
Abstract
Purpose:
To assess the extent to which surgical experience can affect perioperative and functional outcomes after photoselective vaporization of the prostate (PVP) with 180W XPX GreenLight laser in patients with lower urinary tract symptoms secondary to benign prostatic obstruction (BPO).
Materials and Methods:
Data from 291 consecutive patients with symptomatic BPO (median follow-up 12 m) were collected and analyzed. Patients were treated at 2 different institutions by 2 expert (G1, n = 182) and 2 novice (G2, n = 109) transurethral prostate surgeons (February 2013 – March 2017) and underwent standard or anatomical PVP depending on surgeons' preferences. Patients' characteristics, perioperative and functional outcomes were compared using the chi-square and Mann–Whitney U tests. Patients' satisfaction was measured using the Patient Global Impression of Improvement (PGI-I) score. Learning curves were analyzed based on changes in quantitative parameters: surgery time, lasing/operative time, and energy delivered (kJ).
Results:
Patients' baseline characteristics, perioperative data and PGI-I score were similar. Overall the complication rates showed better trends for G1. Serum prostate-specific antigen levels, maximum flow rate, and International Prostatic Symptoms Score improved in both groups, with perceived improvements greater in G2 (p < 0.006). Lasing time/operative time ratio showed greater evolution for G1 than G2 (0.50:IQR 0.38–0.60 vs 0.46:IQR 0.34–0.58, respectively)(p = 0.201). A major increase in energy delivery for G2 was achieved within the first 50 procedures, whereas more than 100 iterations were needed for G1 to reach LT/OT >60%.
Conclusion:
Surgeons' background and expertise appear to affect outcomes over the learning curve, with roughly similar perioperative and functional results.
Introduction
B
GreenLight laser PVP has been standardized and described at all levels, from standard PVP to more complex procedures involving enucleation. 6 What remains to be assessed, however, is how to quantify experience, that is, the threshold number of operations required to achieve a sufficient level of expertise. Only a few studies have addressed this issue, and data are limited because the technique has evolved considerably since its introduction in 1998. 7 As a result, learning curves have yet to be adequately described.
The aims of this study were to compare learning curves between expert and novice surgeons from two different institutions, and evaluate the extent to which surgical experience can affect perioperative and functional outcomes after PVP.
Materials and Methods
Clinical data
We analyzed data from 291 consecutive BPO patients undergoing PVP with 180-W XPS GL laser at two different institutions. Data were recorded in a prospectively maintained database between February 2013 and March 2017. Subjects were divided into two groups. Group 1 included senior surgeons experienced in transurethral resection of the prostate (TURP) (>130 TURPs each) and Group 2 included novice surgeons (<30 TURPs). Expert and novice surgeons were from different institutions and nobody had previous experience with first generation of Greenlight.
Patient assessment and indications for BPO surgery were according to the European Association of Urology (EAU) guidelines on the management of non-neurogenic male LUTS. 2 Individuals with a history of prostate cancer or severe neurological diseases were excluded. Preoperative assessment included age, prostate volume, any anticoagulant and antiplatelet therapies, phytotherapy, alpha-blockers and 5-alpha reductase inhibitors therapies, ASA (American Society of Anesthesiologists) score, International Prostate Symptom Score (IPSS), serum prostate-specific antigen (PSA) levels, and maximum urinary flow (Qmax). History of catheterization was also reported.
Perioperative parameters such as surgery time, irradiation time, energy delivered, postoperative length of catheterization, postoperative hospital stay, and acute urinary retention were recorded. Intra- and postoperative adverse events were reported using the Clavien–Dindo classification. 8 Complications were registered as “early” (within 30 postoperative days) in the presence of fever, postoperative urinary retention, burning urination, frequency, de novo urge, de novo urge incontinence, and stress incontinence if they required medications or medical advice; or “late” (after 3 months) in the presence of de novo urethral strictures, bladder neck contracture, and reinterventions for residual adenomas.
Postoperative outcomes such as PSA, IPSS, and Qmax were compared at baseline and at 6 months. The patients' perceptions of improvement were assessed using a single item questionnaire, the PGI-I, 9 that included patients greatly improved (score-1) to very much worsened (score-7). Even if the original questionnaire was based on 7-item scale, since items 3-6-7 were selected by very few patients, it was decided to incorporate them together (1 greatly improved–2 improved–3 + 4 not changed–5 + 6 + 7 worsened).
The study was approved by the Institutional Ethics Committee and all patients gave their informed consent before surgery.
