
Abstract
Objective:
To describe population-wide utilization rates and outcomes of percutaneous nephrolithotomy (PCNL) in the management of pediatric upper urinary tract calculi (UUTC).
Patients and Methods:
Patients <18 years with a diagnosis of UUTC, who underwent PCNL between 2001 and 2014 were identified from the National Inpatient Sample database. Annual PCNL rates, based on the at-risk population for each year, were estimated, and change in utilization rate was analyzed using negative binomial regression. Perioperative outcomes, hospital length of stay (LOS), and costs were determined; continuous and categorical variables were analyzed using nonparametric tests and Chi-squared tests, respectively. Trends tests and multivariable analyses (MVAs) were also performed where appropriate.
Results:
An estimated 3206 pediatric PCNL procedures were performed. Mean annual PCNL rate increased significantly relative to 2001 (incidence rate ratio = 1.40; 95% confidence interval 1.15–1.71, p = 0.001). Proportion of PCNL as a fraction of all inpatient surgical procedures for UUTC also significantly increased over time, from 15.7% in 2001 to 26.4% in 2014 (p < 0.0001). Complications overall occurred in 20.7% of cases, with a significantly rising rate over time period (p < 0.0001). Complication rates were similar across hospital types and geographic regions. Median hospitalization cost was significantly higher for the West than for each of the other regions (p < 0.05 in each case). Median LOS was also highest for the West (4 days vs 3 days for each of the other regions). In MVA, significant predictors of both increased LOS and costs included black race, comorbidities of hypertension, diabetes, coagulopathy and neurologic disease, hospitalization in the South, and presence of complications. Race, gender, comorbidities, and treatment year were among the predictors of complications.
Conclusions:
PCNL utilization in the management of pediatric UUTC has significantly increased since 2001, with an associated increase in complication rates, although major complications were uncommon. Regional variations in costs and LOS were evident.
Introduction
A
As technology and technique modifications for pediatric PCNL have evolved, and as the incidence of stone disease in the pediatric population continues to rise, 10 –12 it is of interest to evaluate the current status of PCNL utilization in the management of pediatric nephrolithiasis. Population-wide data on PCNL utilization and outcomes in children are scarce. Using worldwide data from the Clinical Research Office of the Endourologic Society (CROES) registry compiled between 2007 and 2009, Guven et al. 13 examined PCNL outcomes for 107 patients ≤14 years compared with those for 2666 children and adults aged 15 years and older. 13 They observed similar perioperative outcomes for the two groups, but a preference for the use of smaller sheath sizes in the younger patients. In this study, we sought to analyze nationwide trends and outcomes for PCNL in patients <18 years of age with upper urinary tract calculi (UUTC), hospitalized in the United States between 2001 and 2014. We hypothesized that PCNL utilization in children has increased over time.
Methods
Patients and methods
The study was approved by the Rutgers-Robert Wood Johnson Medical School Institutional Review Board. Pediatric patients undergoing PCNL were identified using the National (Nationwide) Inpatient Sample (NIS) databases for 2001–2014. The NIS databases are maintained by the Healthcare Cost and Utilization Project (HCUP), created by the Agency for Healthcare Research and Quality (AHRQ). They contain hospital discharge data from HCUP-participating hospitals. Before 2012, the NIS databases were compiled using data for all discharges selected from a random stratified sample of 20% of HCUP-participating hospitals, whereas from 2012 onward, they incorporated data from a random stratified sample of 20% of discharges across all HCUP-participating hospitals. National estimates are derived using discharge and trend weights provided by AHRQ, which were revised in 2012 for the years 1993–2011, so as to facilitate comparisons to data from 2012 and beyond. The NIS is the largest publicly available, all-payer, database in the United States, with data representative of more than 96% of the U.S. population. Diagnoses and procedures in the NIS are coded using International Classification of Disease, 9th revision, clinical modification (ICD-9-CM) codes.
