
Abstract
Introduction:
Ureteroscopy (URS) and percutaneous nephrolithotomy (PCNL) are common procedures performed to treat kidney stones. Despite advances in technology/technique, serious infectious complications can occur. To better understand the preoperative antibiotic administration patterns and adherence to guidelines from the American Urological Association (AUA) and the European Association of Urology (EAU), members of the Endourological Society were sent a clinical vignette-based survey to assess the antibiotic use in a variety of pre-URS and pre-PCNL scenarios.
Methods:
Endourological Society members were e-mailed a survey that queried antibiotic therapy duration before uncomplicated URS and PCNL with negative and asymptomatic positive preoperative urine cultures (PUCs). For negative PUC questions, selecting more perioperative antibiotics was considered a “prolonged” course as it extends past the maximum of 24-hour perioperative prophylaxis recommended by both the AUA and EAU.
Results:
The response rate was 16.3% for a total of 326 responders. Twenty-one percent to 39% of respondents reported giving prolonged courses of preoperative antibiotics before a URS or PCNL with a negative PUC (p < 0.0001). When presented with a negative PUC, more prolonged antibiotic courses were reported with the following hierarchy: PCNL for 2 cm intrarenal stones (39%) > URS for 12 mm renal pelvis stone (28%) > URS for 7 mm distal ureteral stones (21%) (p < 0.0001). In both negative and positive PUC questions, differences were noted in preoperative antibiotic prescribing patterns among site of practice (United States, Canada, Europe, Asia, South America, and Others), type of practice (academic vs all others), years in practice (<10 or ≥10 years), and surgical volume (URS and PCNL >100 or ≤100 annual cases).
Conclusions:
Adherence to guidelines on antibiotic administration before PCNL and URS with a negative PUC varies by scenario and provider. In 21% to 39% of negative PUC cases, reported antibiotic use before a URS or PCNL is not consistent with recommendations from the AUA and EAU. Before a positive PUC URS or PCNL, nearly all surveyed provide preoperative antibiotics; however, the regimen length is variable.
Introduction
D
Despite relative agreement for immediate perioperative antibiotic prophylaxis, there is no consensus regarding antibiotic use the days leading up to URS or PCNL. 4,7 –9 To better understand the preoperative antibiotic administration patterns and adherence to recommendations from the AUA and EAU, members of the Endourological Society were asked to complete a clinical vignette-based survey assessing the antibiotic use in a variety of pre-URS and pre-PCNL clinical scenarios.
Methods
A 13-question survey was created using
Questions 1 to 6 (Table 1) gathered physician demographic data, including site of practice, type of practice, years in practice, endourology fellowship training, and number of ureteroscopic and percutaneous stone removal cases per year. Questions 7 to 13 (Table 2) presented physicians with clinical scenarios and asked them to select which antibiotic regimen they would recommend in each case. The scenarios were designed to include patients who would soon undergo operative intervention for a urinary stone and varied in procedure type (URS vs PCNL), preoperative urine culture (PUC) results, stone size, and stone location. All patients described in questions 7 to 13 were healthy other than the symptoms listed. No patients featured staghorn calculi. Vignette patients with positive PUC results had no signs or symptoms of a urinary tract infection, signifying asymptomatic bacteriuria.
Survey questions were designed to evaluate identical clinical scenarios with negative and positive PUC results. For negative PUC questions, we considered giving more perioperative antibiotics to be a “prolonged” course as it extends past the 24-hour window recommended by both the AUA and EAU. Since there are no clinical guidelines by a major professional organization to direct preoperative antibiotic use in the setting of a positive PUC, there is no “prolonged” assessment for these questions. Instead, we produced a characterization of responses.
Statistical analyses
Descriptive statistics include survey responses reported by frequency. Survey responses and categorical variables were compared using chi-square analysis with Fisher's exact test used for cell sizes <5. When appropriate, all statistical tests were two-sided with p < 0.05, except in cases of multiple comparisons where a Bonferroni correction was performed. Statistical analyses were performed with the Statistical Package for the Social Sciences (SPSS) (IBM, Armonk, NY).