Surgical technique
In both groups, the procedure was carried out with a GreenLightTM 180-W XPS laser. A MoXy fiber was inserted through the working channel of a continuous, double-flow, 26Ch resectoscope using 0.9% saline as an irrigant. Surgeons opted for either the so-called International Greenlight User Groups (IGLU) modular technique used in classical PVP 10,11 or the anatomical technique as described by Gomez Sancha. 12 IGLU-PVP was performed as follows. Initially, with a urethrocystoscopy, the ureteral orifices were visualized as the presence of bladder tumor was escluded. An initial incision was created at either the 5 or 7 o'clock position down to the surgical capsule, after which the middle lobe was vaporized, followed by the lateral lobes and the apex. The laser was operated in a centripetal direction starting from the capsule, and was aimed more deeply into the tissue to reduce the risk of perforation or bleeding. Upon completion of the procedure, the prostatic fossa was reviewed and hemostasis checked.
In the so-called anatomical PVP, a standard central cavity was first created, after which the capsular localization maneuver described by Sancha 12 was performed on both sides, and a careful mechanical dissection was carried out toward the bladder neck at the 6 o'clock position. The adenomatous tissue was incised down to the capsule, which was then vaporized laterally and anteriorly following the capsular plane.
Platelet aggregation inhibitors were maintained where needed, 13 and low molecular weight heparin was administered to patients requiring bridge therapy. 14 The procedures were mainly performed under spinal anesthesia, and antibiotic prophylaxis was administrated according to institutional protocols.
Learning curve parameters
We created two consecutive groups, each including one novice and one expert surgeon. At study onset, all surgeons were new to GreenLightTM 180-W XPS PVP. To assess learning curves, we analyzed the following parameters: surgery time (min), lasing time (min)/operative time (min) (%) (LT/OT), and energy delivered (kJ). Surgeons aimed to achieve the same reference values for LT/OT as those reported in the literature, based on a comparison of functional outcomes and operative complications. Thresholds for learning curve evaluation were set at 50 and 100 procedures, and comparisons were made in terms of LT/OT ratio and energy delivered. The analysis focused on changes in IPSS, Qmax, and PSA between the two groups at 6 months. Patients who needed concomitant endoscopic treatment or intraoperative conversion into TURP were excluded.
Statistical analysis
Quantitative variables were summarized as mean and standard deviation (SD) or median and interquartile range (IQR) according to their distribution. Qualitative data were summarized as frequency and percentage. Departures from normal distribution were evaluated for each variable using a Shapiro–Wilk's test (results are reported separately for each group, that is, expert vs novice surgeons). Cross-group differences in frequency were assessed with a chi-square test, while quantitative parameters were analyzed using the Mann–Whitney U-test. The Wilcoxon signed-rank test was applied to paired data to measure absolute variations of functional outcomes in Group 1 and Group 2.
Patients' satisfaction was measured with the PGI-I score. Learning curves were analyzed based on changes in the following quantitative parameters: surgery time, lasing/operative time, and energy delivered (kJ). The variable of interest was the dependent variable, and patient's rank was the predictor (independent variable). We used linear regression analysis to evaluate the determinants of lasing time/operative time ratio, and third order polynomial (cubic) curves to describe the relationship between lasing time/operative time ratio and sequence number of patients. Statistical significance was set at p < 0.05 and all analyses were carried out using IBM® SPSS Statistics v 20.0 (SPSS, Inc., Chicago, IL).
Results
Baseline and perioperative patients characteristics
A total of 291 consecutive patients were included. Table 1 shows baseline characteristics while Table 2 peri-postoperative outcomes and complications. Median age was 69.0 for Group 1 (IQR 63.0–75.0) and 71.0 (IQR 65.0–77.5) for Group 2. No differences in perioperative parameters were observed. Median operative time for Group 2 exceeded that for Group 1 by 5 minutes (55 minutes, IQR 41.5–66.3 vs 60 minutes, IQR 40.0–75.0, p = 0.777). Significant differences between the two groups were found in distribution of PGI (p = 0.015) and Clavien-Dindo grades (p < 0.001). Early complications were found in 39.6% and 56.9% of Group 1 and Group 2 patients, respectively (p = 0.004). No significant differences were found for late complications (19.8% vs 22.0%; p = 0.647).
Data expressed as median and interquartile range.
Statistically significant p is highlighted in bold type.
p-value relative to Mann–Whitney U Test.
p-value relative to Chi-Squared Test.
BPH = benign prostatic hyperplasia; TURP = transurethral resection of the prostate.