The study population included patients under the age of 18 years excluding newborns (identified by ICD-9-CM diagnosis codes of V30.0x–V39.0x), with principal or secondary discharge diagnoses of “calculus of kidney or ureter” (ICD-9-CM diagnosis codes 592.0, 592.1, and 592.9), who underwent PCNL during hospitalization (ICD-9-CM procedure codes 55.03 and 55.04). Total number of PCNLs performed during each year was determined, and rate of PCNL utilization was computed by dividing the nationwide estimated procedure count for each year by the total U.S. pediatric population for the corresponding year. Population data were obtained from the U.S. Census Bureau estimates. 14
Data on patient demographics, insurance status, hospital length of stay (LOS), perioperative complications, and hospitalization costs were abstracted. The NIS database contains data on hospital charges for each discharge. Hospitalization costs were estimated by multiplying hospitalization charges by Cost-to-Charge ratio files available through HCUP, and adjusted by inflation to the year 2014. Categorical variables were analyzed using Chi-squared tests, while continuous variables were tested for normality of distribution and analyzed using t-tests or Wilcoxon rank sum tests as appropriate. Change in proportions over time was analyzed using the Cochran–Armitage trend s test. Multivariable analysis (MVA) with control for patient demographic characteristics, comorbidities, insurance status, and hospital characteristics was performed to estimate predictors of PCNL, complications, total hospital costs, and LOS. Negative binomial regression using procedure count as the dependent variable, calendar year as the independent variable, and the natural log of the pediatric population for each year as the offset term, was used to analyze annual rates of PCNL utilization. A p-value <0.05 was considered statistically significant in each case. Statistical analysis was performed using SAS statistical software, version 9.4 (SAS Institute, Cary, NC), and Stata® version 15 statistical software (StataCorp LP, College Station, TX).
Results
PCNL utilization
Over the study period, an estimated 3206 (standard deviation 260) pediatric PCNL procedures were performed across the United States, representing 20.7% of all inpatient surgical procedures for UUTC (n = 15,463). Relative to 2001, overall annual PCNL rate for 2002–2014 was 3.2 per million, compared with 2.3 per million for 2001 (incidence rate ratio [IRR] = 1.40; 95% confidence interval [CI] 1.15–1.71, p = 0.001) (Fig. 1). By subgroups of age, PCNL utilization rate relative to 2001 significantly increased for 5–9 and 15–17 year olds (IRR 2.02; 95% CI 1.18–3.46; p = 0.01 and IRR 1.94; 95% CI 1.38–2.73; p < 0.001, respectively). The utilization rate decreased for those <5 years (IRR 0.61; 95% CI 0.37–1.0; p = 0.048), and remained unchanged for the 10- to 14-year age group (IRR 1.27; 95% CI 0.89–1.81; p = 0.19).
