
Abstract
Background and Aims:
Procedures for urolithiasis are a core part of the development for the urologist in training. Understanding the learning curve of the procedures is important, allowing for planning in the training and assessment of trainees. The aim of this study was to systematically review the literature pertaining to learning curves in urolithiasis surgery.
Materials and Methods:
The review was registered on the PROSPERO database and conducted in keeping with the Preferred Reporting Items for Systematic reviews and Meta-Analysis statement. Embase, MEDLINE, and PsycINFO were systematically searched from inception to January 2018, with a reference review conducted. All empirical studies on learning curves in urolithiasis surgery were included irrespective of procedure. Articles describing pediatric surgery, nontechnical skills in surgery, or those not written in English were excluded.
Results:
Of 390 articles identified from screening, a final 18 studies were included. Fourteen studies identified the learning curve in percutaneous nephrolithotomy. These studies identified a learning curve of between 30 and 60 cases for both operative time (OT) and complication rates. Four articles focused on flexible ureteroscopy (FURS); the learning curve for FURS has been outlined as 60 cases for OT and 56 cases for fragmentation efficacy.
Conclusions:
The complexities of determining learning curves are extensive; studies use different parameters to measure outcomes and observe skill acquisition rates of surgeons with differing prior experience. Evidence in this article can guide trainee urologists with regard to the expected rate of progress. Multi-operator multicenter research utilizing standard outcome measures should be conducted to establish definitive learning curves.
Introduction
L
The first description of the learning curve was provided in 1885 by Ebbinghaus and related to the psychology of learning. 3 Since then, the concept of learning curves has been used predominantly in the aviation industry 4 and in recent years has begun to filter into the surgical field. The importance of learning curves in the clinical setting has only become more apparent since the 2001 inquiry into mortality after cardiac surgery in the Bristol Pediatric Surgical Unit, which concluded that to improve outcomes, patients should be spared exposure to the beginning of a surgeon's learning curve. 5
Urology is a rapidly progressing field with operative techniques and technologies continually evolving. Despite many changes in this arena, urolithiasis procedures remain a key group of operations urologists are required to master during their training. The learning curve of a urological procedure is the time a surgeon finds the process more difficult; subsequently, the operation may take longer and be associated with lower efficacy and higher complication rates. 6
Since the introduction of the European Working Time Directive in 2003, 7 there is an increasing demand for focus on surgical competence through means such as learning curve identification. As urolithiasis is such a common and important area of urology, it is essential to determine a learning curve for each technique. This would enable assessment of the progress of a surgeon in training, ensuring competence in each component of the procedure. Additionally, enhanced understanding of the rate of skill acquisition during training can aid the development of effective procedure-specific training programs.
Therefore, this study aims to systematically review the literature on learning curves in urolithiasis surgery procedures using multiple outcome measures.
Materials and Methods
A search protocol for learning curves in various urolithiasis procedures was developed in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analysis statement. 8 The protocol was registered with the PROSPERO database (ID no.: CRD42018085022). 9
Information sources and search
The MEDLINE, Embase, and PsycINFO databases were systematically searched from inception to January 2018.
Search terms included “learning curves” or “learning effects” or “curve analysis” or “skill acquisition” and “urolithiasis.” A further procedure-specific search was conducted, including “urolithotomy,” “lithotomy,” “extracorporeal shockwave lithotripsy,” “percutaneous nephrolithotomy,” “ureteroscopy,” “ureterorenoscopic lithotripsy,” “renal calculi surgery,” and “ureteric calculi surgery” combined with the keywords relating to learning curves.
A subsequent reference review was conducted, and the Cochrane Library database was reviewed. A search for preprint articles was conducted through OpenGrey, and ongoing studies were identified through the ISRCTN database. Where texts were unavailable or more information was required, the authors were contacted directly.
Study eligibility criteria
All empirical studies pertaining to learning curves in urolithiasis surgery were included irrespective of procedure or whether they were conducted prospectively or retrospectively. Abstracts from conferences were included if sufficient information could be extracted.
Articles describing pediatric surgery, nontechnical skills in surgery, or those not written in English were excluded.
Study selection
Two reviewers independently identified potentially relevant articles. After meeting the inclusion criteria, duplicates were removed, and the titles and abstracts of studies were reviewed. The full text of each article was reviewed and excluded if not relevant to learning curves in urolithiasis procedures. Articles pertaining the learning curves in percutaneous nephrolithotomy (PCNL) and flexible ureteroscopy (FURS) were found. All citations were transferred to referencing software (Mendeley 2018; Elsevier, London, United Kingdom).
Data collection and data items
Studies were grouped according to the procedure they are related to. The characteristics and results of each study were tabulated using an electronic data collection program (Microsoft Excel 2016, Redmond, WA).
