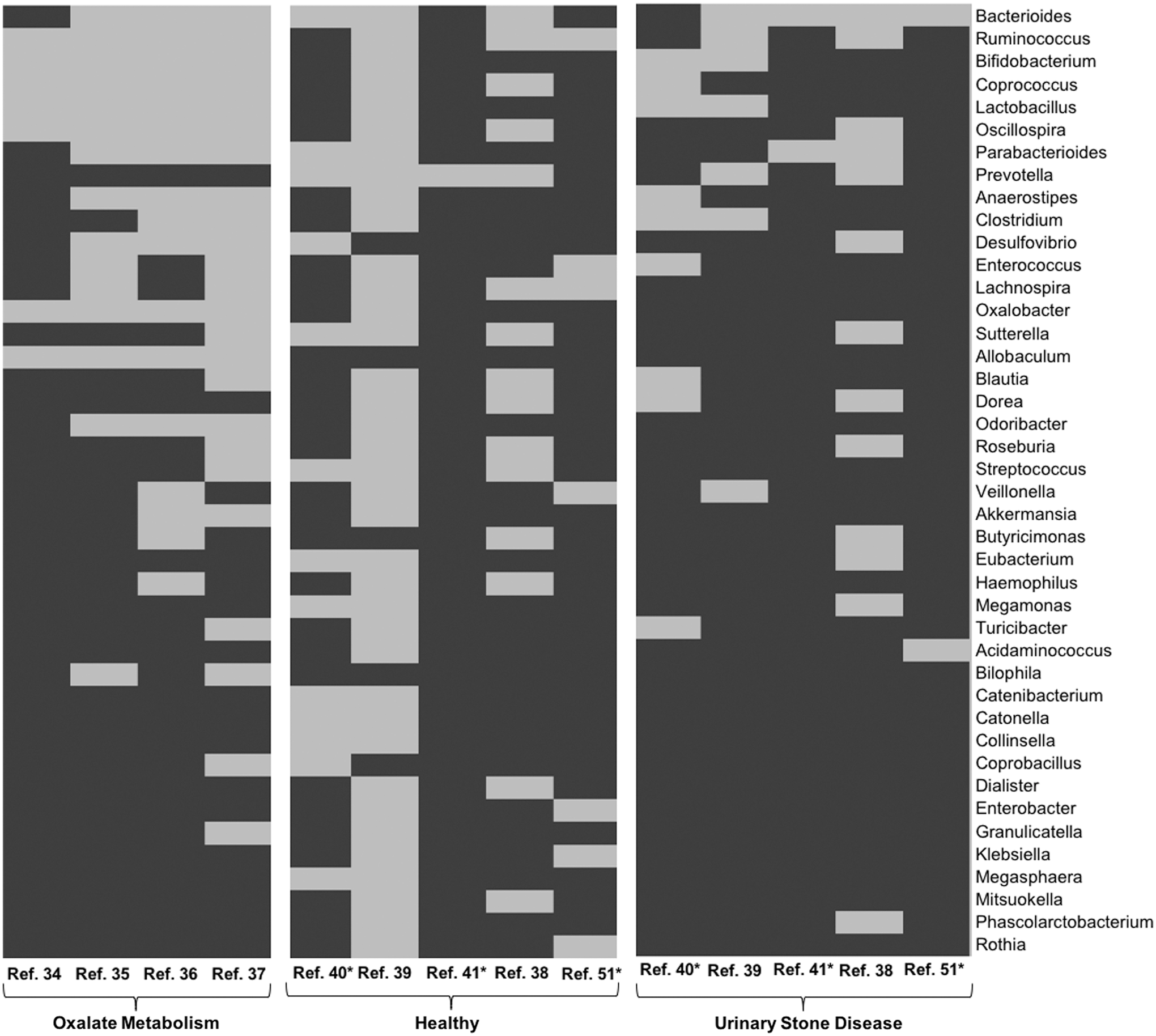
Microbial genera associated with oxalate metabolism, healthy individuals, or those with USD. Gray represents genera with OTUs enriched in each group, black indicates genera with no OTUs enriched. *Primary sources of data not available. Only genera present in more than one study are shown. OUT = operational taxonomic unit.
