
Abstract
Background and Purpose:
Although several different ureteral access sheaths (UASs) of ≤10/12F are commercially available, their advantages and disadvantages during retrograde intrarenal surgery (RIRS) are still unknown. This study aimed to evaluate the difference in intrapelvic pressure (IPP) between different UASs of ≤10/12F with several irrigation pressure settings.
Materials and Methods:
Five different commercially available UASs (9.5/11.5F Flexor®, 10/12F ReTrace®, 10/12F Bi-Flex®, 10/12F Proxis®, and 10/12F UroPass®) with the thinnest ureteroscope (UFR-P6®) were tested with eight different irrigation pressures (40–180 mbar) in an ex vivo porcine kidney model. Diameters of each part of the UASs were measured using a digimatic caliper, and IPP and irrigation outflow (IOF) rates were evaluated at the time of reaching the plateau of maximum IPP.
Results:
The 9.5/11.5F Flexor had the narrowest inner diameter and the 10/12F UroPass had the widest outer diameter among UASs (both p < 0.05). The 10/12F UroPass and 10/12F Bi-Flex provided an IPP below 40 cm H2O at all irrigation pressures, whereas the 9.5/11.5F Flexor, 10/12F Proxis, and 10/12F ReTrace provided such an IPP at irrigation pressures of <60, 120, and 120 mbar, respectively. Similar to IPP, the 10/12F UroPass and 10/12F Bi-Flex had a significantly higher IOF rate than that of the other UASs at all irrigation pressures (both p < 0.05).
Conclusion:
The 9.5/11.5F Flexor is the thinnest UAS and may provide excessive IPP during RIRS. Among 10/12F UASs, 10/12F UroPass and 10/12F Bi-Flex can provide a safe IPP and good IOF at any irrigation pressure.
Introduction
R
Several small-sized UASs (≤10/12F) are commercially available, and can possibly decrease the insertion force, which affects ureteral wall tension and the risk of ureteral injury. 8 However, a small-sized UAS can cause a higher IPP because of low irrigation outflow (IOF) through the narrow gap between the f-URS and UAS, leading to postoperative hemorrhage, sepsis, and renal extravasation. 4,9 This is one of the dilemmas of surgeons when they select a UAS during RIRS. Moreover, a recent study showed that diameters of UAS are different depending on companies, even if indicated as the same Fr commercially. 10 Therefore, we consider that understanding the properties of UASs is important for urologists to appropriately use them, especially for small-sized UASs.
In this study, we evaluated IPP and the IOF rate between different UASs of ≤10/12F with several irrigation pressure settings using the thinnest ureteroscope in an ex vivo porcine kidney model.
Materials and Methods
Experimental instruments
Experimental instruments and a fresh cadaveric porcine kidney with a T-box 11 were used in this study (Fig. 1). A 6F pressure catheter and UASs were inserted to the porcine ureter and sutured tightly; it successfully prevented fluid leakage even though reaching higher IPPs. The tip of the pressure catheter and f-URS were placed into the renal pelvis centrally, and UASs were set on the ureteropelvic junction for all measurements. IPP was measured using the Invasive Pressure Measurement module® (Philips, the Netherlands) connected to a 6F pressure catheter.
