
Abstract
Purpose:
We performed a systematic review of the literature regarding the diagnosis and treatment of caliceal diverticulum (CD).
Methods:
The search strategy was conducted according to the Cochrane review guidelines for systematic reviews and Preferred Reporting Items for Systematic reviews and Meta-Analyses checklist.
Results:
In total 1189 titles and abstracts were reviewed, of which 101 were selected for article evaluation. Of these 101 articles, 40 were selected for inclusion after full article evaluations. In the extracted article, intravenous urography (IVU), rather than CT urography, was the main imaging tool for diagnosis, although many articles had failed to provide any imaging modality information. The extracted articles included 88, 153, and 487 patients who underwent shock wave lithotripsy (SWL), flexible ureteroscopy/retrograde intrarenal surgery (fURS/RIRS), and percutaneous nephrolithotomy (PCNL), respectively. Stone-free rates were 21.3% (SWL), 61.4% (fURS/RIRS), and 83.0% (PCNL). The complication rates were 8.0% (SWL), 3.3% (fURS/RIRS), and 11.9% (PCNL). There was incomplete and inconsistent reporting of even basic clinical parameters, such as the size and location of the CD, number of stones, outcomes, and complications. There was a striking lack of follow-up data, despite a known high recurrence rate. The literature on laparoscopic management was too sparse to analyze.
Conclusions:
This meta-analysis revealed that there are not enough high-quality studies to evaluate the ideal strategy for the diagnosis and treatment of CDs. This systematic review emphasizes (a) the importance of contrast imaging for CD diagnosis, (b) higher success rates but also higher complication rates in PCNL compared with SWL and FURS, and (c) the need for standardized reporting of outcomes to include complications, number of interventions, symptom resolution, stone clearance, and CD ablation.
Introduction
C
CD is a rare disease with an unknown incidence, reported in 0.21%–0.6% of intravenous pyelographic investigations 3 –5 and occurring bilaterally in nearly 3% of patients. 6 Patients usually present with hematuria, pain, or sepsis, and form stones in up to 50% of cases. 6,7
Stones are thought to be due to urinary stasis, whereby urine fills the cavity, and stagnates due to the narrow neck, precipitating calculi crystals. 8,9 However, an underlying metabolic abnormality for stone formation has been reported in over 50%. 10,11
The critical problem for patients and also physicians is that there has been no consensus on the best treatment strategy to manage CDs. Various treatment modalities have been proposed from conservative treatment, shock wave lithotripsy (SWL), percutaneous nephrolithotomy (PCNL), flexible ureteroscopy/retrograde intrarenal surgery (fURS/RIRS), and partial or total nephrectomy for adults 6,12 –15 and for children. 16 Management tends to follow an upward trend from the less invasive to the more invasive.
We aimed to perform a systematic review of the literature to gain a better understanding of how to diagnose and treat CD, as well as to evaluate the different treatment modality efficacy and safety rates. We also aimed to assess the quality of the published literature to determine whether improvements in reporting and study design are needed.
Methods
Search strategy and study selection
The search strategy was conducted according to the Cochrane review guidelines for systematic reviews and Preferred Reporting Items for Systematic reviews and Meta-Analyses checklist.
Relevant studies were identified from MEDLINE (1966–December 2017), EMBASE (1980–December 2017), Cochrane Central Register of Controlled Trials - CENTRAL (in The Cochrane Library–Issue 1, 2017), CINAHL (1872–December 2017), Google Scholar, and Individual urological journals.
Terms used included: “ureteroscopy,” “flexible ureteroscopy,” “PCNL,” “SWL,” “stones,” “diverticulum,” “urolithiasis,” “calculi,” “calyceal,” and “calyceal diverticulum.”
Mesh phrases included: (“Diverticulum”[Mesh]) AND (“Calculi”[Mesh]) (“Diverticulum”[Mesh]) AND (“Urinary Calculi”[Mesh]) (“Diverticulum”[Mesh]) AND (“Kidney Calices”[Mesh]) (“Diverticulum”[Mesh]) AND (“Urinary Calculi”[Mesh]) AND (“Kidney Calices”[Mesh]) (“Diverticulum”[Mesh]) AND (“Calculi”[Mesh]) AND (“Kidney Calices”[Mesh]).