To determine if broad shifts in the gut microbiota is a common driver facilitating the onset of comorbidities, we conducted an analysis of data associated with the AGP in combination with data derived from the above studies on gut microbiota and USD. Specifically, we looked at individuals who had self-reported diabetes, cardiovascular disease, obesity, or kidney disease, compared to healthy individuals. The analysis shows a considerable overlap in microbial genera depleted in diseased individuals, particularly between kidney disease and USD (Fig. 3).
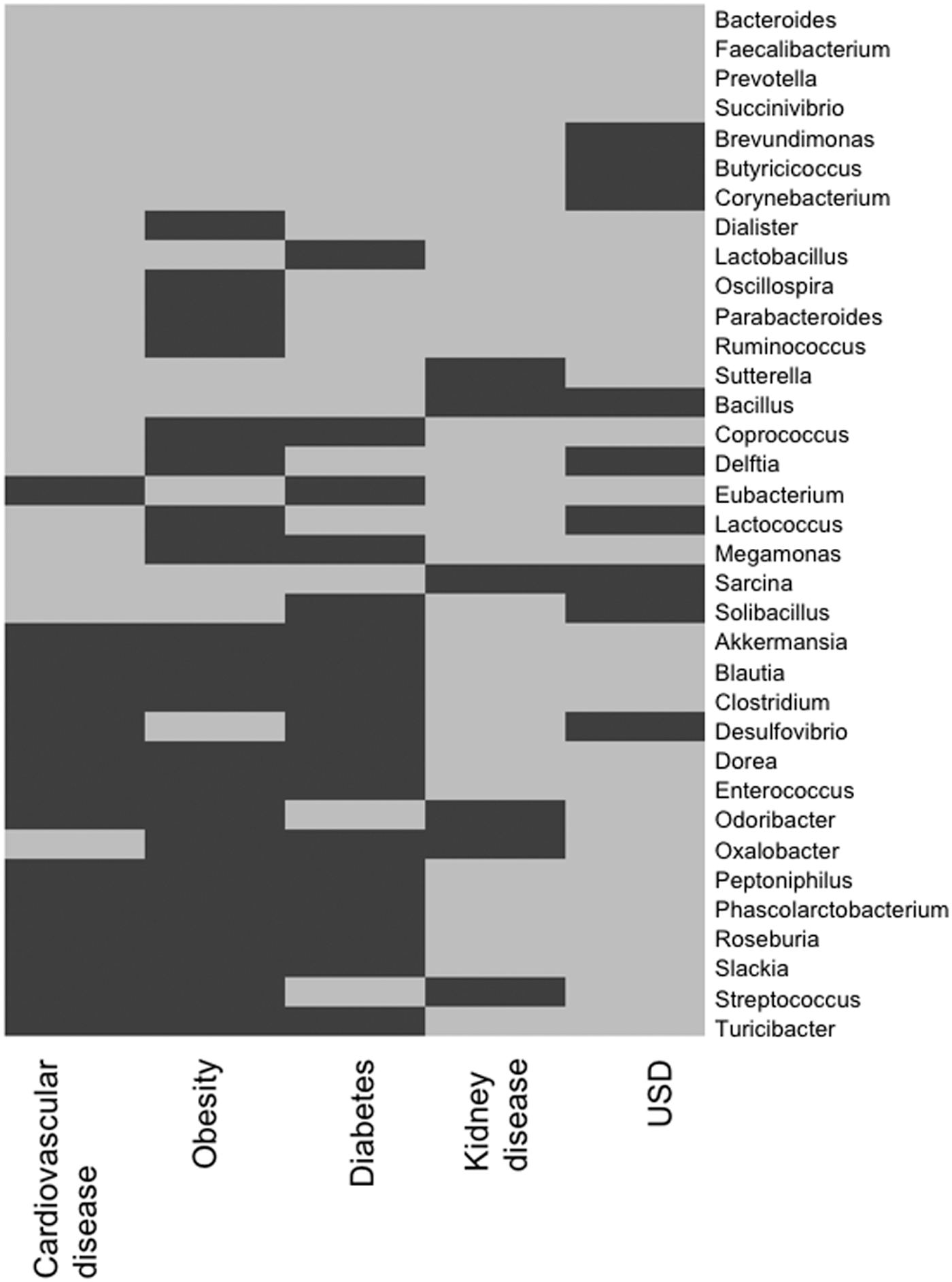
Microbial genera associated with USD and comorbidities. Data from Figure 2 were integrated for the USD columns. Gray indicated bacteria depleted, black indicates bacteria not depleted. Only genera depleted in more than one disease are shown.