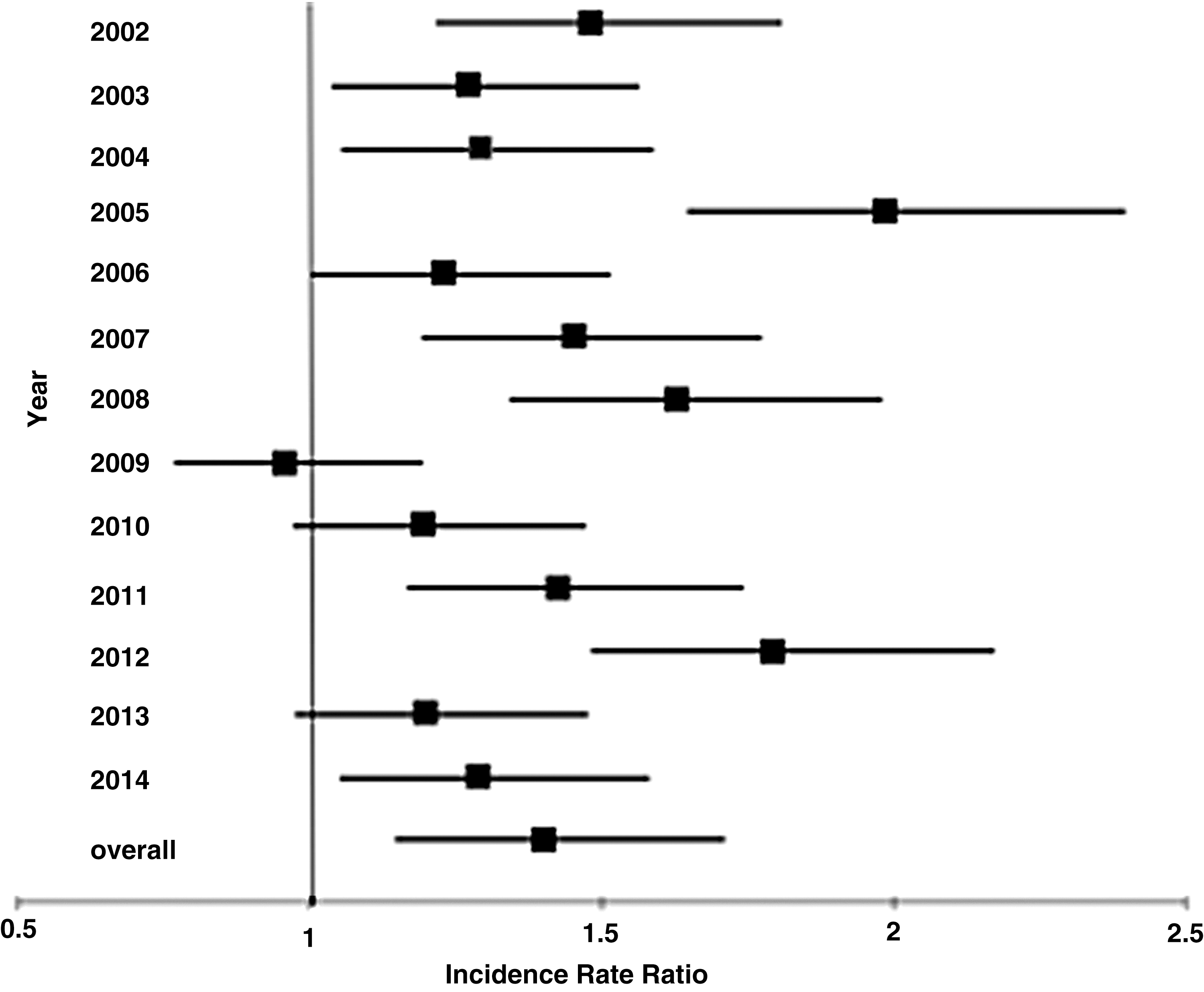
The vertical line at 1 represents the referent year (2001). Data points and bars respectively represent IRRs and 95% confidence intervals for each year relative to 2001, and the overall IRR. IRRs = incident rate ratios.
Proportion of PCNL as a fraction of all inpatient surgical procedures for UUTC also significantly increased over time, from 15.7% in 2001 to 26.4% in 2014 (p < 0.0001); this increase was observed for the overall cohort and for each age subgroup.
Overall, 41.6% of the PCNLs were performed in 15–17 year olds, 53.8% in girls and 53.2% in whites. A majority of PCNLs (63.8%) were completed in the Midwest and South, while 86.9% were performed in urban teaching hospitals (Table 1).
PCNL = percutaneous nephrolithotomy; UUTC = upper urinary tract calculi.
Inpatient outcomes
For the overall cohort, median (interquartile range [IQR]) LOS was 3 (2, 5) days. Overall LOS did not significantly vary by age, gender, or hospital type, but significantly varied according to race/ethnicity (p = 0.0004) and hospital region (p = 0.006). Blacks had a median LOS of 6 days (IQR 3, 9), which was significantly longer than that for whites (3 days [IQR 2, 5]; p = 0.0005) or Hispanics (4 days [IQR 2, 5]; p = 0.04). Median LOS for the West (4 days [IQR 2, 5.5]) was higher than for each of the other regions (3 days each [IQRs 2, 4–2, 5]), but on pairwise comparisons, this difference achieved statistical significance only with comparison to the Midwest (p = 0.004).