Results
A total of 369 individuals returned surveys, with an overall response rate of 18.5%. Of these, 43 did not have every question answered and were excluded for a total of 326 (16.3%) respondents. Among these responders, 136 (41.7%) practiced in the United States, 210 (64.4%) held academic positions, 218 (66.9%) had completed an endourology fellowship, and 60% had ≥10 years of experience as a urologist. Additionally, 154 (47.2%) and 49 (15.0%) reported performing >100 annual URS and PCNL procedures for stone, respectively. Response frequencies for the demographic questions are listed in Table 1. Response frequencies for the clinical vignettes are represented in Figure 1.
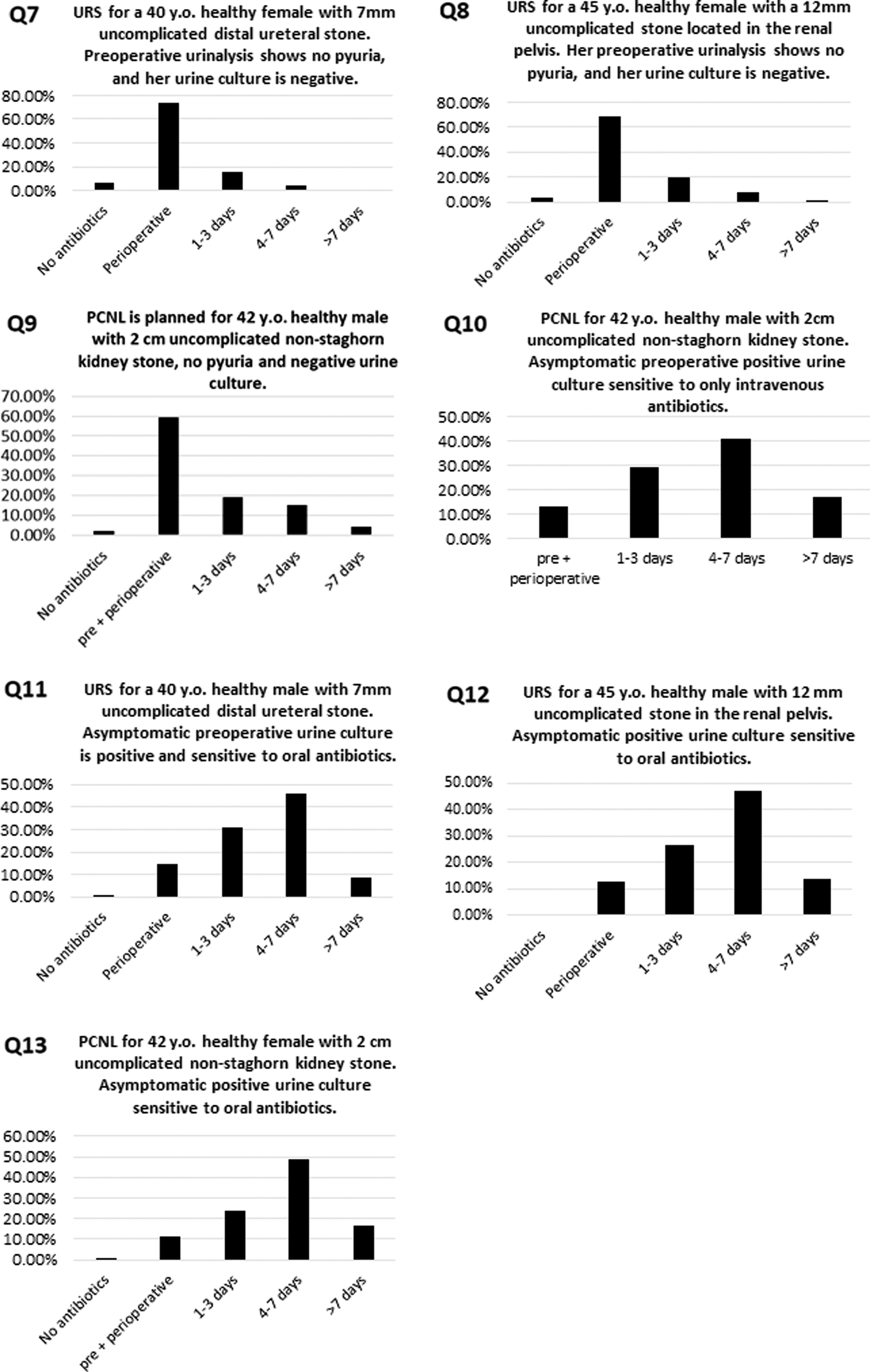
Clinical judgment responses with abbreviated questions and answers. PCNL = percutaneous nephrolithotomy; URS = ureteroscopy.