Data are expressed as median and interquartile range.
Statistically significant p is highlighted in bold type.
p-value relative to Mann–Whitney U Test.
p-value relative to Chi-Squared Test.
PVP = photoselective vaporization of the prostate.
Functional outcomes
Functional outcomes at 6 months postoperatively are shown in Table 3 and Fig. 1. Serum PSA levels, Qmax, and IPSS improved significantly in both groups. The relative variation in IPSS was statistically significant in both Group (−0.67 vs −0.71) with higher variation in G2 (p < 0.006).
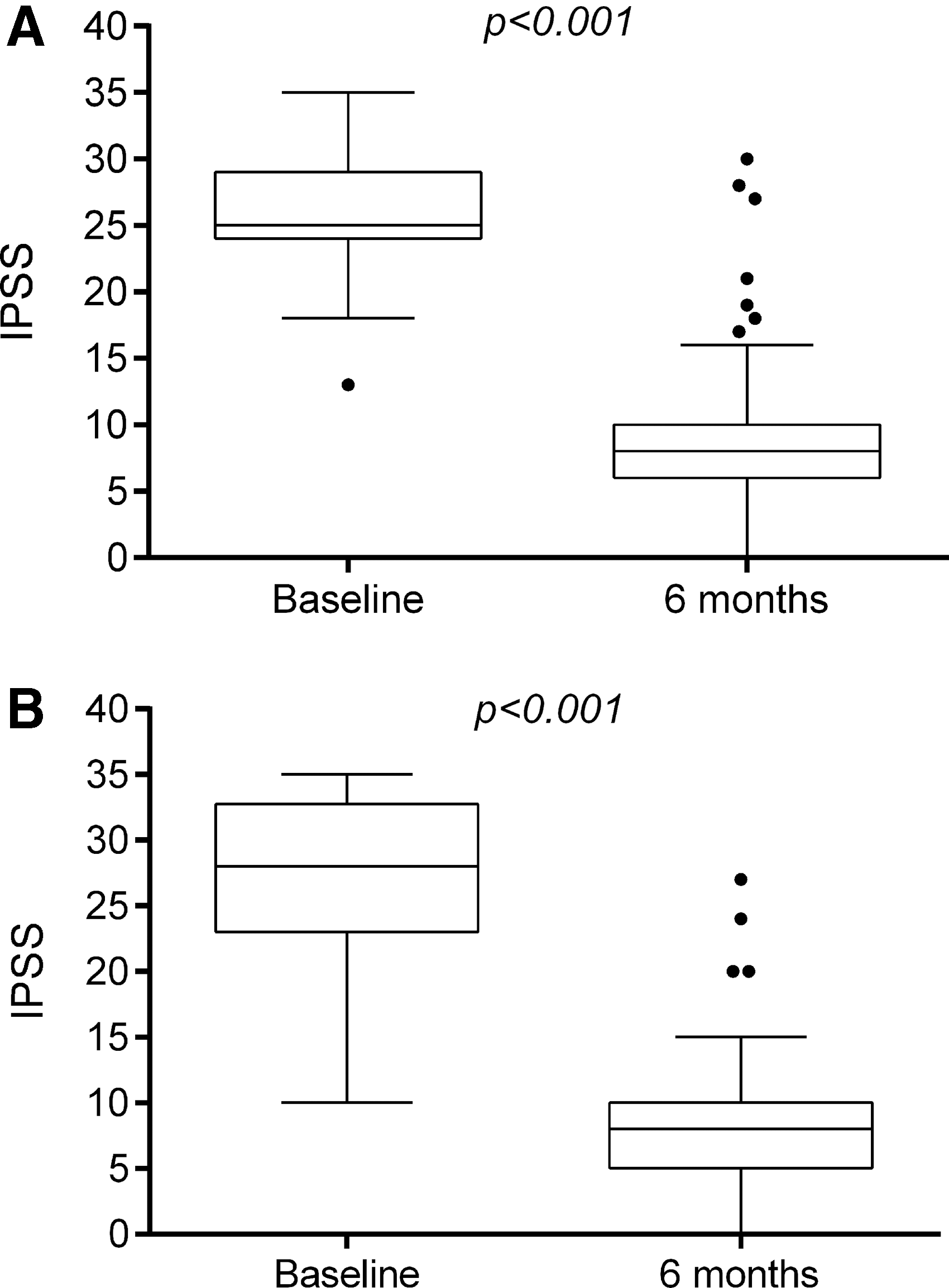
Box-and-whisker plots of IPSS values at baseline and at 6 months post-PVP. Graphs show the 25th and 75th percentile range (box) with 95% confidence intervals (whiskers) and median values (transverse lines in the box). The Wilcoxon signed-rank test shows statistically significant differences between two time points.
