
Abstract
Objective:
To evaluate the modifications and feasibility of radical videoscopic inguinal lymphadenectomy (VIL).
Patients and Methods:
From January 2010 to December 2017, more than 200 patients who have underwent bilateral radical inguinal lymphadenectomy for penile cancer in Sun Yat-Sen University Cancer Center. And there were 33 patients who received radical VIL and 174 patients who received open inguinal lymphadenectomy (OIL). According to similar factors of age, body mass index, T stage, and N stage, two matched groups were created with a rate of 1:2, one group received VIL, and another group received OIL. The numbers of harvested lymph nodes, operating times, and complications were compared between the two groups. Descriptive statistical analyses, t tests, chi-square tests, and rank sum tests were performed.
Results:
In total, 93 patients were selected, including 31 patients who underwent bilateral VIL and 62 who underwent OIL. The numbers of harvested lymph nodes did not differ significantly (p = 0.983), the operating time was longer for the VIL than the open lymphadenectomy (p < 0.01), and the morbidity was lower among the VIL than the open lymphadenectomy.
Conclusions:
Modified radical VIL is feasible, practical, and results in reduced morbidity. The dissecting field and the defined plane were critical to these modifications.
Introduction
R
We previously reported on modified radical OILs that were performed with good oncologic outcomes. 1,10 Modifications, including adequate dissection boundaries and dissection in definite anatomical planes, were related to oncologic effectiveness. 1,10 Based on these open surgery experiences and preexperiments, from August 2013 to June 2016, we performed radical VILs with these modifications in patients with clinical disease stages of ≤N2. In this report, we report our series of 81 cases (48 patients) who underwent radical VIL. The clinical characteristics, operating times, numbers of lymph nodes yielded, and morbidities were recorded and compared with those of pair-matched patients who underwent radical OIL from 2010.
Patients and Methods
Patients
This study protocol was approved by the Sun Yat-sen University Cancer Center Ethics Committee (No. 2014 -XJS- 038), and informed consent was acquired from all patients. VIL was performed on clinical stage N1-2 patients and N0 patients with risk factors that included poor differentiation, a tumor size >3 cm, and a stage >T2. Patients with prior inguinal radiation therapy or inguinal surgery were excluded.
Surgery design
The boundaries of dissection were same as those for radical OIL. 1,10
The same template used for standard ILD was marked on the surface of the skin with the patient in the supine position. The video monitor was positioned at the side of head, and the surgeon was positioned between the patient's legs (Fig. 1a, b).
Next, the patient was placed in a low lithotomy position. The body and the thigh were as straight as possible, the thigh was at 20°–30° of external rotation, and the legs drooped naturally (as illustrated in Fig. 1). Finally, the operation table was set at foot height in the horizontal position.
After sterilization, an incision of ∼4 cm was made in the middle of the inferior border of the boundaries. As we have previously reported, beneath the skin, the white, semihyaline membranous tissue between the two layers of Camper's fascia was defined. 1,4 Along this membrane, a fan-shaped space around the incision was exposed as performed in the OILs. The tissues between the superficial layer of Camper's fascia and the fascia lata were sharply dissected, and a space of ∼8 cm × 3 cm was created for the videoscopic devices. In this space, the saphenous vein was also exposed for preservation (Fig. 2a).
Trocar placement: Three ports were used: one 10-mm port was placed 2 cm below the inferior borderline in the middle, and two 5-mm ports were placed each at 0.5 cm from the end of the inferior border. Then, the trocar was set, and the incision was sutured (Fig. 2b).
Similar to other reports, 10–12 mmHg CO2 was insufflated. Then, along this marker, using 30° laparoscopy, the superficial lymph-fatty tissue was separated along the boundaries from the template-marked skin under fine needle guidance. The dissection was then performed deep to the fascia lata, and the tissue was retrogradely dissected from the peripheral to the central field, so that all the superficial lymphatic tissues could be removed. Medially, the spermatic cord was exposed, and the tissue around it was removed en bloc, then the lymphatic drainage was sutured.