The characteristics noted for each study included the authors, year of study, type of procedure, study design, number of surgeons observed, and number of cases performed. The previous experience of surgeons in PCNL was noted. It was also recorded if the novice was supervised by a mentor or if the performance of the novice was compared with an expert.
All outcome measures identified in the articles that are related to learning curves were extracted; the variables can be categorized into patient safety measures and operative efficacy and efficiency measures.
Patient safety measures included: Radiation dose Blood transfusion rates Estimated blood loss Complications Length of hospital stay (LOS) Retreatment rate
Operative efficacy and efficiency measures encompassed: Operative time (OT) Fluoroscopic screening time (FST) Puncture time and success rate Stone-free rate (SFR)
Data regarding the method used by each article to draw conclusions regarding learning curves were also extracted.
Results
Study selection
A total of 390 potentially relevant studies were discovered. After deduplication, plus title, and abstract review, the full text of 33 articles was screened. Eighteen studies satisfied inclusion and exclusion criteria (Fig. 1); these articles focused on the learning curve in either PCNL or FURS. No articles were found pertaining to the learning curve in other urolithiasis techniques.
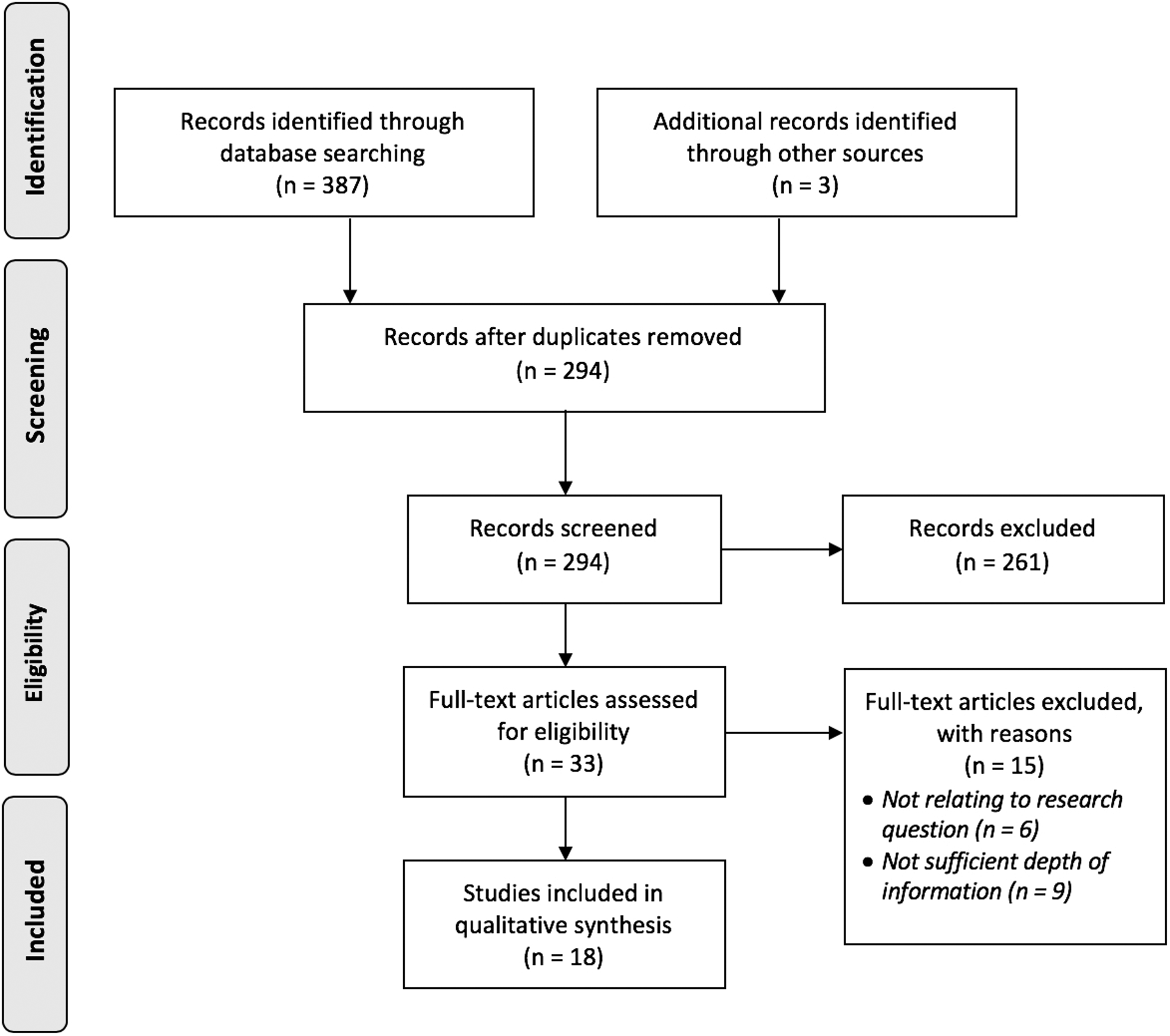
Study selection process according to the Preferred Reporting Items for Systematic reviews and Meta-Analysis.