Data are expressed as median and interquartile range.
Statistically significant p is highlighted in bold type.
p-value relative to Wilcoxon signed rank test.
p-value relative to Mann–Whitney Test U between relative variation.
PSA = prostate-specific antigen; IPSS = International Prostate Symptoms Score; UFM = uroflowmetry.
Learning curve evolution
No significant differences in operative time were found between the two groups. Learning curve analysis showed greater evolution in lasing time/operative time ratio for Group 1 than Group 2 (0.50:IQR 0.38–0.60 vs 0.46:IQR 0.34–0.58, respectively) (p = 0.201) (Fig. 2).
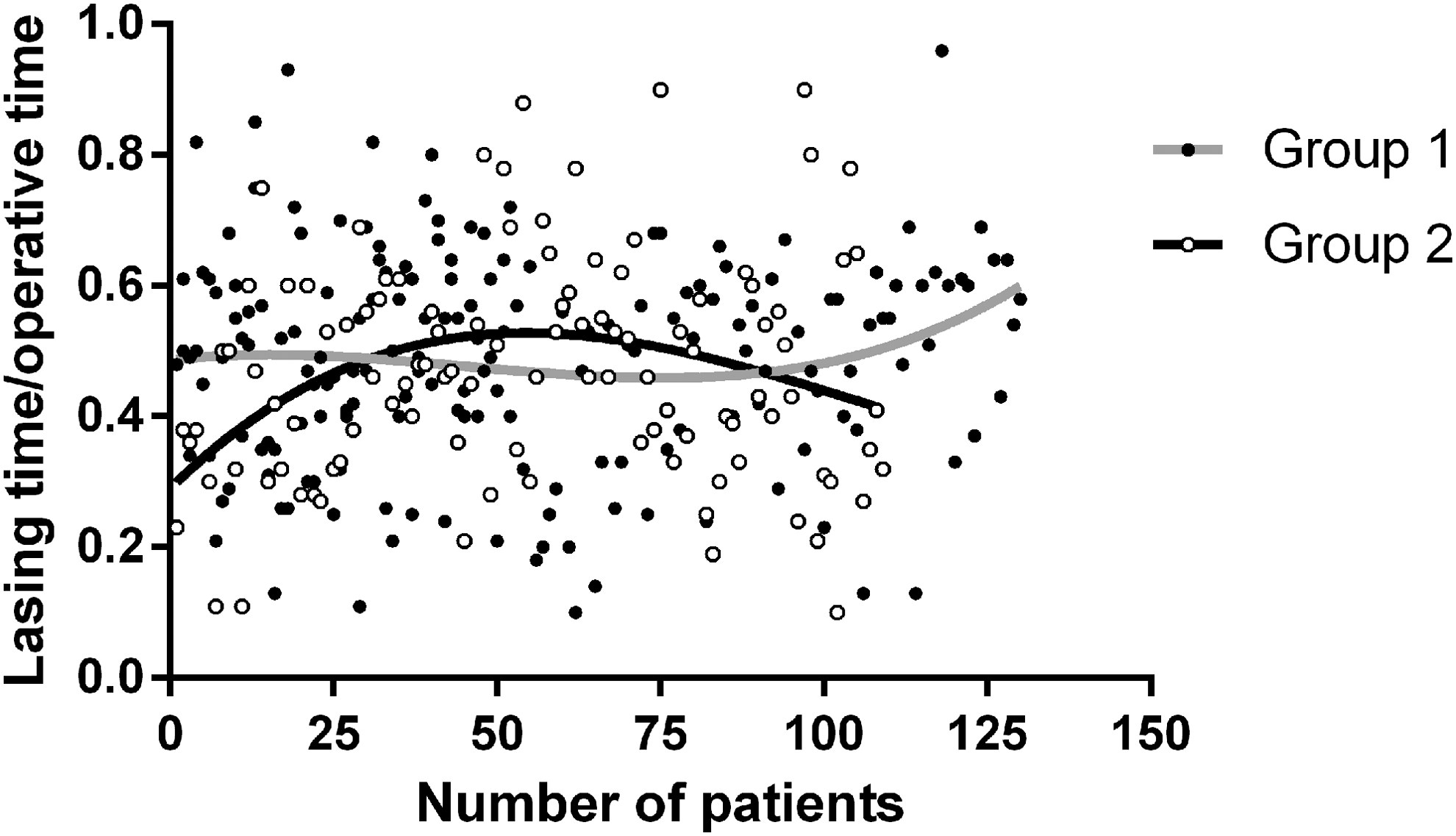
Evolution of lasing time/operative time ratio.