Next, the tissues were divided into two lumps along the saphenous vein, and the branches of the saphenous vein were dissected until the femoral vein was exposed. The deep inguinal lymph node was dissected along the femoral vein up to the femoral ring. The saphenous vein and the branches of the femoral nerve were preserved, as shown in the Supplementary Video (Supplementary Data are available online at
The specimen was removed en bloc through the inferior incision. Then, negative pressure drainage was applied through the medial port until the drainage was less than 10 mL daily for 2 days, and bed rest was required for 3–5 days postoperatively.
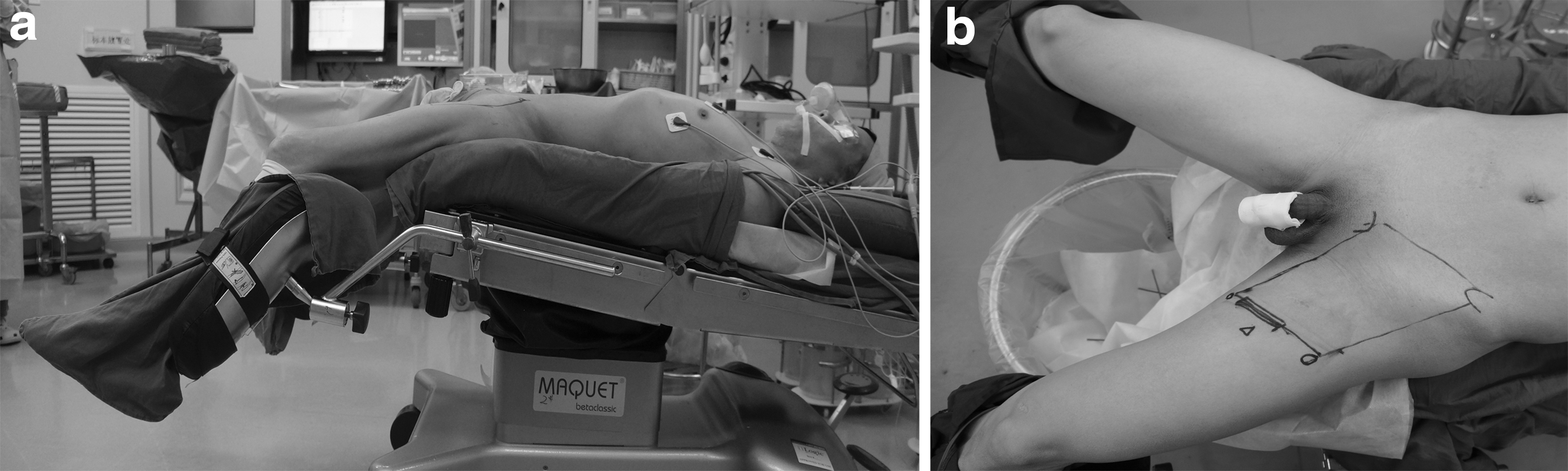
Modified lithotomy position.
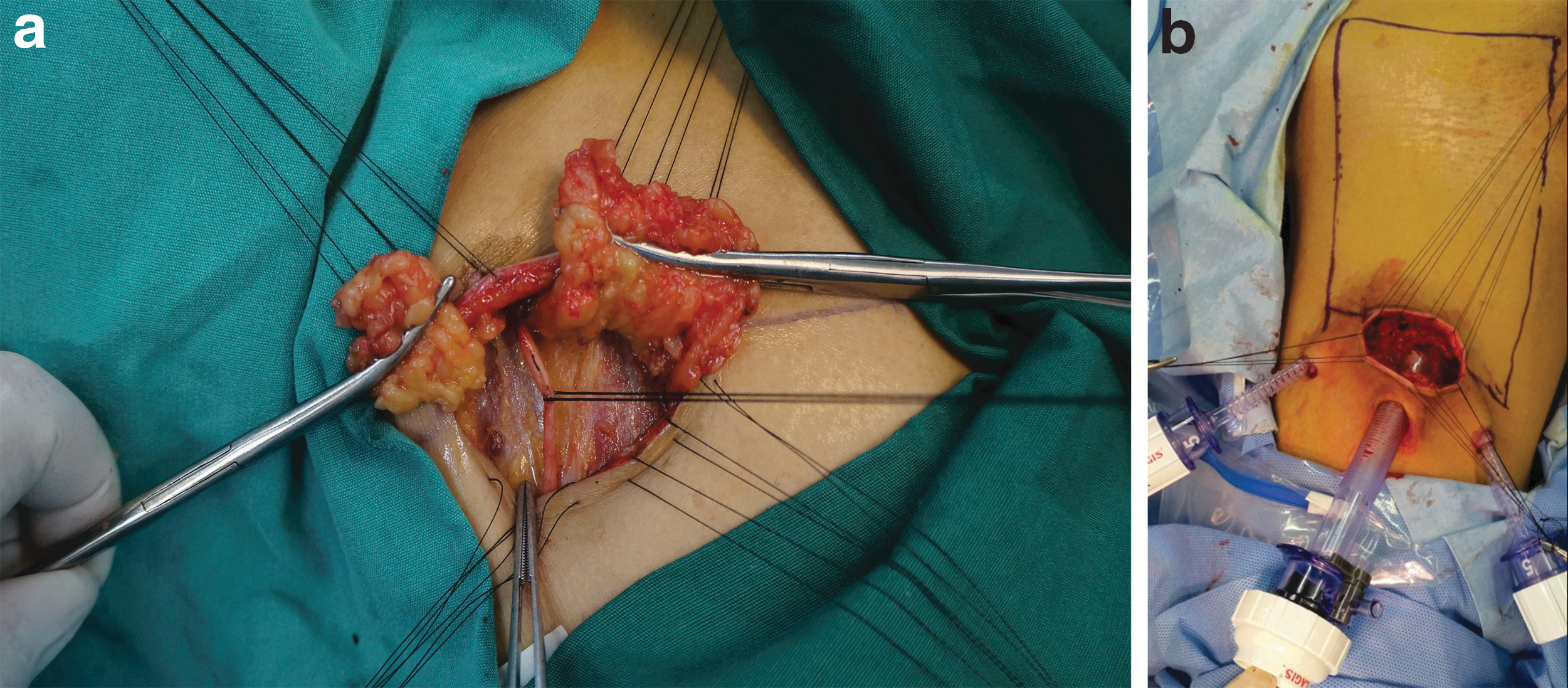
Inferior border incision and initial space of videoscopy.
Antibiotic therapy was performed for 72 hours from 30 minutes before operation, and it would prolong if infection or skin necrosis was detected. Compression stockings were used to prevent deep venous thrombosis and leg lymphedema.
Statistical analysis
Using a binary logistic regression model, propensity score was generated. A matched pair group who underwent bilateral OIL was created in a ratio of 2:1 according to the following parameters: age, body mass index (BMI), and tumor–node–metastasis (TNM) stage, and two groups were matched with similar scores. The numbers of lymph nodes