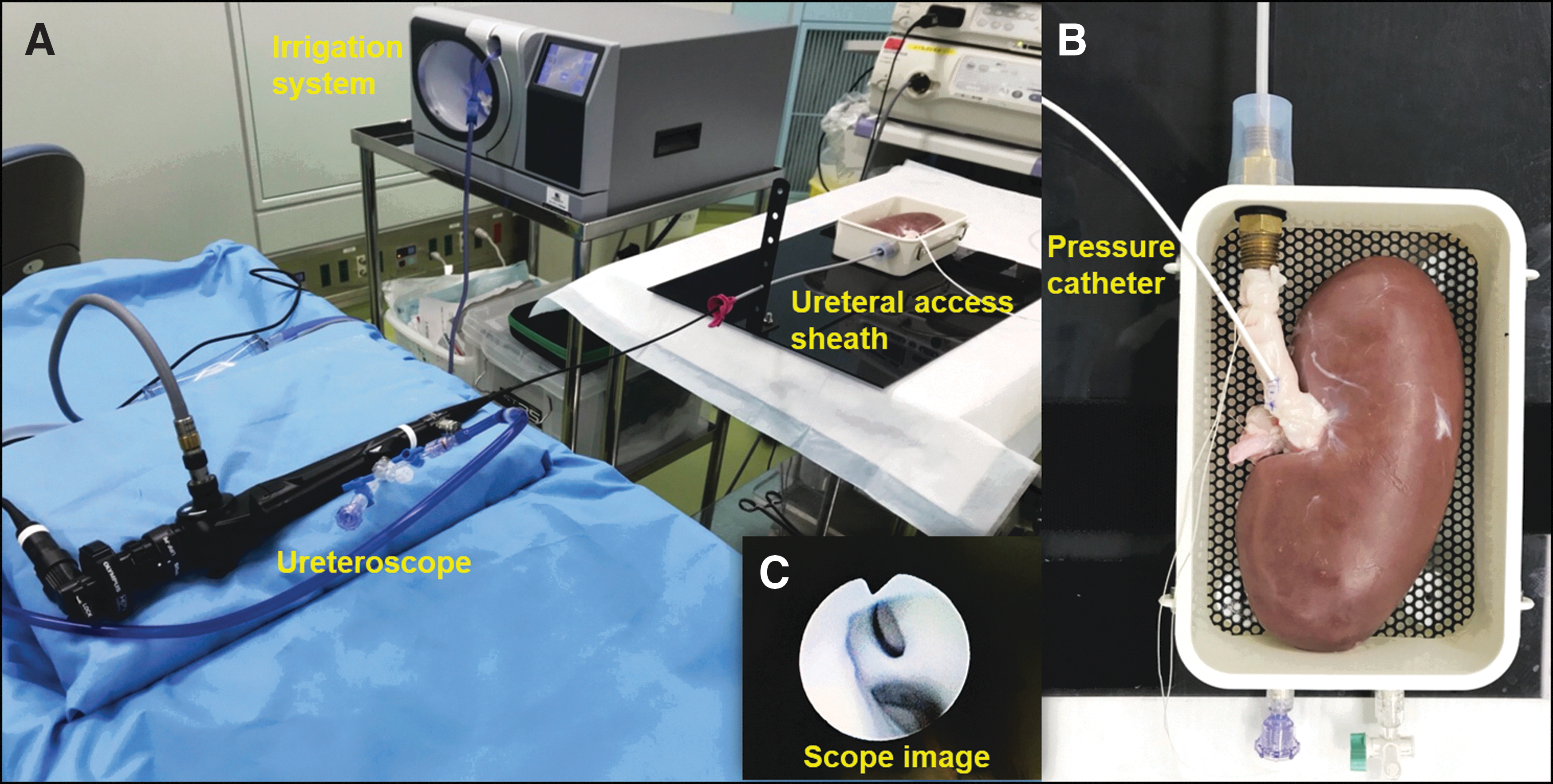
Photographs of study setting. (
For the f-URS, we used the URF-P6® (Olympus, Japan), which is the thinnest optical f-URS currently available, 10 and Endoflow II with the Traxer-Flow irrigation system (Rocamed, Monaco) to achieve a steady continuous irrigation pressure Fig. 1). We tested five different commercially available UASs, including the 9.5/11.5 F Flexor® (Cook Medical), 10/12 F ReTrace® (Coloplast, Denmark), 10/12 F Bi-Flex® (Rocamed), 10/12 F Proxis® (BARD), and 10/12 F UroPass® (Olympus, Japan). 12
Evaluation
For the five UASs, the diameters of the UAS, including the inner, outer, and thickness diameters ( = outer−inner diameters), were measured with a digimatic caliper (ABSOLUTE™; Mitutoyo, Japan). These diameters could be measured up to 0.01 mm. To minimize technical errors, we measured each UAS three times and the mean value was used.
Maximum IPP was measured at the time of reaching its plateau. Pressure values were measured in mm Hg and multiplied by 1.3595 to calculate the values in cm H2O. The IOF rate (mL/second) was simultaneously recorded through the gap between the f-URS and UAS for 20 seconds after reaching the plateau of IPP. This sequence of tests was repeated three times for each combination of UAS and irrigation flow pressure (40, 60, 80, 100, 120, 140, 160, and 180 mbar) (1 mbar is equal to 1.0197 cm H2O).