Complications occurred in 20.7% of cases (665 of 3206). Complication rates over the study interval are shown in Figure 2. Although there was fluctuation in the observed rates, there was an overall increase in the frequency of PCNL complications between 2001 and 2014 (p < 0.0001). On subset analysis, rates for overall infectious complications were observed to significantly increase over time, from 8.8% in 2001 to 20.9% in 2014 (p = 0.0008), while rates for other complication types were insufficiently large to conduct an accurate trend analysis. Complication rates significantly varied according to age (p = 0.037), gender (p = 0.0002), and race/ethnicity (p = 0.01). Complication rates were statistically similar across geographic regions and hospital types (p > 0.05 in each case). Infectious complications overall were the most common (12.9%), including urinary tract infection (UTI) in 320 (10.0%) and sepsis in 124 cases (3.9%). Hydrothorax, venous thrombosis, and persistent urinary fistula were not observed. Inpatient mortality rate was 0.16% (5 of 3206) (Table 2); interestingly, inpatient mortality after PCNL was observed only in 2010.
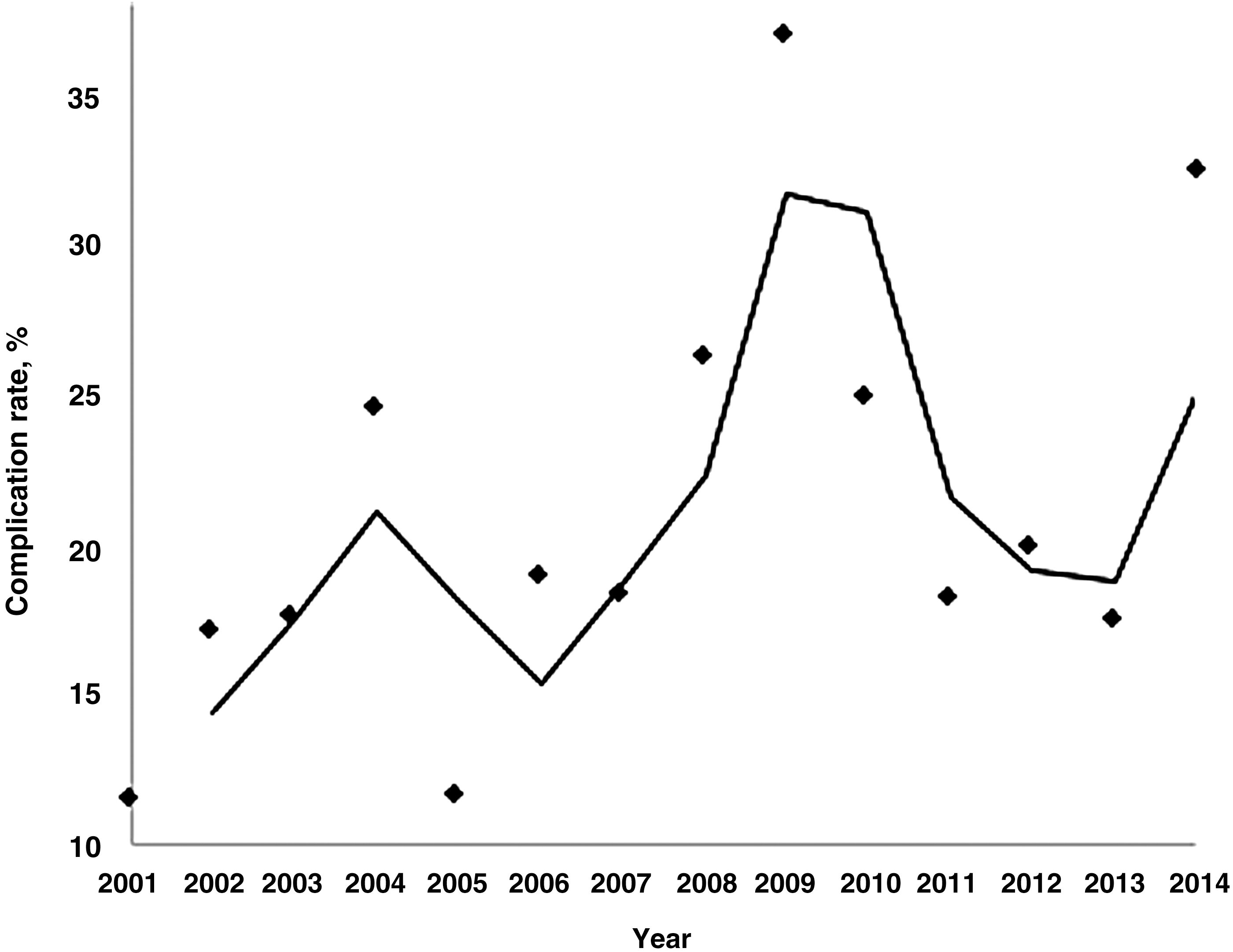
Trend in complication rates is shown using a moving average trend line whereby each point on the line represents the average complication rate for two consecutive years.
UTI = urinary tract infection.
Costs
Median (IQR) overall cost per hospitalization for pediatric PCNL was $12,494 ($8,365–$18,411). Median hospitalization cost did not significantly vary by age, gender, or teaching hospital status, but varied significantly by race, hospital region, and presence of complications (Table 3).
Multivariable analysis
On multivariate analysis, significant predictors of both increased LOS and costs included black race, comorbidities of hypertension, diabetes, coagulopathy and neurologic disease, hospitalization in the South, and presence of complications. Neurologic diseases included paralysis, seizure disorders, movement disorders, dystonias, and others. Significant predictors of complications included female gender, race/ethnicity, comorbidities of coagulopathy, neurologic disease and chronic lung disease, and having Medicaid insurance (Table 4).
Only statistically significant associations are displayed.
CHF = congestive heart failure; DM = diabetes mellitus; HTN = hypertension; LOS = length of stay.
Discussion
Several studies have documented sharp increases in the incidence and prevalence of urolithiasis in children in recent decades. 10 –12 Parallel with this has been an increase in the number of surgical interventions for stone disease in the pediatric population. 15 In patients with large stone burdens or possessing unfavorable anatomy, PCNL has largely replaced open surgery in adults and children, and its utilization in adult stone formers has expanded over time. 16,17 However, its potential for significant morbidity contributed to its slower adoption in pediatric patients. To our knowledge, we present the first population-based study of PCNL trends and outcomes in pediatric patients in the United States. We demonstrated a significant overall increase in the rate of PCNL use between 2001 and 2014. Several