harvested, the numbers of positive lymph nodes, and complications according to the Clavien–Dindo classification were compared between the two groups using t-test, rank sum test, and chi-square test; p < 0.05 was considered significant.
Results
From August 2013 to July 2016, 81 VILs were performed in 48 patients, including 33 patients who underwent bilateral VIL and 15 who underwent left VIL and right OIL. All VIL procedures were performed by two surgeons (Profs. Hui Han and Peng Chen). In addition, between January 2010 and December 2016, 174 bilateral OILs were performed, and the OILs were performed by 3 surgeons (Profs. Hui Han, Fang-Jian Zhou and Kai Yao). The clinical characteristics of these patients who underwent bilateral VILs and OILs are listed in Table 1.
Single lateral.
BMI = body mass index; OIL = open inguinal lymphadenectomy; VIL = videoscopic inguinal lymphadenectomy.
Using match paired analysis, 31 patients who underwent bilateral VIL were matched with 62 patients who underwent bilateral OIL, adjusted to age, BMI, and TNM stage. The other two were not matched effectively. The clinical characteristics of these patients are listed in Table 2. According to the Clavien–Dindo classifications, 8 and 24 limb complications in 5 and 15 patients were observed among the patients who underwent VIL and OIL, respectively (p = 0.08; Table 3). No grade III or IV complications were detected.