Statistical analysis
The data are presented as mean values. Comparison of measurement values was performed using Welch's t-test. Correlations between data were evaluated with Spearman's rank correlation test. All statistical analyses were performed using SPSS® version 21.0 (SPSS IBM, Armonk, NY). A two-sided p-value of <0.05 was considered statistically significant.
Results
Characteristics of UASs
The characteristics of UASs and ureteroscopes are shown in Table 1. The 9.5/11.5F Flexor had the smallest outer diameter of UAS compared with that of the other UASs (all p < 0.05). The 10/12F UroPass had the largest outer diameter among the other 10/12F UASs. The 10/12F UroPass had a significantly larger outer diameter than that of the 10/12F Bi-Flex (p < 0.05).
Characteristics of Ureteral Access Sheaths and a Flexible Ureteroscope Used in the Study
Data of UASs are shown as mean values.
UASs = ureteral access sheaths.
The 9.5/11.5F Flexor had the narrowest inner diameter of UAS compared with that of other UASs (all p < 0.05). The 10/12F UroPass had the widest inner diameter compared with that of other UASs (all p < 0.05). The 10/12F Proxis had a significantly narrower inner diameter than that of the 10/12F UroPass (p = 0.011) and 10/12F Bi-Flex (p = 0.024), but had a comparable inner diameter with the 10/12F ReTrace (p = 0.074).
Maximum IPP