Study characteristics and results synthesis
Selected articles consisted of case series assessing the learning curves in PCNL or FURS. Results were classified by procedure and further subdivided by outcome measure.
Percutaneous nephrolithotomy
In total, 14 studies described the learning curve of PCNL; the design and characteristics of these studies are summarized in Table 1. All studies examined were case series so level IV evidence. 10
Design and Characteristics of Percutaneous Nephrolithotomy Studies
A = abstract; ANOVA = analysis of variance; FST = fluoroscopic screening time; Hb = hemoglobin; LOS = length of hospital stay; MIP = minimally invasive percutaneous nephrolithotomy; NR = not reported; OT = operative time; SFR = stone-free rate; US = ultrasound.
A large proportion of the studies were prospective case series (10/18). Five studies focused on the learning curve of gaining access in PCNL, two observed the learning curve specifically in minimally invasive percutaneous nephrolithotomy (MIP), two related to supine PCNL, and the rest focused on “standard” prone PCNL.
The number of surgeons observed in these studies ranged from 1 to 8, with half observing a single operator. Most of the studies examined the learning curve of surgeons who had previous endourological experience but were considered novices in PCNL. The majority of studies observed surgeons at a single center; only one publication was a multicentered observation. The number of patients included in the individual studies ranged from 53 to 248, with 1739 in total.
There was no uniformity in the criteria for surgeons to be considered a novice in the studies. All surgeons had received prior endourological training, but the extent of this was not discussed in most articles; in the studies where this was included, experience varied from 1 11 to 6 years. 12
Six studies provided mentor supervision to the trainees, and in only one study, the mentor was present throughout all procedures. Interestingly, only six of the studies compared the results of novices with that of experts in PCNL.
If outcome measures observed in studies were comparable, they were summarized. When possible, the “novice” and “expert” results were compared. Novice referred to surgeons embarking on the learning curve, and experts were those deemed to have completed the curve.
Operative efficacy measures
Operative time
The OT was observed in 11 studies 11 –21 ; the learning curve for the length of procedure was identified between 30 and 60 cases (Table 2).
Outcome Measures in Percutaneous Nephrolithotomy Studies with Corresponding Number of Cases Required to Complete Learning Curve
— = Learning curve of this outcome measure not commented on in study; A = abstract; C = competence; E = excellence; NSD = no significant difference in outcome measure observed between the start and the end of study.
OT consistently plateaued after 60 procedures in 4 articles. 11 –13,18 An article by Jessen and colleagues 18 looked at the first 75 consecutive PCNL access procedures of a novice; they concluded that a surgeon was required to conduct between 30 and 40 cases to complete the learning curve in relation to SFR, complications, and rate of retreatment. The OT, however, continued to decrease after this number; therefore, the study indicated that competence could be achieved after 30 to 40 cases. Excellence plateaued in OT after 60 to 80 PCNLs.
Garg and colleagues 20 carried out a particularly well-designed retrospective study focusing on the learning curves of eight trainees. This was the only study that focused on outcome measures in relation to stone complexity. They concluded that completion of the learning curve occurred after 30 to 35 cases; however, this only applied to OT when accessing stones of grade I complexity. The surgeons in this study had previously performed 50 to 70 percutaneous nephrostomies, which the authors attributed to the shortened learning curve.
Another article determined that the OT of two novice surgeons reached that of an expert after 30 cases; however, both trainees had completed a modular training scheme before commencing PCNLs. 19
Of the 11 studies observing OT, 6 compared the OT of novice surgeons with that of a surgeon deemed a PCNL expert. 11,13,17 –20 All six of these articles noted that the expert group had a shorter OT.
Fluoroscopic screening time
FST was observed in 6 studies, 12,13,17,20,22,23 with the number of cases required to reach a plateau in screening time ranging from 20 to 115 (Table 2).