Single lateral.
p = 0.08.
In a median follow-up of 22 months (14–47 months), for 31 patients who underwent VIL, 5 patients developed metastasis and died, 1 suffered recurrence in the groin skin, and no inguinal lymph node recurrence was detected. For those matched 62 patients who underwent OIL, 12 patients developed metastasis and 10 of them died.
Discussions
In 2003, Bishoff reported their trial of endoscopic subcutaneous ILD. 11 Then, in 2006, Tobias-Machado and his colleagues first described VIL. In those techniques, the dissections of the superficial and deep lymph nodes were performed in the femoral triangle without the preservation of the long saphenous vein (SV). 6 Specifically, the initial space was created through a mini-incision for the trocar and extended with sharp or blunt separation. The characteristics of these reports are similar, and they demonstrate that VIL was associated with decreased morbidity and comparable oncologic control in short-term follow-ups. 8,9,12 –16
In this study, we found that VIL was associated with less skin-related morbidities, although there was no statistical significance, and the number of lymph nodes was comparable. With modified position, the exposure of full-template (radical) field was feasible, although the operating time was longer. In contrast to radical OIL, we believed that most reported VILs have been performed in the femoral triangle, which might result in residual lymph node tissue. Importantly, in these reports of VIL, conversion to radical ILD was not available for positive lymph nodes. However, in the NCCN guidelines regarding penile cancer, standard ILD is recommended when positive nodes are detected. 17,18 Therefore, we believe that full-template VIL might be more reliable and practical.
In 1988, Catalona proposed that a modified ILD that preserves the SV and leaves the sartorius muscle in place was associated with reduced complications. 19 However, Lopes and colleagues demonstrated that the oncologic outcomes of modified ILDs are not reliable because the lateral area is not dissected. 17,19 Furthermore, in our experience of radical lymphadenectomy, the scope of standard ILD has been reliable in terms of oncologic outcomes. 1,10 Using Single-Photon Emission Computed Tomography (SPECT-CT), Leijte and coworkers demonstrated that sentinel and higher tier nodes were located in the superior and central inguinal zones and that there is lymphatic drainage to the inferior inguinal zones. 20 In addition, Zhu and colleagues found that the medial inguinal package was the first to be involved in the lymph node region. 21 Therefore, the superomedial district is the most common site of inguinal lymph node metastasis. Correspondingly, this district is also the most common location of recurrence when the scope of the OIL is not sufficient, which accords with our experiences. However, the femoral triangle does not include the medial zone next to the spermatic cord or the lateral zone next to the boundary, which may result in inguinal recurrence (Fig. 3).