Discussion
GreenLight Laser PVP for the treatment of LUTS in men with BPO is regarded worldwide as a simple and effective procedure. 15,16 An interesting development came about with the introduction of the 180-W-XPS laser system. Surgeons have experimented extensively with it and have devised new techniques that combine vaporization with resection and enucleation to improve prostatic tissue resection in larger glands. 17 An understanding of the learning curve is crucial to determine how much experience is required to provide reproducible outcomes; however, only a few studies to date have investigated learning curve variability in relation to the GreenLight 180-W XPS laser. 18 –20
In a study from 2017, Bastard et al. compared the work of three senior surgeons, all experts in TURP, and analyzed individual proficiency and corresponding differences. The authors concluded that surgeon experience affects perioperative outcomes over the learning curve, with about 100 procedures being required to reach a plateau regardless of baseline expertise. 21 To the best of our knowledge, no studies have compared learning curves between expert and novice surgeons from different institutions, or have investigated how surgical experience can affect perioperative and functional outcomes post PVP.
Our results show no significant variations in LT/OT ratio between Group 1 (senior surgeons) and Group 2 (novice surgeons), while learning curve evolution showed different trends. In Group 2, a significant increase in LT/OT ratio was registered between the 1st and 50th patient, reflecting increased familiarity with the PVP technique. Conversely, more than 100 procedures were needed in Group 1 to finally obtain a consistent increase and reach an LT/OT ratio >60%. 22,23 This difference may be due to the fact that expert surgeons began performing anatomical PVP from the onset, resulting in an initial decrease in LT/OT ratio, whereas novice surgeons did not switch to the anatomical technique until classical PVP had been mastered. Our data also confirm previous reports that unexperienced operators need at least 30–50 procedures to attain significant improvements 6 and benefit from being coached by a tutor, notwithstanding the proven efficacy of the dedicated GreenLight simulator in teaching the basics. 24
All functional outcomes are in line with the available literature. 25 We reported an overall symptoms improvement at 6 months post-PVP, with absolute variations in IPSS, PSA, and Qmax, which are statistically significant in both groups. 26,27 However, as demonstrated by Seki, improvements in proficiency levels did not translate into better functional outcomes. 28 Patients' satisfaction after PVP was consistently high, although with statistically significant differences between the two groups, and the self-reported improvement rate overlaps with data from other series. 29 As regards safety, our results show statistically significant differences in favor of expert surgeons, but this finding must not be overinterpreted. In fact, all complications were Clavien grade I and most were temporary storage symptoms often reported in all transurethral procedures. 30 As with functional outcomes, there was no connection between complication rates and the length of the learning period. 28
Taken together, our findings suggest that: (a) PVP can be quickly taught and safely mastered without compromising functional results, even in patients operated on by novice surgeons; (b) greater experience in endoscopic procedures is important to ensure good surgical outcomes early in the learning curve; and (c) a continuous effort toward improving performance is essential to optimize energy use.
This study is not without limitations. One major concern is related to the retrospective nature of the analysis and the unbalance between groups. Also, no distinction was made between standard and anatomical PVP. A larger sample size would no doubt guarantee a more robust assessment of the study variables; on the other hand, we believe that our method for analyzing surgeon progress could also be applied to larger series. Differences in daily practice between centers and in operating frequency were not investigated. The time between one procedure and the next is arguably an integral part of the learning curve; however, operating times appear to be more linked to prostate volume and this should be taken into account when analyzing evolution trends. Finally, a longer follow-up and a healthcare costs analysis would be beneficial. Despite these limitations, to the best of our knowledge this is the first study to compare PVP learning curves between expert and novice surgeons, emphasizing once more the flexible nature of the GreenLight laser system.
Conclusion
Although a few groups have tried to set learning curves for PVP, this is the first study that applies learning curve analysis to assess how expert and novice surgeons compare to each other. Our data confirm the effectiveness and safety of the GreenLight 180 W-XPS system, and show how individual background and expertise can affect outcomes with roughly similar perioperative and functional results. This issue remains crucial for a more accurate understanding of the potential of PVP.
Footnotes
Author Disclosure Statement
No competing financial interests exist.