
Abstract
Introduction and Objectives:
Retrograde urethrogram (RUG) and voiding cystourethrogram (VCUG) are currently the gold standard imaging technique for diagnosis of urethral stricture and determination of stricture location. However, RUG and VCUG have multiple limitations. These techniques require exposure to ionizing radiation, the quality is operator and patient dependent, there is a moderate degree of invasiveness with urethral catheterization, can have artifacts because of patient positioning that underestimates stricture length. The development of novel imaging modalities without ionizing radiation to accurately evaluate the presence, location, length, and lumen cross-sectional area (CSA) of the urethral stricture would be of great value. The objective of this study was to develop a novel endoluminal ultrasound (ELUS) imaging technique that permits the accurate quantitation of urethral stricture.
Methods:
Urethral strictures were created in rabbits (n = 5) by electrocautery and an ELUS technique was developed for subsequent luminal imaging. A 3.2F 40 MHz ultrasound (US) probe was introduced transurethrally and infused with US contrast agent. Images were recorded as the catheter was pulled back at a constant speed to acquire tomographic images. Lumen CSA over the entire urethral length was calculated using a custom methodology and validated in our laboratory.
Results:
Urethral luminal CSA over the entire length of urethra before and after experimental stricture development was quantified including the length of stenosis. Intra- and interobserver variability (r = 0.99 for both) was excellent.
Conclusions:
Feasibility of ELUS as a quantitative technique to determine healthy urethral lumen and stricture CSA was demonstrated. The translational potential for a nonionizing imaging modality to better describe CSA, length, location, and uninvolved urethral CSA of the stricture is a significant improvement over current methodology.
Introduction
U
The current modalities of stricture work-up have multiple limitations. Urethroscopy facilitates visualization of the distal extent of stricture location but cannot comment on stricture length. RUG by itself cannot comment on the length of the stricture but when used in tandem with VCUG the length can be estimated. At minimum, VCUG necessitates urethral catheterization through a stricture and may necessitate placement of a suprapubic tube with tight or dense strictures. Both RUG and VCUG necessitate ionizing radiation to the patient, technologist, and urologist. 3 In addition, both RUG and VCUG show two-dimensional images that could lead to underestimation of stricture length and severity based on patient positioning. 2