factors could certainly be responsible for driving this trend, including but not limited to increasing size and complexity of stone burden in the pediatric population, increased training of pediatric urologic subspecialists skilled with managing complex pediatric stone disease, and technological improvements in PCNL equipment that have enhanced its safety, thereby facilitating its increased utilization in younger children. The specific driving factors cannot be gleaned from out dataset given that it lacks granular clinical information, but these findings open avenues for further investigation. Indeed, recent evidence points toward a preference for use of smaller tract sizes and smaller nephroscopes in younger children, supporting the idea that technological improvements may have partly contributed to increased implementation of PCNL in children. 13
An interesting finding in our study was that complication rates following pediatric PCNL significantly increased between 2001 and 2014. This mirrors trend in PCNL complications in adults. 18 The overall complication rate in our study was 20.7%, mirroring that reported in previous studies in both adults. 19,20 and children. 21 Serious complications including hemorrhage (2.3%), sepsis (3.9%), respiratory complications (2.2%), and renal complications (0.9%) were rare, while UTI was relatively more frequent (10%). This finding is also in line with outcomes observed in large case series of pediatric PCNL, in which the vast majority of complications were Grade I or II complications. 21 –23 However, factors underlying the rise in the rate of complications over time are less clear. One possible explanation could be an increase in the number of patients with more complex stone burdens being offered PCNL as provider experience grows. Another possibility is that even among those with large stone burdens, PCNL is offered only for the most complex of cases, as select patients with large renal stone burdens can also be eligible for retrograde intrarenal surgery. 24 On MVA, we observed that comorbidities of neurological disease, coagulopathy, and chronic lung disease among others were significant predictors of a higher complication risk. Furthermore, among pediatric patients with UUTC who underwent surgical intervention, comorbidities of renal failure and neurologic disorders were found to be more common in the PCNL cohort (data not shown), lending support to the idea that performing PCNL in sicker patients raises the risk of complications. Additionally, performing PCNL in patients with greater stone complexity has been associated with higher rates of complications. 13,16,21
Although 87% of pediatric PCNL cases were performed at urban teaching hospitals and in the South, we observed that complication rates did not significantly differ according to hospital type or geographic region. A possible explanation is that the more complex cases were referred to the larger urban teaching hospitals where outcomes matched those for smaller hospitals with less complex cases. Data from CROES have indeed demonstrated that PCNL complication rates are lower in high volume centers. 25