Allen and colleagues 13 compared 155 PCNLs of a novice in groups of 15 cases. At the outset, FST was 9.93 minutes, which decreased to a minimum of 3.85 minutes by cases 100 to 115, which was comparable to a senior surgeon. Negrete-Pulido and colleagues 22 observed FST in 82 procedures carried out by an endourology fellow, noting a significant decrease from 4.73 minutes in the initial 20 cases compared with 2.03 minutes after 40 punctures when a plateau in the graph was reached. A similar study by Tanriverdi and colleagues 12 observed a peak in FST (17.58 minutes) in the first 15 cases, a decrease in FST was noted for 46th to 60th case (8.92 minutes); after this point, the FST continued to decrease but no longer significantly. Schilling and coworkers 17 conducted a retrospective study comparing the FST of an expert and novice carrying out MIPs during a 1-year period. At the start of the year, the FST for the novice and expert was significantly different, 4.6 and 2.8 minutes, respectively. The FST of the novice decreased throughout the year; however, this was not statistically significant, and the learning curve did not reach a plateau. In 2016, Usawachintachit and coworkers 23 compared the FST of 100 consecutive ultrasound-guided prone PCNLs carried out by an experienced PCNL surgeon. The article concluded that the learning curve for FST, puncture time, and radiation dose was complete after 20 cases; the short curve is attributed to prior surgeon experience. The screening time was compared between experts and novices in three articles 13,17,19 ; each study observed a shorter FST for the more experienced surgeon.
Stone-free rate and extraction percentage
SFR was an outcome measure reported in 10 articles ranging from 30 to 105 cases required to achieve competence (Table 2).
A number of the studies found that there was no significant difference in the SFR achieved by novices in initial procedures compared with their subsequent cases or the SFR of experts. 11,12,16,19,23 Ziaee and coworkers observed that 105 consecutive procedures split into groups of 15 cases; the mean stone extraction percentage increased from 88.3% in the first 15 cases to 99.3% in the 99th to 105th procedure. This study also found that the amount of residual stone plateaued between 99 and 105 cases. A study of 240 ultrasound-guided PCNLs performed by a surgeon found that the SFR significantly increased with experience reaching 90% for the 121st to the 180th patient. 24 A conference abstract by Bucuras and coworkers 15 observed 149 supine PCNLs to establish the learning curve for this procedure variation. They noted the difference in OT, LOS, SFR, and complications between the first 40 and last 40 cases, and the established supine PCNL was safe after 40 cases.
Puncture time and success rate
A number of studies observed the puncture success rate 18,22 –24 (Table 2). Yu and associates 24 observed the longest learning curve with regard to puncture success, noting that the curve did not flatten until the trainee had completed 120 cases.
Negrete-Pulido and associates 22 observed that the relative frequency of puncture success did not reach an acceptable level until the surgeon had completed 50 punctures. The same article noted a decrease in puncture time from 7.67 minutes in the first 20 cases to 4.69 minutes at the end of this study; however, a plateau in the learning curve was not observed.
An observation of learning curves in percutaneous access using ultrasound and fluoroscopy by Jessen and associates 18 found a relatively short curve of less than 30 cases for puncture success rate. In this study, after 30 cases, the trainee no longer required assistance from the senior surgeon and was able to perform punctures alone with similar success rates to that of the expert.
Patient safety measures
Blood loss and transfusion rate
Multiple studies investigating the learning curves associated with PCNL looked at outcome measures, such as blood loss, 12,14 blood transfusion rates, 12,14,23 and change in the patients preoperative and postoperative hemoglobin levels. 12,16,19,21 None of the studies was able to find a significant difference in these measures as the novice progressed, as a result a learning curve could not be described for these factors (Table 2).
Radiation dose
Radiation dose was used as an outcome measure for the learning curve in two studies. Allen and associates found that competence was achieved after 115 cases by which time the radiation dose had decreased to an average of 406 cGy/cm 2 in comparison to 1440 cGy/cm 2 at the beginning. 13 Usawachintachit and coworkers demonstrated a very different result when observing radiation dose in percutaneous access concluding that only 20 cases were required to obtain a significantly decreased level of exposure. 23
Complications
Although complications were measured in 11 of the 14 studies, 11,14 –16,18 –24 often these were measured using different parameters to classify complications therefore not statistically comparable.
A recent study by Yu and coworkers observed no cases of access-related injury to organs and three cases of perforation during dilatation, these all occurred in the first 60 cases. 24
A single study in 2010 noted no major complications, finding that minor injuries only occurred within the first 45 cases, indicating completion of the learning curve after that number of procedures. 14
Although Garg and coworkers 20 described the surgeon reaching a plateau of the learning curve in relation to complications, the article did not state the number of cases required to reach this stage.
Of the 11 studies, 6 indicated no statistical difference in the complication rates of the trainees in their early or late cases or indeed in comparison to the rates of experienced surgeons. 11,16,19,21 –23
Length of hospital stay
Despite LOS being one of the most frequently measured factors (Table 2), only one article described a reduction in LOS between the novices earlier and later procedures, a specific number of procedures required to complete the curve were not noted. 21
Retreatment rate
One of the studies investigating retreatment rates among patients found that an operator was required to complete 30 to 40 PCNLs before a decrease in this outcome was recognized. 18 The other two studies observing retreatment failed to establish a difference in retreatment rate between early and late cases by a novice surgeon. 16,19
Ureteroscopy
Overall, four studies were found to evaluate the learning curve in FURS; there were no articles pertaining to rigid ureteroscopy (URS). The studies were considered level IV evidence as they were all case series. A summary of the design and characteristics of these articles can be found in Table 3.