Eligibility criteria
All studies reporting their centers' experience with CDs were included. The literature was searched for reviews attempting to classify caliceal diverticula. Only studies on children and adult humans were included. There was no language restriction. References within individual articles were searched for further included studies. Authors of included studies were contacted, wherever data were not available or not clear.
Selection of relevant articles
Two reviewers (O.A. and I.H.) identified studies for potential inclusion. Disagreement between the two extracting authors was resolved by consensus. We limited our inclusion of case series to those reporting on 20 or more to allow for a more robust understanding of the disease from a larger series.
Data extraction and statistical analysis
The first author (I.H.) extracted data from studies relevant to classification of CD, outcomes of various management regimens, and complications. Interventions included SWL, FURS/RIRS, PCNL, laparoscopic surgery, and open surgery. The following variables were extracted: country origin of article, gender, patient's symptom, presence of infection, characteristics of CD and bearing stones, imaging modalities, treatment method outcome: stone-free rates, symptom-free rates, diverticulum-free rates, or no need for further interventions, stone sizes, and complications. To ensure the robustness of the review, the second and third authors (O.A. and F.A.) independently verified all the data.
Similar data were pooled into a cumulative meta-analysis, in an intention to treat basis, to allow a numerical representation of the results.
We aimed to perform a quality assessment of harms using the McHarm scale for each included study. 17 We used Review Manager (RevMan 5.3) to plot the quality assessment of Harms tables.
Results
The literature search flowchart is depicted in Figure 1. In total, 1189 titles and abstracts were reviewed, of which 101 were selected for article evaluation. Of these 101 articles, 40 were selected for inclusion after full article evaluations. Only 1 of 40 studies was an international conference abstract describing a classification system, 18 otherwise all were fully published articles.
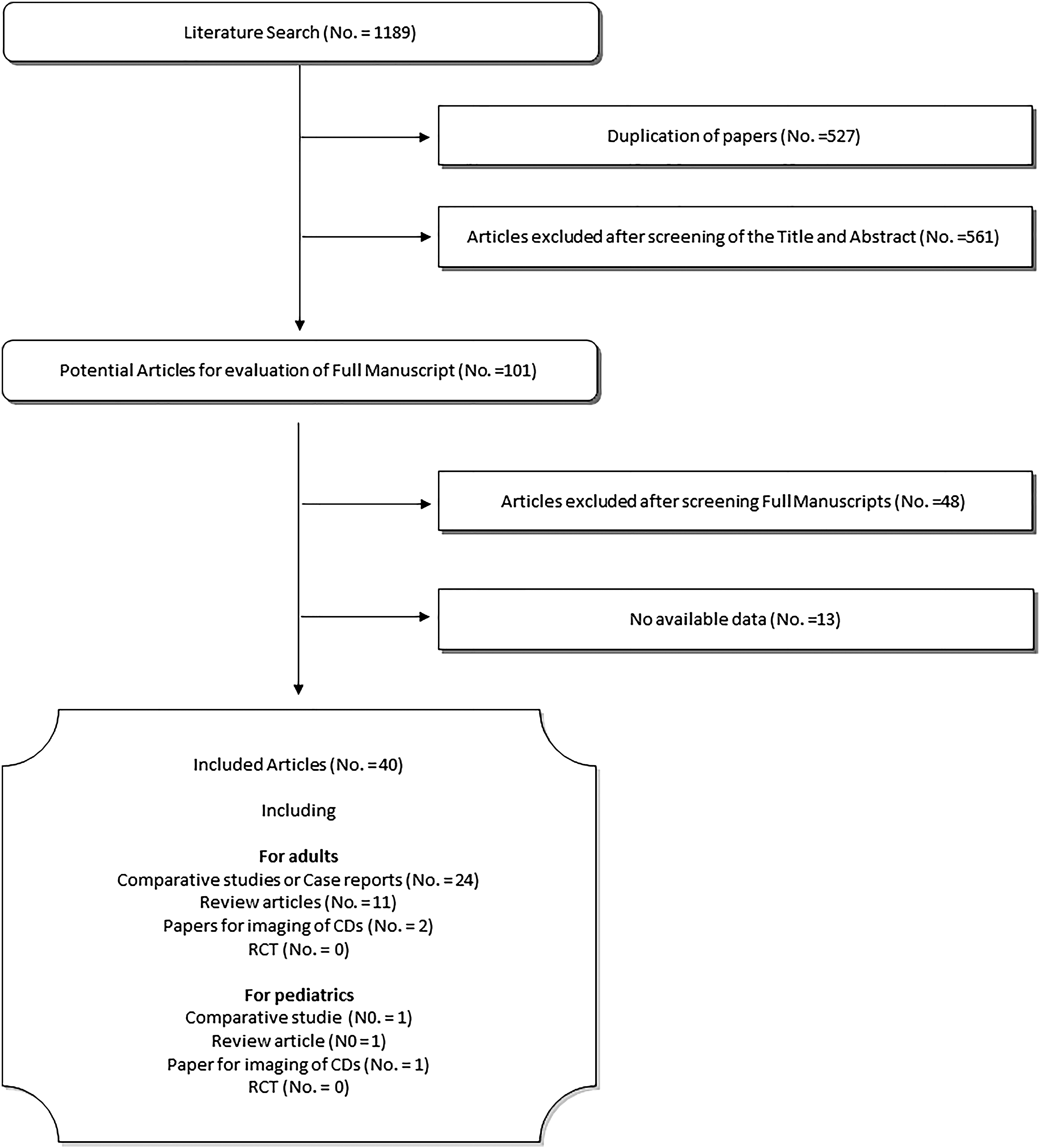
Flowchart for article selection process of the review.