The IPP of each UAS and irrigation pressure are shown in Figure 2 and their comparisons are shown in Table 2. The 10/12F UroPass and 10/12F Bi-Flex provided IPP below the limit for intrarenal reflux, which is considered as 40 cm H2O, 13 at all irrigation pressures. However, the 9.5/11.5F Flexor, 10/12F Proxis, and 10/12F ReTrace provided such an IPP at an irrigation pressure of 60, 120, and 120 mbar or less, respectively.
Comparison of Intrapelvic Pressure for Each Ureteral Access Sheath and Irrigation Pressure
Data are shown as mean values.
Bold font indicates significant p-values.
Comparison was performed using Welch's t-test.
IPP = intrapelvic pressure.
The 9.5/11.5F Flexor had a significantly higher IPP at all irrigation pressures (all p < 0.01) and the 10/12F ReTrace had a lower IPP at ≥60 mbar (p < 0.05) compared with the 10/12F Proxis. The 10/12F UroPass and 10/12F Bi-Flex had a significantly lower IPP than that of the 10/12F Proxis at all irrigation pressures (all p < 0.01). However, the IPP of the 10/12F UroPass was significantly higher than that of the 10/12F Bi-Flex at only 40 mbar (p < 0.05) (Table 2 and Fig. 2).
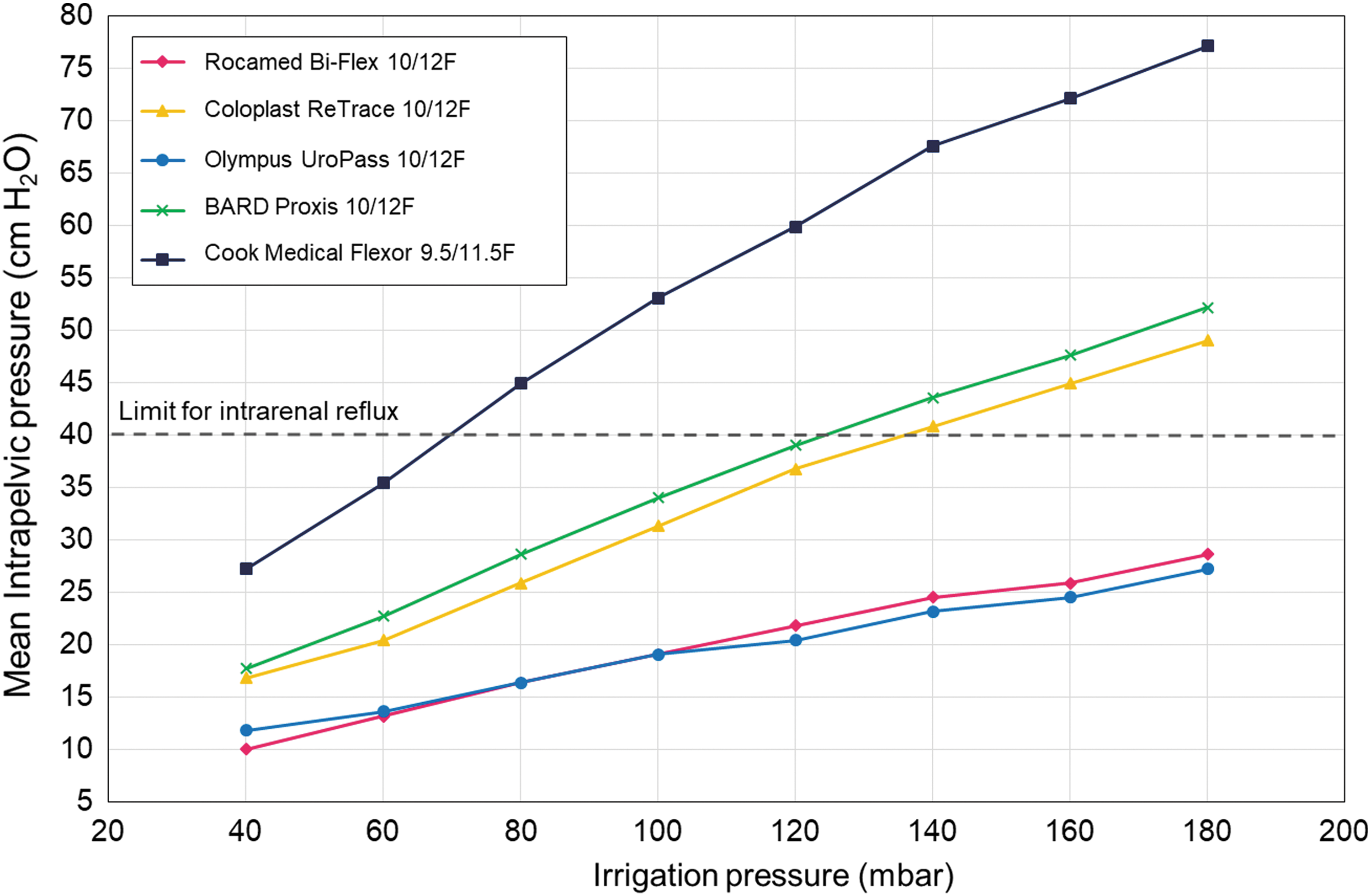
Graph showing intrapelvic pressure for each ureteral access sheath and irrigation pressure.
IOF rate at the plateau of IPP
The 9.5/11.5F Flexor had a significantly lower IOF rate at all irrigation pressures compared with the 10/12F Proxis (all p < 0.05). However, the 10/12F UroPass and 10/12F Bi-Flex had significantly higher IOF rates at all irrigation pressures compared with the 10/12F Proxis (all p < 0.05). The IPP of the 10/12F UroPass was significantly higher than that of the 10/12F Bi-Flex at only 40 mbar (p < 0.05) (Fig. 3).