Discussion
The incidence of USD is rapidly increasing nation-wide despite current strategies to mitigate the disease. 1,3 The broad-scale trend of increasing prevalence of USD and comorbidities is indicative of population-wide changes to public health. 24 –26 With the known links between USD and bacteria that reside in the gut, one potential factor driving the trend of increasing prevalence is the microbiome. 14 Oxalate is present in ∼70%–80% of kidney stones, is broadly consumed in the diet as well as produced endogenously from several dietary precursors, and is metabolized exclusively within the gut microbiota, with no contribution from the host. 82,83 These characteristics of USD and oxalate metabolism set up the hypothesis that oxalate-degrading bacteria within the gut are vital for the inhibition of USD, with particular emphasis on the unique oxalate-degrading specialist, O. formigenes.10 17 However, with mixed and often unclear results along with advances in sequencing technology, an alternative hypothesis has emerged, that the contribution of the gut microbiota to oxalate metabolism and protection against USD extends beyond O. formigenes. This review examined the literature to provide evidence for and against both hypotheses, with the specific goal of informing the development of the most effective and persistent bacteriotherapies to inhibit USD.
To date, the primary focus of research into the contribution of the gut microbiota to USD has been O. formigenes. In this study, we have shown that studies consistently report a higher level of colonization by O. formigenes in healthy individuals compared to patients with USD (Table 1). Furthermore, all studies that examined the effect of antibiotics on colonization by O. formigenes have seen a strong negative correlation. However, from 14 studies, 6 reported no significant effect of O. formigenes colonization on urinary oxalate levels (Table 1). Although colonization by O. formigenes is typically higher in the healthy population, colonization values ranged from 11% to 100% (Table 1). Colonization by O. formigenes in patients with USD ranged from 0% to 100%. Studies that have used O. formigenes as probiotics to reduce urinary oxalate levels have been successful, except in cases of patients with PH. However, colonization is typically ephemeral with bacteria quickly becoming undetectable after administration and/or a high oxalate diet ceases (Table 2). Collectively, these results clearly indicate that, although O. formigenes is important for oxalate metabolism and protection against USD, this OTU alone is neither necessary nor sufficient to maintain oxalate metabolism or protect against USD. In addition to studies focused on O. formigenes, several studies have found a diversity of oxalate-degrading bacteria from humans and other mammalian sources. 14,16,33,36,37 Use of these bacteria as probiotics have similar effects at reducing urinary oxalate and in persistence as O. formigenes (Table 2).
Compared to studies on O. formigenes and other oxalate-degrading bacteria, those that have focused on the contribution of the whole gut microbiota to oxalate metabolism and USD are in their infancy. However, these studies have shown that a broad diversity of bacteria is associated with oxalate metabolism, protection against USD, and facilitation of USD (Fig. 2). Interestingly, although Oxalobacter is regularly associated with oxalate metabolism, it was only associated with healthy individuals in one of the five whole gut microbiota studies examined. Beyond O. formigenes, several taxa were consistently reported to be associated with healthy individuals and oxalate metabolism, particularly Bacteroides, Ruminococcus, Bifidobacterium, Coprococcus, Lactobacillus, Oscillospira, and Parabacteroides (Fig. 2). However, Bacteroides, Ruminococcus, Bifidobacterium, Coprococcus, and Lactobacillus were also enriched in USD patients in one to four studies, indicating that specific OTUs within these genera may be important for the formation or inhibition of stones. Further evidence that a broad diversity of bacteria is important for oxalate metabolism and protection from USD comes from studies that used fecal transplants to induce oxalate metabolism. In these studies, Oxalobacter colonization persisted for up to 9 months. 35 In fact, in one study, the diversity and abundance of Oxalobacter and other Oxalobacteraceae was higher a week after transplants and a high oxalate diet stopped compared to directly after transplants. 37 This provides further evidence that colonization by Oxalobacter is facilitated by association with a diversity of bacteria in the transplant preparation. It is important to note that, although the microbiota composition associated with comorbidities to USD was unique, there were several genera depleted in diseased individuals that were common to all diseases (Fig. 3). This indicates that perhaps there are common mechanisms between the absence of certain bacteria and the onset of USD and comorbidities.