Overall, 37 of 40 articles reported outcomes for adult CDs, including 24 comparative studies/case reports, 8 –11,18 –37 11 review articles, 1 –6,12 –15,38 and 2 imaging articles. 39,40 The 24 comparative studies/case reports consist of 18 reports of surgical treatment outcome, 8,19 –35 three reports of classification/treatment algorithm of CD, 18,36,37 and three reports of metabolic analysis of CD patients. 9 –11
Three of 40 articles were for pediatric CDs, including 1 comparative study to report surgical outcomes, 7 1 review article, 16 and 1 imaging article. 41
Characteristics of included studies
The included 40 articles were published between 1941 and 2017, with the majority conducted in the USA (26/40), nine conducted in Europe, three in the Middle East, and one each in Australia and Canada. Of 24 comparative studies/case report studies, 18 adult studies 8,19 –35 and 1 pediatric study 28 were conducted to report surgical outcomes and thus enrolled in the meta-analysis in this study. All of these 19 studies were retrospective cohort observational studies, with no randomization or control groups, involving cases between 1983 and 2016. A total of 757 patients (759 renal units) were enrolled and 18 of 19 studies (94.7%) were reports of a single-center experience (Table 1). The methodological quality assessment was difficult due to the disparity of the included studies; however, we aimed to include all the published literature on CD to give a wide picture of the evidence.
There were four studies reporting on the outcomes of SWL, 5 studies on RIRS, 14 studies on PCNL, 1 study on each multitreatment modalities, including PCNL followed by SWL, laparoscopic, and open surgery.
In total, 757 patients were included, of which 60.1% were female (429 women) and 39.9% males (285 men); 20 patients did not have a specific sex reported. The average age reported ranged from 35.4 to 54.7 years of age. There was no predominant side of CD with few bilateral CD (286 right/284 left/1 bilateral/187 unclear). The most frequently present symptom of CD patients was pain (68%–100%). Symptoms also included infections (9%–74%) and hematuria (12.8%–23%). The asymptomatic rate ranged from 0% to 20% (Table 2).
— = unclear; CD = caliceal diverticulum; UTI = urinary tract infection.
Imaging
Diagnostic imaging modality for CDs
Table 3 shows the imaging modality used to detect CDs in 19 studies. Intravenous urography (IVU) was reported as the main imaging tool for diagnosis of CDs, although 9 of 19 articles had failed to provide any imaging modality information.
— = unclear; IVU = intravenous urography; NCCT = noncontrast computed tomography; U = upper pole; M = middle pole; L = lower pole.