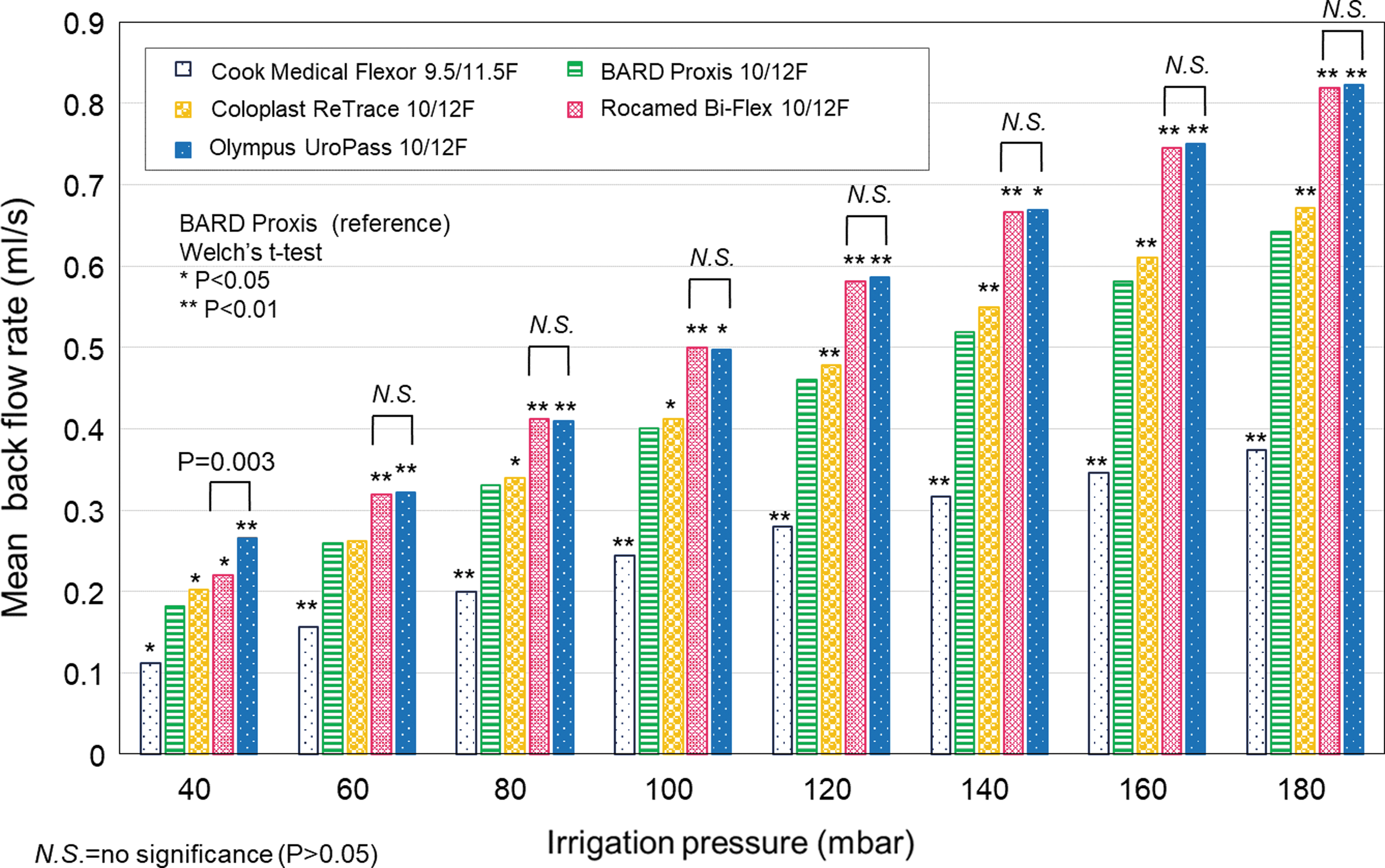
Bar graphs of the mean back flow rate at the plateau of intrarenal pressure.
Correlations between characteristics of UASs and IPP
Finally, we investigated the correlations between properties of UASs and IPP at irrigation pressures of 40, 100, and 180 mbar. The inner diameters of UASs were significantly correlated with IPP (all p < 0.05). However, the outer diameter was not associated with IPP at 40 and 100 mbar irrigation pressures (p = 0.154 and p = 0.091, respectively).
Discussion
In this study, we evaluated characteristics of five different five UASs of ≤10/12F and their differences in IPP and IOF rate using the ex vivo porcine kidney model. The 9.5/11.5F Flexor had the thinnest UAS among the other UASs, and it recorded the highest IPP of 77.1 cm H2O. Among 10/12F UASs, the 10/12F UroPass and 10/12F Bi-Flex could significantly maintain a lower IPP under any irrigation pressure compared with the 10/12F Proxis and 10/12F ReTrace. Similar to IPP, the 10/12F UroPass and 10/12F Bi-Flex had significantly higher IOF rates than that of the other UASs at all irrigation pressures. Finally, the degree of IPP was correlated with the degree of inner diameter. This is the first report to evaluate characteristics of different UASs of <10/12F in terms of their IPP and IOF rate at several irrigation pressure settings.