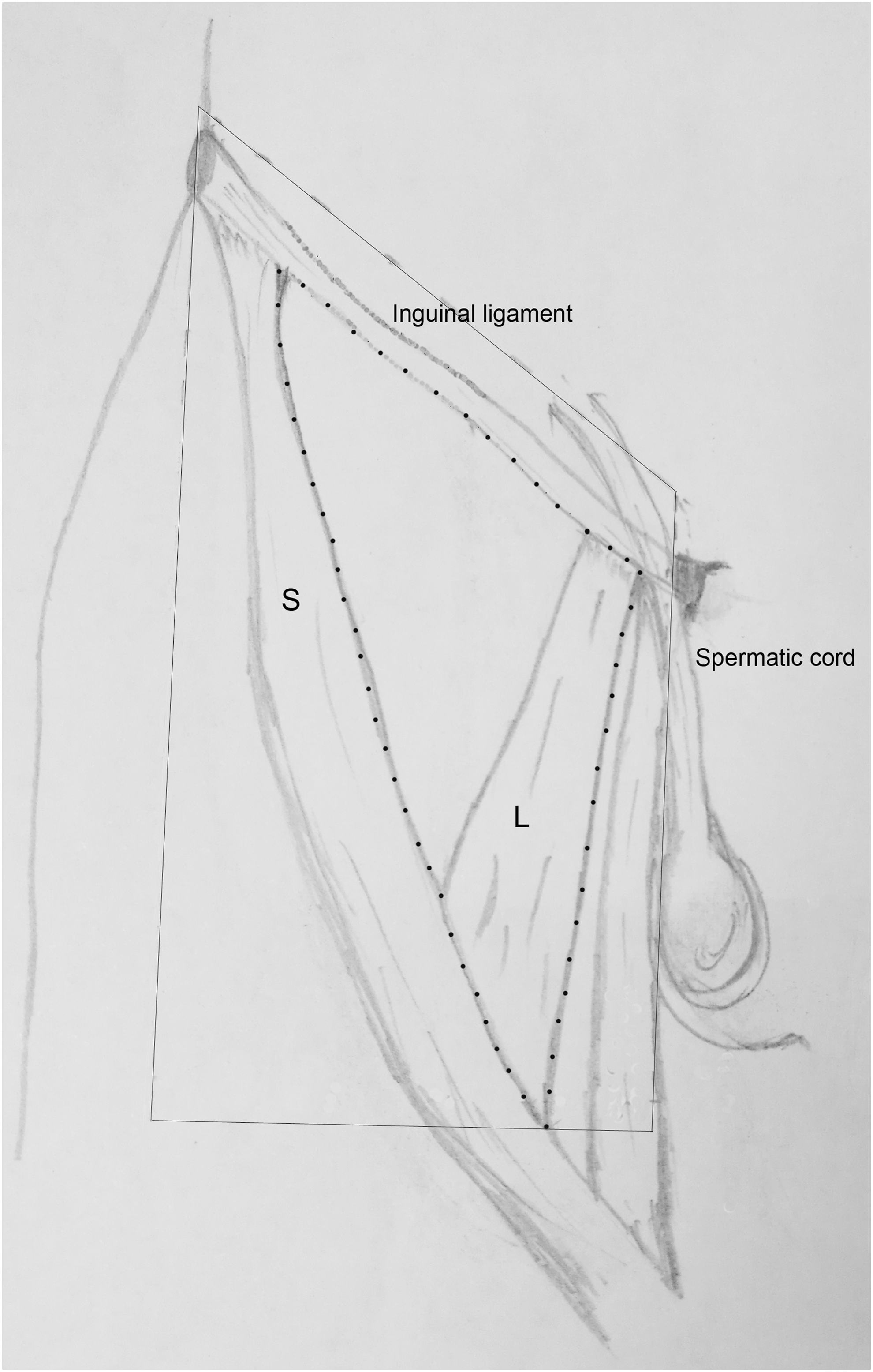
Comparison between full template and formal triangle. L = long adductor muscle; S = sartorius muscle.
Our prior OIL studies revealed that modified radical OIL decreases complications without compromising the oncologic efficacy. 1,10 Moreover, matched-pair analysis revealed that numbers of harvested lymph nodes were comparable between radical VIL and radical OIL; therefore, radical VIL might be more reliable. In the present study, radical VILs were performed in 81 limb areas of 48 patients without conversions to open procedures. The complications were comparable to prior reports of VIL and were better than those of radical OIL. To replicate the radical ILD technique applied through this laparoscopic approach, modifications were made in these aspects.
First, the scope of the radical ILD was precisely achieved through improved positioning and fine-needle penetration guidance. The modified low lithotomy position was required to expose Daseler's area; the boundaries were marked preoperatively and defined with fine-needle penetration intraoperatively. In most recent reports of VIL, the patients have been placed in the supine position with their legs placed on leg spreaders or with thigh abduction. 8,14,22 Although we used this position in our initial experiences, the area above the inguinal ligament and lateral to the spermatic cord was impossible to expose and dissect, because the angle between body and thigh hindered the dissection of the area around the inguinal ligament, especially for right side inguinal dissections. The hindrance caused by the right thigh affected the exposure and dissection of the median tissues and the tissues around the spermatic cord. The drooped leg and externally rotated thigh facilitated the removal of the upper and median tissues, which are important parts of Daseler's field. In brief, the intersection angle between the torso and thigh hindered the exposure of the areas around the inguinal ligament, and the modified position made radical VIL possible and acceptable. The use of “transparent observation” to define the boundaries might have resulted in a bias of ∼2 cm, which is significant and crucial in the dissecting field. 6,8 Using fine-needle guidance, the boundaries were defined accurately during the operation without reducing or enlarging the field.