Accurate imaging assessment for surgical treatment
Table 3 also showed clinical information about CDs and stone-bearing status in 19 studies. More than half of these articles failed to report CD size and number (Table 2); however, CD position (upper/middle/lower pole) had been described well in almost all of the articles. The location in the upper pole (51.9%) was more common than middle (27.2%) and lower pole (20.9%), as previously reported. 3,4
Surgical treatment options for CDs
Shock wave lithotripsy
Among the studies examined, a total of 88 patients with 89 renal units underwent SWL, of which, the stone-free rate was only 21.3%. Sixty percent of the patients were symptom free after their procedure. The combined complication rate was 8.0% (Table 4). None of the patients had had any treatment before the SWL.
— = unclear; SFR = stone-free rate.
Flexible ureteroscopy/retrograde intrarenal surgery
A total of 153 patients underwent FURS/RIRS, of which, the stone-free rate was 61.4%, and the symptom-free rate was 67.9%. The complication rate was 3.3% (Table 5). The majority (60.7%) of the patients had had previous failed treatment of other modalities, including SWL and PCNL.
— = unclear.
Percutaneous nephrolithotomy
In total, 487 patients (488 renal units) underwent PCNL as treatment for their CD. Of the extractable data 83.0% (341/411) were stone free, 90.8% (277/305) were symptom free, 11.9% developed complications, and 34.2% (53/161) had had previous treatments (Table 6).
— = unclear; PCNL = percutaneous nephrolithotomy.
Others: multiple treatment modalities (PCNL followed by SWL), laparoscopic surgery, and open surgery
Very few studies met our inclusion criteria. Only 1 study for 10 adult patients reported multiple modality treatment, PCNL followed by SWL. 21 The stone-free rate was 90% and both symptom free and no further treatment rate was 100%. As regards surgical complications, 1 of 10 cases showed pleural effusion (10%) (Table 7).
— = unclear.
Only one study for four pediatric patients had had laparoscopic/open surgery for their CD, of which all were stone free and symptom free, with no complications 28 (Table 7).
Discussions
Out of over 1000 articles identified by our search, only 40 met our inclusion criteria despite being relatively inclusive regarding quality standards. The CD literature is not only sparse, but inconsistently reported, making analysis of outcomes particularly challenging.
Imaging for diagnosis of CDs
Noncontrast-enhanced computed tomography (NCCT) has become the standard for diagnosing acute flank pain or suspected urolithiasis, and has replaced IVU. The advantage of noncontrast imaging must be balanced against loss of information on urinary collecting system anatomy and renal function. Indeed, NCCT is significantly more accurate than IVU in evaluating patients with suspected acute urolithiasis. 42
To get an accurate diagnosis of CD, however, a contrast study has to be performed to assess the anatomy of renal collecting system. A previous study reported that CD mostly becomes apparent by IVU because there is inherent connection with the collecting system. 40 In fact, EAU guidelines only recommend a contrast study as grade A when stone removal is planned and the anatomy of the renal collecting system needs to be assessed. 43 Nonetheless, this guideline recommended enhanced computed tomography or IVU just as grade C in complex cases. The widespread adoption of noncontrast CT in place of IVU may delay the accurate diagnosis of CD, and a contrast study should be more strongly recommended, especially in complex cases.
Shortcomings in CD imaging in the literature
Surprisingly, there was a lack of information in the extracted studies of basic anatomical details of CD, size and number of any stones, and imaging modality. Previous treatment algorithms indicated that anterior–posterior position of CD affected the operative outcome and have to be considered in choosing optimal treatment options. 36 –38 These articles recommended laparoscopy for anterior CD and PCNL for posterior CD. However, anterior–posterior information of CD had not been described in the vast majority of articles—only two articles included adequate data. 34,35 We suggest that the surgeon should assess the three-dimensional data of CD for making optimal treatment strategy, including anterior–posterior data, and the future studies of CD should provide the three-dimensional information of CD.
Surgical treatment of CDs
Shortcomings in surgical treatment of CD literature
Apart from one multicenter report, 34 the entire literature consists of single institutional experience and no systematic review articles. As a result, the literature is likely to reflect profound institutional bias in patient selection and treatment outcomes. The level of evidence is poor, which is unsurprising given the relatively rare incidence of CD, its wide range of clinical features, and the fact that there are numerous treatment options available. Nonetheless, the quality of reporting in the literature is disappointing due to lack of standardization of CD features, inadequate follow-up, and patchy reporting of complications.