One difference between studies that have focused on O. formigenes using O. formigenes-specific primers and studies that have focused on the whole microbiota is that the use of O. formigenes-specific primers can detect a difference between healthy and USD groups when high-throughput sequencing does not. 39,40 Barnett et al. 75 found a threefold difference in the colonization rate of healthy individuals depending on the molecular technique used, and Kaufman et al. 10 saw a difference between culture and PCR techniques. It must be noted that, although Suryavanshi did not detect a difference in O. formigenes with high-throughput sequencing in their study, we did detect a difference in independent analysis. The conflict in the detection of a difference of O. formigenes colonization in healthy vs USD individuals using O. formigenes-specific primers or high-throughput sequencing is something that must be resolved. Finally, one aspect that has been revealed by studies on the whole gut microbiota is that dysbiotic bacteria that facilitate USD may potentially play an important role in the onset of disease (Figs. 2 and 3). However, it appears that the loss of beneficial bacteria may be more important than the acquisition of dysbiotic bacteria.
Implications for the management of USD
The implications of this review for the management of USD can be broken down into two sections: immediately actionable and requiring additional research. Although the mechanistic links between microbial network in the gut and USD have yet to be established, evidence strongly supports the observation that diverse bacteria in the gut are important for the inhibition of USD. Therefore, activities that promote gut microbiota diversity may help to inhibit primary or recurrent stone formation, such as exercise, a low-fat and low-sugar diet, and the restricted use of antibiotics. In fact, a high oxalate vegetarian diet may actually inhibit rather than promote USD and lower rather than increase urinary oxalate supersaturation. 78 The lower incidence of USD in vegetarians may reflect a more diverse microbiota, since the gut microbiota diversity increases with greater intake of plant-based foods. 84
In addition to the immediately actionable strategy to help inhibit USD, the management of USD in association with the gut microbiota would benefit from additional research in the following areas: first, whole microbiota studies indicate that dysbiosis may play a role in USD. However, this is an area that has been completely unexplored. In conjunction to minimizing the use of antibiotics, introducing the restoration of the gut microbiota after a course of antibiotics may help to prevent the loss of bacteria important for oxalate metabolism. Studies with oxalate-degrading probiotics have yielded promising results; however, the results of our meta-analysis reveal that incorporating a broader diversity of bacteria into probiotics may be a more effective and persistent solution. Studies that examine the contribution of the whole gut microbiota to oxalate metabolism and USD are relatively new. Therefore, more studies are needed to pinpoint which bacteria or communities of bacteria are most important for protection against USD. Finally, the mechanistic link between the functional microbial networks and their role in maintaining a healthy balance of oxalate needs to be understood. Doing so will allow us to specifically target bacteriotherapy strategies to individual patients, to maximize their potential for success, although minimizing the burden on both patients and clinicians. It has previously been established that the simpler the intervention for the patient, the more likely they are to conform to it.
Conclusions
Evidence to date strongly suggests that there are intimate links between the gut microbiota, the balance of oxalate, and USD that go well beyond O. formigenes and other oxalate-degrading bacteria. Rather than rule out the importance of O. formigenes and other oxalate degraders, this review consistently points to the complementary role of the functionally integrated communities of bacteria on oxalate metabolism and urolithiasis pathogenesis. The successful development of bacteriotherapies to inhibit USD will need to incorporate the functional microbiota concept along with changes to diet and lifestyle that affect it. More research is needed to explore these mechanistic links and to tailor treatment options to individual patients in a clinical setting.
Footnotes
Acknowledgment
We would like to express our gratitude to Marian Simonson, Assistant Director of the Cleveland Clinic Floyd D Loop Alumni Library, for all her support, attention, and kindness during the literature search strategy and review.
Author Disclosure Statement
None of the authors have any relevant conflicts of interest to declare.