Negative PUC vs positive PUC
Each “negative PUC” question was evaluated with respect to its “positive PUC” question. The number of respondents giving ≥1, ≥4, and >7 days of preoperative antibiotics were analyzed (Table 3). Across all preoperative antibiotic durations, longer courses of antibiotics were used for positive PUC than negative PUC questions (p < 0.001).
No respondents reported giving >7 days of antibiotics for Q11.
Negative PUC: distal ureteral URS vs renal pelvis URS vs renal pelvis PCNL
To assess the use of prolonged antibiotic courses among the negative PUC vignettes (Q7–9), each was compared against the other in Table 4. Prolonged courses of preoperative antibiotics were more frequently given before a URS for a renal pelvis stone than a URS for a distal ureteral stone (p < 0.0001). Prolonged preoperative antibiotics were given more frequently before a PCNL than before URS for either a renal pelvis or a distal ureteral stone (<0.0001). Finally, 21% to 28% of respondents reported giving more antibiotics than just a single perioperative dose before URS and 39% give more than a single preoperative dose followed by perioperative antibiotics before a PCNL.
Negative PUC: site of practice—question 1
Statistically different courses of preoperative antibiotics were seen in the negative PUC URS questions (Q7 and 8). There were no statistically significant results across all sites of practice for the negative PUC PCNL vignette (Q9) (Table 5). Relative to other sites, Europeans tended to avoid prolonged courses of preoperative antibiotics when posed with a negative PUC before a URS for a distal ureteral stone (Q7) (p = 0.049). Respondents from Asia tended to give prolonged courses of preoperative antibiotics for both URS questions (Q7 and 8) (p = 0.002 and p = 0.001, respectively). Finally, U.S. physicians tended to avoid prolonged antibiotic courses before a URS for a renal pelvis stone (Q8).
Bonferroni adjusted p-values.
Negative PUC: type of practice, years in practice, and endourology fellowship training—questions 2 to 4
Given the large proportion of respondents practicing in an academic setting (n = 210, 64%), our analysis evaluates them against all others. For the negative PUC questions, there was no statistically significant difference in reported preoperative antibiotic use between academic and nonacademic urologists (p = 0.092).
Years in urologic practice was divided into those in practice for <10 or ≥10 years, and there was no statistically significant difference in antibiotic use between these groups (p = 0.216–0.338).
Respondents were separated into two groups that comprised those with and without endourology fellowship training. Endourology fellowship-trained respondents gave more prolonged courses of antibiotics before a negative PUC PCNL (Q10) (p = 0.044). Complete data for this subsection can be found in Supplementary Table S1 (Supplementary Data are available online at
Negative PUC: surgical volume—questions 5 to 6
For URS and PCNL, groups were defined as those performing ≤100 and >100 PCNL or URS procedures per year. Questions 7 and 8 involve negative PUC URS procedures, and for each, there was no difference in prolonged preoperative antibiotic use (p = 1.0 and p = 0.452, respectively). The negative PUC PCNL question (Q9) demonstrated that those who perform >100 PCNL procedures per year tended to give prolonged courses of preoperative antibiotics (p < 0.001) (Supplementary Table S2).