Design and Characteristics of Ureteroscopy Studies
A = abstract; CUSUM = cumulative sum; FURS = flexible ureteroscopy; URS = ureteroscopy.
All were retrospective case studies and conducted in single institutions. Most of these studies focused on an individual surgeon's experience. The subjects had varying levels of expertise, ranging from novice to those having carried out multiple URSs. The number of patients included in the articles ranged from 43 to 219, with a total of 442 participants.
The outcomes measures monitored when observing the learning curve included: OT, SFR, fragmentation efficacy, complications, and qualitative measures (tissue management, bimanual dexterity, autonomy, depth perception, and efficiency).
Operative efficacy measures
OT was a measured by two studies focusing on FURS (Table 4). The OT was observed by Cho and colleagues in 100 consecutive cases by a single surgeon. Interestingly, they noted a significant increase in the length of operation after the first 60 cases. 25 The increase in OT was found to correlate with increasing stone volume and size; the learning curve for OT could not be established in this article. The cases were then assessed in sets of 10 for change in fragmentation efficacy as the surgeon became more experienced. Fragmentation efficiency was calculated through the “removed stone volume (in cubic millimeters)” divided by the “operative time (in minutes).” No further increase in fragmentation efficacy was noted between 51 and 60 cases or after this set. These results were further analyzed using cumulative sum analysis; this change point analysis enabled the identification of the 56th case as the point at which the curve plateaued. Cho and colleagues were the only group to study SFR and noted no significant change over the 100 cases. 25
Outcome Measures in Ureteroscopy Studies with Corresponding Number of Cases Required to Complete Learning Curve
— = Learning curve of this outcome measure not commented on in study; A = abstract; C = competence; E = excellence.
The 2016 conference abstract by Da Cruz and colleagues observed the first 80 FURSs by a trainee surgeon. Comparison of OT found no further significant decrease after the first 60 cases. 26 This study also observed a variety of qualitative measures including tissue management, bimanual dexterity, depth perception, autonomy, and efficiency; in these fields, no significant change was noted after group 3 (cases 41–60), and so, they concluded the learning curve was complete after 60 cases.
Patient safety measures
Complications were the only patient safety measure observed relating to learning curves in FURS. A retrospective study of 219 patients by Komori and coworkers 27 in a high-volume center observed complication rates. The rate of complications of a novice in FURS before training and in the first 100 cases after training was compared with that of an expert surgeon. Although the incidence of urosepsis as a complication did not decrease, the rate of all other severe complications decreased with experience, indicating that the learning curve was complete at 100 cases.
Discussion
This systematic review has identified the current evidence base for the learning curves in urolithiasis surgery. A 2013 systematic review of learning curves in urological procedures 1 found six articles pertaining to learning curves in PCNL. The present study is the first to provide a comprehensive review of the learning curves in urolithiasis surgery and includes an additional eight PCNL studies.
The most widely investigated surgical modality was PCNL with the number of cases required to attain competence for this procedure being dependent on the type of PCNL conducted and the outcome measure utilized to measure competence (Fig. 2). For prone PCNL, the learning curve varied greatly depending on outcome measure and was demonstrated to be complete after 30 to 60 cases when observing OT, 30 to 115 cases for FST, and after 105 cases for acceptable SFR to be achieved. When focusing on gaining access to the kidney in PCNL, studies identified a learning curve for the length of operation to be completed after 60 cases, with FST reaching an acceptable level between 20 and 40 procedures. With regard to PCNLs performed with the patient in a supine position, the OT reaches acceptable length after 36 cases.