Second, the clear dissection plane that was created through the 4-cm incision along the inferior boundary ensured en bloc inguinal lymph node dissection. And we were able to identify three useful anatomic markers, that is, the white semihyaline membrane under the superficial layer of Camper's fascia, the fascia lata, and the SV. In our initial two patients following the previous VIL studies (these patients were not included in this study), we found that it was difficult to expose a clear plane with laparoscopic devices through the mini-incision for the trocar and to create the initial space for laparoscopy by blunt separation. As Jacobellis reported, there is a white semihyaline membrane under the superficial layer of Camper's fascia. 4 Master and coworkers also implied that the correct plane was the most crucial aspect of VIL. 8 With the dissection in this definite plane, the vascular supply to the skin was preserved. Moreover, the superficial inguinal lymph node between the membrane and fascia lata was completely dissected.
Based on our OIL experience of more than 200 patients, no loose space is available under the semihyaline membrane. 1,10 If this plane is not clearly defined and sharply dissected during the operation, the skin flap is so thin that necrosis results or so thick that residual lymphatic tissue is left. Therefore, dissecting in the right plane was associated with decreases in morbidity and increases in oncologic efficacy, and the plane and the initial space could be exposed through an inferior incision. In addition, we found that the plane was clearer in the VILs than in the OILs in terms of the amplification effect of laparoscopy, which was useful for protecting the skin and removing the lymph-fat tissue with an ultrasonic knife. Although the incision was as long as 4 cm, it was useful for removing the specimen en bloc.
Through the inferior incision, the SV and fascia lata were exposed and preserved as anatomic markers. Then, VIL was performed along the defined plane, and the tissues between the superficial layer of Camper's fascia and the fascia lata were divided into two parts along the SV from the medial to the lateral region. We believe that the role of the preservation of the SV and fascia lata is related to reducing circulatory system damage and leaving the sartorius muscle. 1,10 Consequently, we harvested 8–32 lymph nodes from each lateral region using VIL, which is more than have been harvested in VIL studies. However, compared to radical OIL, incision-related morbidities were decreased following VIL.
In our radical VIL series, the numbers of harvested lymph nodes were comparable to those harvested in radical OIL cases, and the morbidity of VIL was less compared with OIL. We believe that the high quality of VIL and the decrease in complications presented in this study were related to two modifications: (1) confirmation of the standard dissecting field with a fine-needle marker and improved positioning during the operation and (2) dissection in a definite plane with three anatomic markers, which were exposed through the inferior mini-incision. Moreover, comparisons of the oncologic efficacies and morbidities of VIL and OIL are planned in a future prospective study.
As a retrospective study, this study has certain limitations. The pathologic N status results were different, which might have affected the morbidity of the OIL procedures. Although age, BMI, and TNM stage were matched between the two groups, bias was still present. In addition, the long-term follow-up was inadequate, but the numbers of harvested lymph nodes might indicate quality lymph node dissections. 23 With a median follow-up of 22 months, no recurrence in the inguinal lymph nodes was detected. The groin skin recurrence might have involved the N3 lymph node, which implies that this procedure might not be suitable for N3 patients. And the oncologic outcome between full-template VIL and formal triangle needs advanced investigation.
Conclusions
Modified radical VIL is feasible and practical and results in reduced morbidity, but the oncologic outcomes require further investigation. The dissecting field and the defined plane were critical to these modifications.
Footnotes
Acknowledgments
Ethical approval: This study protocol was approved by the Sun Yat-sen University Cancer Center Ethics Committee (No. 2014-XJS-038), and informed consent was acquired from all patients. Funding: This study was granted by the National natural Science Foundation of China (No. 81722755) and Guangdong science and technology planning project (No. 2015A030302018). Availability of data and materials: The authenticity of this article has been validated by uploading the key raw data onto the Research Data Deposit public platform (
Authors' Contribution
H.H., P.C., Z.-S.L., and F.-J.Z. took a plan and review of this study, and Y.-L. Y., S.-J.G., D.C., Y.-J.W., and K.Y. collected data and wrote this article.
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.