Positive PUC analysis
Among the six sites of practice, respondent type and years of practice, endourology fellowship training status, and surgical volume, the responses for questions 10 to 13 were relatively consistent and not statistically different. Nevertheless, some differences were seen in reported lengths of preoperative antibiosis. Answer choices generally included: no antibiotics, a perioperative dose, 1 to 3 days, 4 to 7 days, and >7 days. The complete results are presented in Supplementary Tables S3 to S5.
Positive PUC: site of practice—question 1
More often than all other sites of practice, Asian participants gave <1 day of antibiotics when posed with a positive PUC sensitive to oral antibiotics before a URS for a distal ureteral stone (Q11) (p = 0.005). The same was true for Asia in the scenario involving a positive PUC before a PCNL susceptible to oral antibiotics (Q13) (p = 0.01). Also, South American respondents more often gave ≥1 day of preoperative antibiotics for Q10, which presents a positive PUC before PCNL sensitive only to intravenous (IV) antibiotics (p = 0.01). For a complete analysis of responses for these questions, please refer to Supplementary Table S3.
Positive PUC: type of practice, years in practice, and endourology fellowship training—questions 2 to 4
Respondents in an academic practice tended to give <1 day of preoperative antibiotics for positive PUC PCNL sensitive to IV antibiotics (Q10) (p = 0.018). In a similar manner, academics tended to give <4 days for a positive PUC PCNL sensitive to oral antibiotics (Q13) (p = 0.05). Across the type of practice, years in practice, and fellowship training categories, there were no statistically significant differences in preoperative antibiotic practices ≤7 or >7 for any positive PUC question. For a complete analysis of responses for these questions, please refer to Supplementary Table S4.
Positive PUC: surgical volume—questions 5 to 6
Respondents in the >100 URS and >100 PCNL groups had no statistically significant differences in their preoperative antibiotic use in the <1 or ≥1 day and <4 or ≥4 days comparisons (p > 0.08). However, for Q12, those who annually perform >100 URS procedures more frequently answered that they would give >7 days of antibiotics (p = 0.037). Urologists who perform >100 PCNL procedures per year tended to give >7 days of preoperative antibiotics for Q13 (p = 0.002) (Supplementary Table S5).
Discussion
Our study provided clinical vignette-based data that characterize preoperative antibiotic practices before URS and PCNL among urologists in the Endourological Society. This information highlights clinical scenarios wherein antibiotic use not consistent with various guidelines may occur and serves as a current picture of antibiotic practice patterns in the “real world.”
Post-surgical infections are morbid and costly 10 ; therefore, much attention has been devoted to mitigating their incidence. For decades, the type of perioperative antimicrobial agents, 11 –13 duration, 14 and timing 15 of drug administration have been refined. This knowledge has been compiled and disseminated through the AUA's Best Practice Statement on urologic surgical antimicrobial prophylaxis 16 and the EAU's guidelines on urologic infections. 17 Despite the veracity of these publications, the use of perioperative antibiotics in accordance with guideline recommendations continues in urology. 18
Negative cultures
At this point, the benefit of preoperative antibiotic courses before a negative PUC PCNL is unclear. Two studies suggest that 1 week of ciprofloxacin or nitrofurantoin before a PCNL can reduce the risk of urosepsis. 19,20 However, a recent randomized controlled trial suggests that there is no benefit for patients with a negative PUC and no urinary drains. 9 Nevertheless, there is evidence for limited perioperative antibiotic administration.
The AUA recommends that URS and PCNL patients be given <24 hours of perioperative antibiotics. 16 The EAU guidelines do not recommend prophylaxis for simple diagnostic URS, and it is optional for ureteroscopic stone management. 17 Despite these recommendations, our study found that 21% to 39% of respondents give prolonged antibiotic courses before a negative PUC URS or PCNL. Additionally, in the context of a negative PUC, prolonged preoperative antibiotic courses were more frequently given before surgery for a 12-mm renal pelvis stone than for a smaller 7-mm distal ureteral stone. Longer operative times have been implicated in higher rates of post-URS sepsis in patients with a negative PUC. 21 –23 Similarly, larger stone size has also been shown to increase the risk of post-URS sepsis. 24 Knowledge of these risks may explain why respondents would give significantly more prolonged courses of antibiotics for a larger renal pelvis stone despite the lack of support in current guidelines.