Description of patients and CDs
Existing articles often failed to provide size and location of CD (especially anterior and posterior axis), and size and the number of bearing stone (Tables 4–7). These characteristics of the CD and stones are essential to know which treatment is optimal and to rigorously evaluate these treatment efficacies in the literature. In addition, as mentioned in the imaging section above, the description of CD diagnosis is generally poor in the literature. We believe that reports should include the imaging modality since diagnosis of CD is one of many difficult clinical issues to be resolved.
Treatment outcomes
Most of existing articles reported only a stone-free status as an outcome, ignoring the fate of the CD itself or the patients' symptoms. While most of them determined stone-free status as no residual stone (or no fragment) (Tables 4–7), many articles do not state their definition of stone-free status. Besides, when and how to determine stone-free status is also a crucial point, but again many articles failed to provide these data in the literature. In the case of asymptomatic CD, there is no clear indication for surgical treatment as previous articles suggested.
36
–38
We believe that outcome reporting should include not only stone-free status, but also symptom-free status, and
Tables 4 –7 showed the follow-up period of each study. Unfortunately, some articles have no data of follow-up period at all; the range of average follow-up periods was 3–74 months. Many studies had inadequate follow-up for a condition with a high recurrence rate, particularly if the CD has not been eliminated. Imaging follow-up for CD should include a contrast study (IVU or contrast CT), however, most of the articles failed to describe follow-up imaging. Thus, the recurrence rate was often not reported in the existing literature to a reasonable standard.
Can we have enough evidence for development of treatment algorithm or clinical classification of CDs?
Anatomical classification system of CD
There were two previous reports proposing anatomical classification systems of CD, one was from Wulfsohn MA,2 and the other was from Dretler SP. 18 The former categorized CD into four types by communicating location and shape of the neck, in contrast, the latter classified CD into two types by communicating location, size of CD, and symptom. The categorization of CD in this way, however, is of no practical utility in clinical practice.
Clinical treatment algorithm of CD
Three articles proposed different clinical algorithms which aim to direct the best treatment strategy depending on CD characteristics. 36 –38 These algorithms consist of several different clinical parameters, including symptoms, CD location (anterior/posterior and upper/middle/lower pole), thickness of overlying parenchyma, stone size in CD (cutoff; 15, 38 20, 37 and 20–30 mm 36 ). The obvious problem is that there was no evidence base to validate these algorithms and compare their utility.
First, we examined the impact of location of CD on treatment outcome. Some articles showed that the location of CD, such as upper/mid/lower pole, had no influence on treatment outcome of CD in RIRS 26,29 and PCNL. 27,35 However, all algorithms involved location of CD as selection criteria. Furthermore, other stone location information, such as anterior and posterior, was used in the algorithm selection criteria, especially in the selection of laparoscopy (for anterior) and PCNL (for posterior). Nonetheless, there is no clinical data in our study to support this idea. In fact, the majority of articles failed to provide any of these data (see Accurate imaging assessment for surgical treatment section).
Second, we examined the cutoff value of CD size for choosing optimal treatment. Some articles showed there was a significant association between successful outcome and stone size in CD treatment in RIRS, 29 although a recent article showed no correlation between success outcome and stone size in CD in PCNL. 35 Generally, for renal stone treatment in non-CD cases, the cutoff value of stone size of 20 mm is used to guide treatment selection in EAU guidelines. 45 However, there is no consensus about legitimate cutoff value of stone size in CD. The cutoff value proposed in these algorithms showed considerable variation (15–30 mm) and is not based on any evidence base, raising doubts about their clinical utility.
Finally, we have to say that there is not enough high-quality clinical data to develop reliable treatment algorithm and validate them for CD treatment. To achieve that, high-quality studies with large number of patients, multi-institutional experience, and prospective study design with standardized reporting are needed.
Conclusions
We aimed to investigate and summarize the current clinical consensus of
Footnotes
Author Disclosure Statement
No competing financial interests exist.