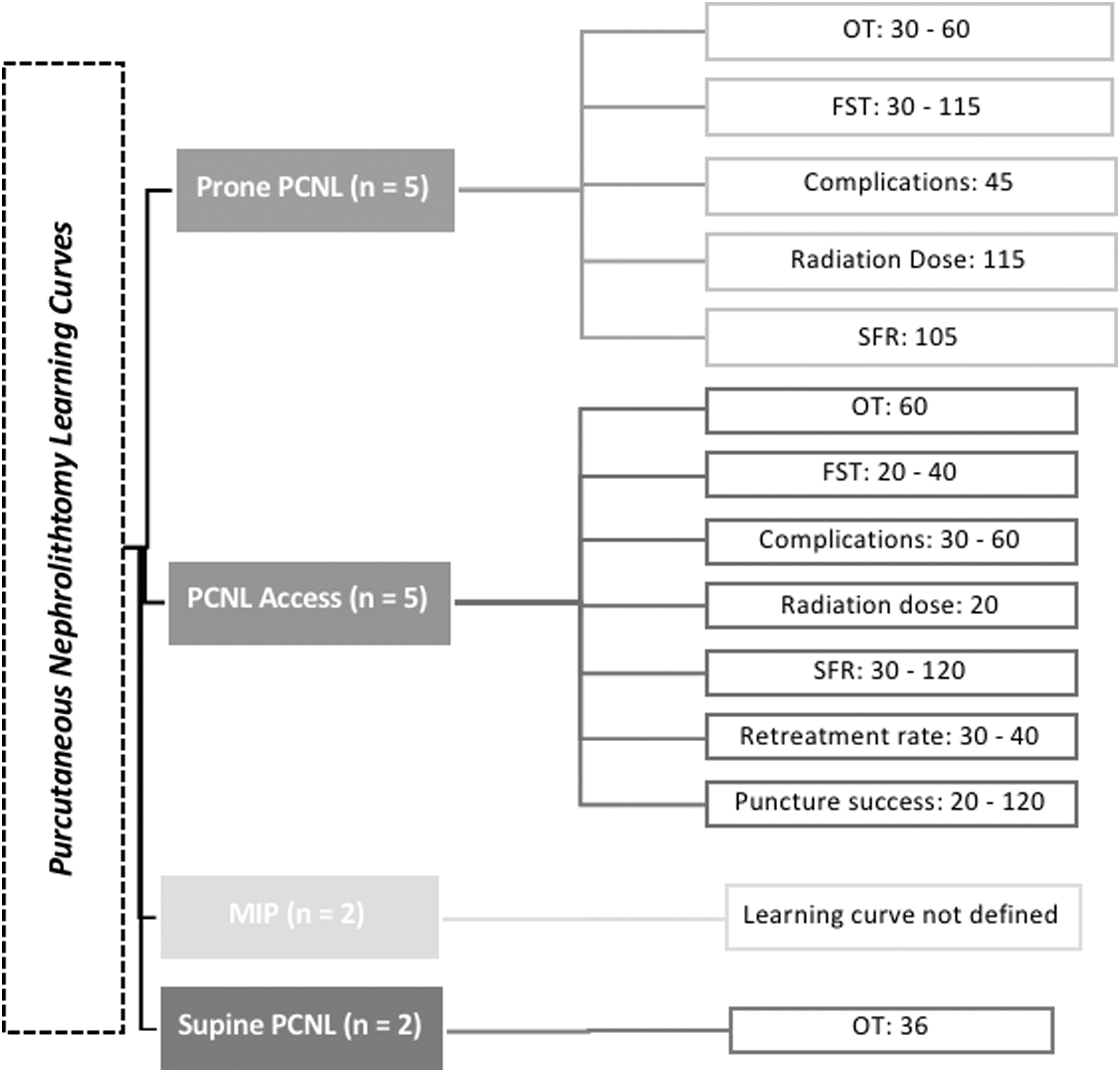
An overview of the evidence of learning curves in PCNL. n = number of studies contributing to the learning curve. FST = fluoroscopic screening time; MIP = minimally invasive percutaneous nephrolithotomy; OT = operative time; PCNL = percutaneous nephrolithotomy; SFR = stone-free rate.
Four studies assessed the learning curves in FURS, identifying that 60 and 56 cases are required for competence in relation to OT and fragmentation efficacy, respectively. For complication rates to plateau, a trainee should have completed 100 FURS procedures, and when observing qualitative measures such as tissue management and dexterity, 60 cases are recommended to achieve competence. However, drawing clearly defined conclusions regarding FURS learning curves for individual outcome measures is challenging due to the scarcity of data in this area at present.
A knowledge of the learning curves for PCNL and URS has important implications for both trainees and trainers. Identifying the learning trajectory allows mentors to tailor training to individual trainees. Learning curves can also aid those designing training tools and assessment ensuring that these programs are delivered at an appropriate rate and knowledge level.
Furthermore, as the popularity of PCNL variations such as supine and minimally invasive techniques increases, an understanding of the impact they have on the learning curve becomes important to ensure that training can be adequately altered to tailor these techniques. 28,29 Additionally, understanding the learning curve for individual steps of the procedure allows for focused training on challenging steps. 30 For PCNL, gaining access to the kidney is often discussed as the most challenging step 31 ; therefore, it is important to understand at what stage trainees should be competent in this, it may indicate when they are able to operate independently.
The ranges outlined in this review can act as a reference point for urology trainees and their mentors to enable them to track their progress and indicate if additional support or focus is required in either PCNL or FURS. Furthermore, these indicators of rate of skill acquisition can be utilized by those designing training programs to ensure that training in urolithiasis is delivered and assessed at an appropriate rate, with the goal of developing accomplished surgeons competent in urolithiasis, a keystone in the delivery of gold-standard healthcare.