Median cost of pediatric PCNL hospitalization was highest for the West and lowest for the Northeast, on both univariate and multivariate analysis. Using data from the Premier Healthcare Database, Leow et al. 26 also demonstrated that hospitalization in the West was a significant predictor of higher 90-day hospital costs following PCNL when compared with the Midwest or Northeast. Taken collectively, these studies reveal that costs of PCNL hospitalization are highest for the West, while our data additionally suggest that this cannot be explained by differences in complication rates, which were statistically similar across the different regions. Regional differences in patient comorbidities that may affect hospitalization acuity, and regional differences in hospital resource utilization are possible drivers of these cost variations, and further studies are needed to explore this further. These findings could have implications in shaping future health policy initiatives.
Our study is not without its limitations. First, given that the NIS database contains only administrative variables, we were unable to analyze clinical information such as stone size, location and complexity, or percutaneous tract size. We believe for example that smaller sheath sizes are generally favored during pediatric PCNL, although there is some variation according to the provider. Future large-scale studies with access to clinical data, such as from a nationwide registry, could be of value in obtaining more in-depth insights about variations in surgical technique and related patient-specific outcomes. Second, given the lack of patient identifiers in the NIS database, we are unable to determine which patients may have undergone repeat procedures vs the number of new patients with stone characteristics favoring selection of PCNL. However, given that our purpose was to study the overall rates of PCNL utilization in the pediatric cohort and its associated outcomes, we believe that the impact of this limitation on our reported findings is minimal. Third, coding errors in the database could have affected our estimates, but we believe that the true estimates likely fall within the reported CIs, and that evaluating the nationwide data over several years provides useful information on current trends. Finally, conclusions based on the NIS dataset are limited to perioperative outcomes only, and therefore complications that resulted in unplanned emergency room visits or hospital readmissions may not have been captured leading to an underestimation.
Conclusions
The rate of utilization of PCNL in the management of pediatric nephrolithiasis in the United States has significantly increased since 2001. Perioperative complications rates have also increased over time, but serious complications are uncommon. Pediatric PCNL hospitalization costs vary significantly according to region, with the highest costs in the West and the lowest costs in Northeast, likely reflecting differences in patient characteristics and/or resource utilization. Future studies re-examining these trends using patient-specific clinical information would be informative in better understanding the evolution of the technique and associated clinical outcomes.
Footnotes
Author Disclosure Statement
No competing financial interests exist.