Respondents from origin regions for these statements (the United States and Europe) largely adhered to them as they did not give significantly more prolonged courses of antibiotics before URS or PCNL. However, for both Questions 7 and 8, participating Asian urologists did give significantly more prolonged antibiotic courses. One reason for this disparity could be that these guidelines are not readily available in languages native to urologists in Asia. To address these practice differences, Asian, European, and American urologic societies may consider developing regionally relevant curricula based on the evidenced-based EAU and AUA guidelines.
In negative PUC scenarios, antibiotic prescribing patterns before URS and PCNL were generally consistent when further delineated by endourology fellowship training, surgical volume, and type and years of practice. However, for Question 9, endourology fellowship-trained participants generally gave more prolonged courses of antibiotics before a PCNL with a negative PUC. The same was true for those who perform >100 PCNL procedures annually. The decision behind preoperative antibiotic use is made with respect to a patient's overall clinical course and comorbidities. The clinical acumen of those who perform >100 annual PCNL procedures and the additional training of the fellowship-trained group may lead them to perform PCNL on patients who are more medically complex, thus requiring more preoperative antibiotics for reasons not captured in our survey.
Positive cultures
In positive PUC cases, preoperative antibiotic administration before PCNL and URS lacks specific clinical guidelines. Despite this limitation, there was overwhelming agreement in the need to treat a positive PUC before surgery. This factor is likely due to the large body of literature, which shows that the risk of postoperative infection is much higher for both URS and PCNL when performed with a positive PUC. 24 –28 However, there was less consensus on the length of preoperative antibiosis.
Just over half of respondents report giving ≥4 days of antibiotics before a URS with a positive PUC. An exception to this was that Asian participants tended to give <1 day of antibiotics when posed with a positive PUC before a URS for a 7-mm distal ureteral stone.
There are no association-sponsored guidelines for preoperative antibiotics for a positive urine culture before a URS. However, there is now level 2B evidence to support at least 5 days of culture-specific antibiotics in patients with a positive urine culture before URS. 28 Perhaps as this new information is disseminated, longer preoperative antibiotic courses in this context will become more common.
When posed with a positive PUC before a PCNL, more than half of respondents report giving ≥4 days of oral or IV antibiotics. This practice is supported by a recent review, which offers grade 2A recommendations for treating a positive PUC before PCNL and for all patients undergoing PCNL to receive prophylactic antibiotics. 28 While there is good evidence to support antibiotics to clear a positive PUC before PCNL, the optimal length and method of treatment have not been established. From our study, nearly two-thirds of respondents answered that a positive PUC susceptible to oral antibiotics requires ≥4 days of treatment before PCNL. Compliance to this recommendation decreases to 57.9% when the culture is susceptible only to IV medications, which may be due to an assumption of superior bioavailability of IV antibiotic formulations.
Limitations of this study are shared with other survey-based practice evaluations. While it is interesting to understand the thought processes and patterns of antibiotic use of members of the Endourological Society, this is a select group of practitioners who more frequently perform these endoscopic procedures. Additionally, those who respond to a survey may feel strongly about the questions/topics discussed, skewing the results in a specific direction, particularly with a net response rate of 16.3%. Finally, our survey operates within the assumption that the URS or PCNL is uncomplicated and does not entirely account for procedural factors or comorbidities that could increase the risk for an infectious complication. Despite these limitations, it is important to characterize the preoperative antibiotic prescribing tendencies of an “expert” group of urologists to promote future investigation into more detailed recommendations for preoperative antibiotic prophylaxis.
Conclusions
Our international vignette-based survey study has identified scenarios and provider subpopulations in which the AUA and EAU guidelines are less widely adhered to and prolonged preoperative antibiotic courses are prescribed.
When faced with a positive urine culture before a URS or PCNL, nearly all surveyed urologists provide some but varied duration in preoperative antibiotics. Randomized controlled studies are needed in this subset to guide appropriate duration of antibiotics.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.