Although a thorough search for articles on all urolithiasis procedures was conducted, only studies relating to PCNL and FURS were found. There is a paucity of data pertaining to learning curves in extracorporeal shockwave lithotripsy (SWL) and rigid URS as well as significantly fewer articles on FURS than PCNL. Although less technically complex than PCNL, these procedures make up a large proportion of the urologists' workload and so understanding of their learning curves would still be of great value.
The articles included in this review observed a variety of outcome measures, which differed greatly between studies (Tables 1 and 3). Articles which measured the same outcomes were often not comparable due to different measurement parameters, for example, the article by Schilling and coworkers 17 OT is the time from puncture to closure of the surgical tract, whereas Allen and coworkers define this as the time from the patient entering the operating theater until the time he or she left. 13 Because of the heterogeneity of the studies and a lack of comparable variables, meta-analysis was not appropriate, so descriptive statistics were utilized in this review.
There was variation in whether stone size and complexity was considered. Some of the studies 11,12,17 –21,23,24,26,27 conducted statistical analysis to determine whether the stone size and complexity varied between the cases taken on by novice and expert surgeons. Conversely, others made no reference to these demographics. 13 –16,22,25,32 As a result, it becomes challenging to establish if outcomes found not to be statistically different are in fact that or because of novices being assigned easier cases. To eliminate confounding factors, stone complexity should be assessed using a validated tool, such as the Guy's stone score, 33 S.T.O.N.E. nephrolithometry, 34 or Clinical Research Office of the Endourological Society nephrolithometric nomogram, 35 and thereafter compared for statistical difference between novice and expert groups.
Interpersonal variation is a significant reason for the wide-ranging results in this study. Additionally, prior surgical experience of novices varied greatly; thus, it is impossible to compare the learning curves of these individuals. Observations of operators from the same starting point such as in the multi-surgeon, prospective studies of holmium laser enucleation of the prostate 36 or endoscopic ultrasound and retrograde cholangiopancreatography 37 are required before a true learning curve can be established.
The complexity of issues surrounding the identification of definite learning curves in surgery has been widely discussed. 2,38 –41 An extensive study into statistical assessment of learning curves in health technologies concluded that reliable learning curve assessment will come from multi-surgeon prospective data and “as a minimum, describe the number and experience of the operators, the data source, the proportion of procedures performed by individual operators (to ensure that no one operator dominates).” 38
Future research into learning curves in urolithiasis should be multicenter, multi-operator prospective observations, a suggested method for assessing learning curves is outlined in Figure 3. Participants for these studies should be trainee urologists, with matching factors such as previous operative experience and simulation experience. When trainees commence URS and PCNL operations, the patients' demographics as well as the stone size and complexity should be analyzed to ensure that no significant differences between operator caseload. Consecutive case cohorts should be analyzed statistically and graphically. Standardized outcome measures should be observed; these can be subdivided into patient safety measures and operative efficacy measures. Patient safety measures include radiation dose (if applicable), retreatment rate including the reason for and method of reintervention, LOS, and complication rates measured using the Clavien–Dindo classification. Operative efficacy measures encompass FST (if applicable), SFR where a stone fragment of ≤2 mm is considered insignificant, puncture time, puncture success rate, and OT. Observation of a larger number of trainees using these standardized outcome measures will enable meta-analysis of data in the future and subsequent definition of learning curves. Knowledge of the expected learning curve in each urolithiasis procedure will allow trainee urologists to compare their progress and adapt their training if necessary.