In 1974, two Japanese surgeons, Hisao Takayasu and Yoshio Aso, developed the UAS to facilitate insertion of a ureteroscope in the ureter. 14 Since this time, along with technological advancements of the f-URS, UASs have been widely used and newly developed with various characteristics, including various lengths, diameters, materials, dilator tip design, and stiffness. 12 To date, no standard criteria regarding how to select the appropriate UAS for each patient have been established, and determining the type of UAS during RIRS depends on the surgeon's discretion. 15 With regard to the size of the UAS, 12/14F UASs are commonly used for RIRS. However, 12/14F UASs can only be passed in 22% of patients because of ureteral narrowing and there is also the concern of UAS-related ureteral injury. 5,16 Therefore, to determine more ideal UASs, accumulative evidence of features of smaller-sized UASs is required for their safe and effective use.
Recently, studies on the combinations of different UASs and ureteroscopes have been published. Al-Qahtani and coworkers 17 established correlation tables with 21 different UASs and 12 different ureteroscopes. These authors found that the 9.5/11.5 Flexor could be inserted only by using the URF-P6 (Olympus) and Flex-X 2 (Storz, Germany). Another study that used eight different f-URSs and five different UASs with an irrigation pressure of 60 cm H2O showed that only the combination of the 9.5/11.5F Flexor and URF-P6 provided an IPP below 40 cm H2O. 10 According to these evidence, the 9.5/11.5F Flexor should be used along with the thinnest f-URS, URF-P6, for protection of the f-URS, and avoiding postoperative complications related to a high IPP. Our study showed that the 9.5/11.5F Flexor-URF-P6 combination setting showed an IPP >40 cm H2O with an irrigation pressure of ≥80 mbar Fig. 2). Therefore, to maintain an IPP of <40 cm H2O when using the 9.5/11.5F Flexor, intermittent removal of the f-URS from the UAS or suction of irrigated solution via the channel of f-URS may be required during RIRS.
Al-Qahtani and coworkers 17 speculated that 10/12F UASs would become the new standard UAS that accepts all endoscopes with a low friction rate. Sener and associates 10 suggested that 10/12F UASs have advantages in terms of IPP and IOF compared with other UASs. We agree with these authors, and have added further information regarding 10/12F UASs as follows. First, the 10/12F Proxis tended to have a higher IPP because of the small inner diameter compared with other 10/12F UASs. Second, the 10/12F Proxis and 10/12F ReTrace showed >40 cm H2O IPP when we used an irrigation pressure of ≥140 mbar. Finally, the 10/12F UroPass and 10/12F Bi-Flex could be safely used under any irrigation pressure, but the 10/12F UroPass had the largest outer diameter compared with the other UASs. Therefore, for preventing UAS-associated ureteral injury and excessive IPP, the 10/12F Bi-Flex might be close to the ideal UAS because it has a small outer diameter with a large inner diameter among ≤10/12F UASs.
Our study has some limitations. One limitation is that we only used one type of ureteroscope with a free working channel. Although there are many commercially available surgical devices with a wide range of diameters, such as ureteroscopes (4.9–10.1F), laser fibers (200–356 μm), and baskets (1.2–3.0F), 1 for the purpose of this study, we considered that we should only focus on UAS characteristics with the simplest study design and easily understood features. In the clinical setting, surgeons may use a hand-pump irrigation system, and not use an automated irrigation system, as we used in this study. However, hand-pump irrigation may create several ranges in irrigation pressure. 18 Therefore, our results could be useful for knowledge of the correlations between features of UASs, actual IPPs, and several irrigation pressures for hand-pump users. There might be a difference between ex vivo and in vivo models, and potential flow of irrigation solution between the ureter and the UAS in an in vivo study. Finally, we could not evaluate UAS-related injury. Therefore, this study was insufficient for indicating the best UAS. Further investigations in the in vivo setting are required in the future.
Conclusions
The 9.5/11.5F Flexor is the thinnest UAS, and may be better for preventing UAS-associated ureteral injury. However, surgeons need to be aware that the 9.5/11.5F Flexor shows excessive IPP during RIRS. Our study suggests that the 10/12F UroPass and 10/12F Bi-Flex can provide a safe IPP and good IOF rate under any irrigation pressure, and may be the first-line choice among ≤10/12F UASs.
Footnotes
Author Disclosure Statement
No competing financial interests exist.