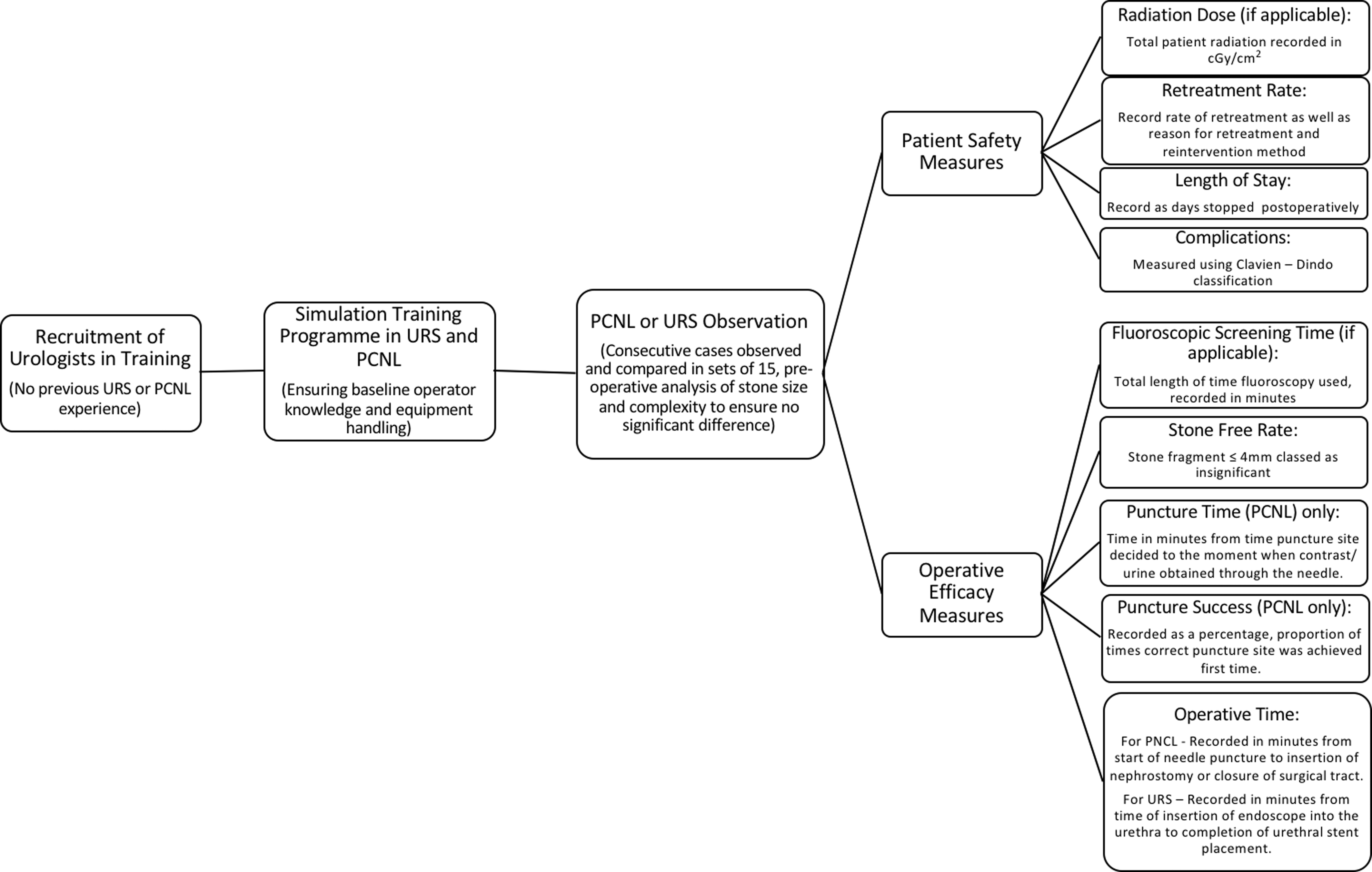
Flowchart of proposed pathway for assessing learning curves in PCNL and URS including outcomes measures and parameters. URS = ureteroscopy.
There are several limitations to the present study; the articles included are low-level evidence and mostly single surgeon, single-center observations. There are no data available to assess the learning curves in urolithiasis techniques other than PCNL and FURS. The lack of continuity in outcome measures means that the meta-analysis is not possible, and it is difficult to compare studies and draw definite numbers of cases required to complete the learning curve. This is in keeping with the findings of other systematic reviews endeavoring to establish learning curves in surgery. 1,42,43 The variability of prior experience of surgeons as well as possible differences in stone complexity and size also hinders definition of learning curves. Additionally, despite a comprehensive and systematic review being conducted, there is always a risk that studies relating to learning curves in urolithiasis have been missed.
Conclusion
There is no doubt over the importance of understanding learning curves in surgery. A systematic review of the evidence available at present has highlighted that 30 to 60 PCNL cases are required to achieve appropriate OTs and between 20 and 115 cases to reach suitable FST. Several conclusions regarding learning curves in PCNL subgroups have also been drawn (Fig. 2). In relation to FURS, 60 and 56 cases should be performed to complete the learning curves relating to OT and fragmentation efficacy, respectively. However, there is a paucity of the literature focusing on the learning curves in urolithiasis procedures such as SWL and rigid URS, and lack of analogous data in articles published on learning curves in PCNL and FURS. Further multicenter multi-operator studies of all urolithiasis techniques with standardized outcome measures will facilitate definite conclusions regarding learning curves.
Footnotes
Acknowledgments
K.Q. acknowledges financial support from the Royal College of Surgeons of England in the form of an Intercalated BSc research award. A.A., K.A., and P.D. acknowledge support from the Urology Foundation and Olympus. P.D. and K.A. acknowledge support from the NIHR Biomedical Research Centre, MRC Centre for Transplantation, King's Health Partners, Guy's and St. Thomas' Charity, School of Surgery, London Deanery, Royal College of Surgeons of England, Intuitive Surgical, EU-FP7, Prostate Cancer United Kingdom, Technology Strategy Board, and the Vattikuti Foundation.
Author Disclosure Statement
No competing financial interests exist.