Urethral ultrasonography by transscrotal or transperineal approach has been explored as an adjuvant to RUG to characterize penile and bulbar urethral strictures. 3 –8 These approaches are not intraluminal and cannot comment on the distended urethral diameter as would occur in voiding. Development of a minimally invasive and reproducible endoluminal technique to evaluate and monitor stricture disease would be useful in both the diagnostic and postsurgical follow-up phases. In this study we developed and validated a novel, quantitative, reproducible endoluminal ultrasound (ELUS) imaging technique in a rabbit model.
Materials and Methods
The institutional animal care and use committee at the VA San Diego Healthcare Systems approved the study protocol and all experiments were conducted in accordance with the Guide for the Care and Use of Laboratory Animals (National Institutes of Health, Bethesda, MD).
Stricture creation
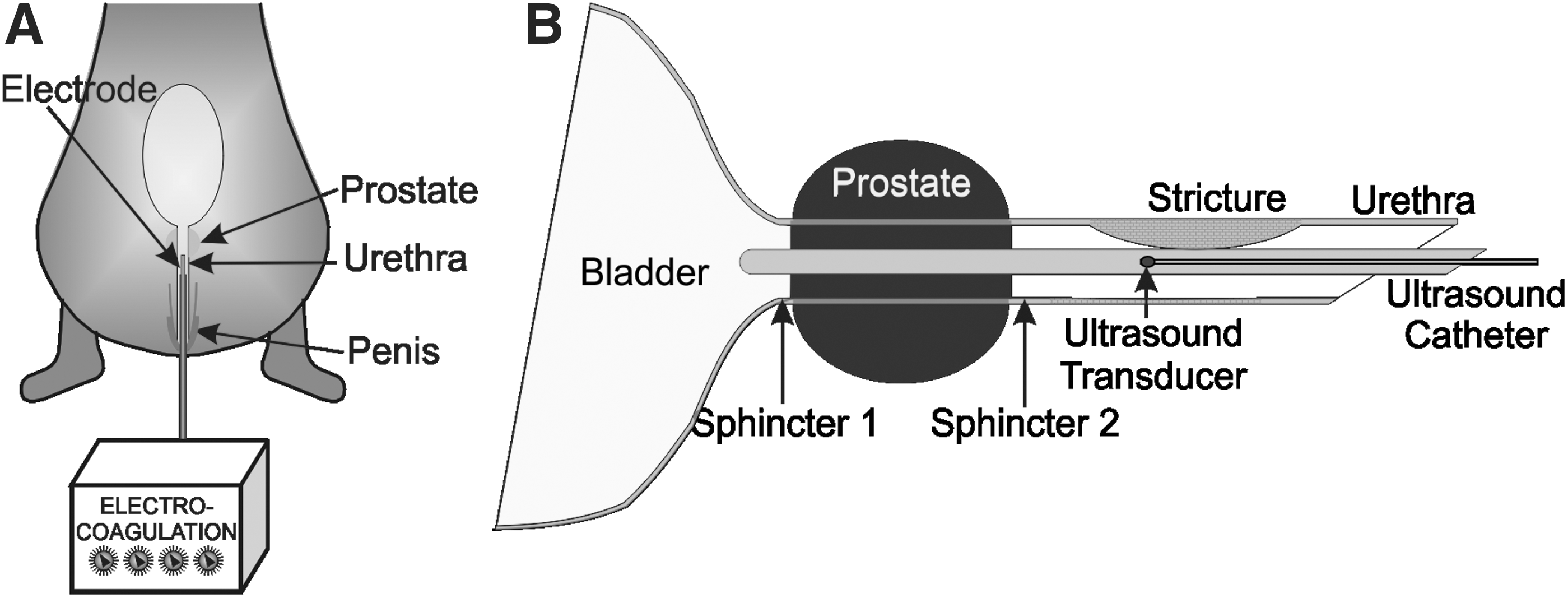
New Zealand white male rabbits (n = 5) weighing 3 to 4 kg were anesthetized with an intramuscular injection of ketamine (35 mg/kg) and xylazine (5 mg/kg). An intravenous catheter was placed in the ear vein for maintenance of anesthesia. Experimental urethral strictures were created in 10 seconds by transurethrally administered electrocautery (50 W, 600 Hz) at two points 5 cm from the urethral meatus 1 cm apart from one another (Fig. 1A). 9
Stricture evaluation with RUG
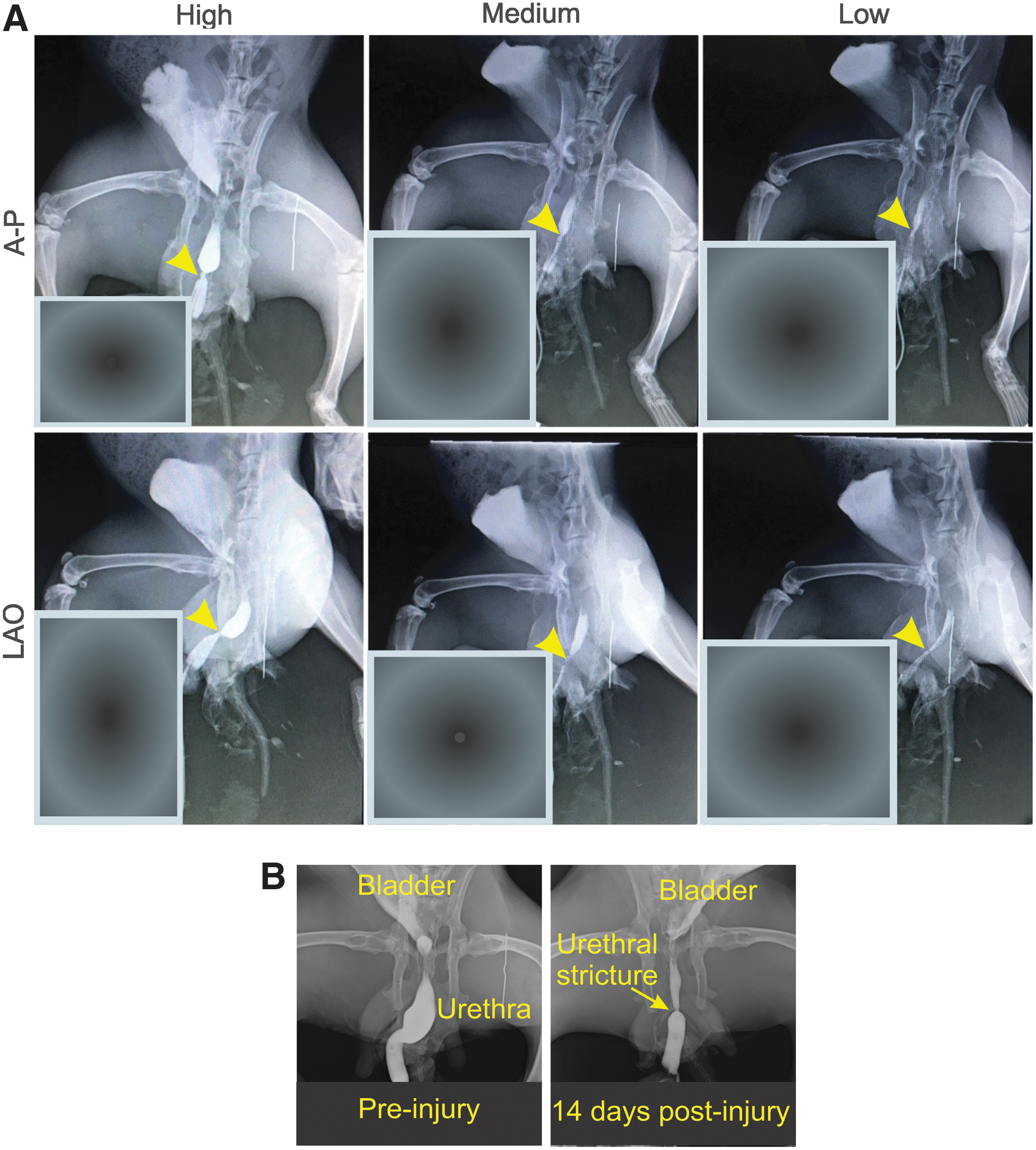
Rabbits were placed in the supine/anterior-posterior (AP) or left anterior oblique (LAO) position and the area around penis was prepped with betadine. To test the impact of contrast pressure, RUG was performed by infusing radiographic contrast (Omnipaque) agent into the urethra at low (15 mm Hg), medium (25 mm Hg), and high (40 mm Hg) pressures. Urethral pressure was monitored using a 3.2F Millar solid state pressure transducer placed in penile urethra that was attached to the ultrasound (US) contrast infusion line and by capturing radiographic images in AP and LAO projections. Optimal images were generated using standard clinical RUG approach for evaluation before and 14 days after mucosal injury. A radiopaque marker was placed in the imaging field for image calibration and to estimate stricture severity.
Endoluminal ultrasound
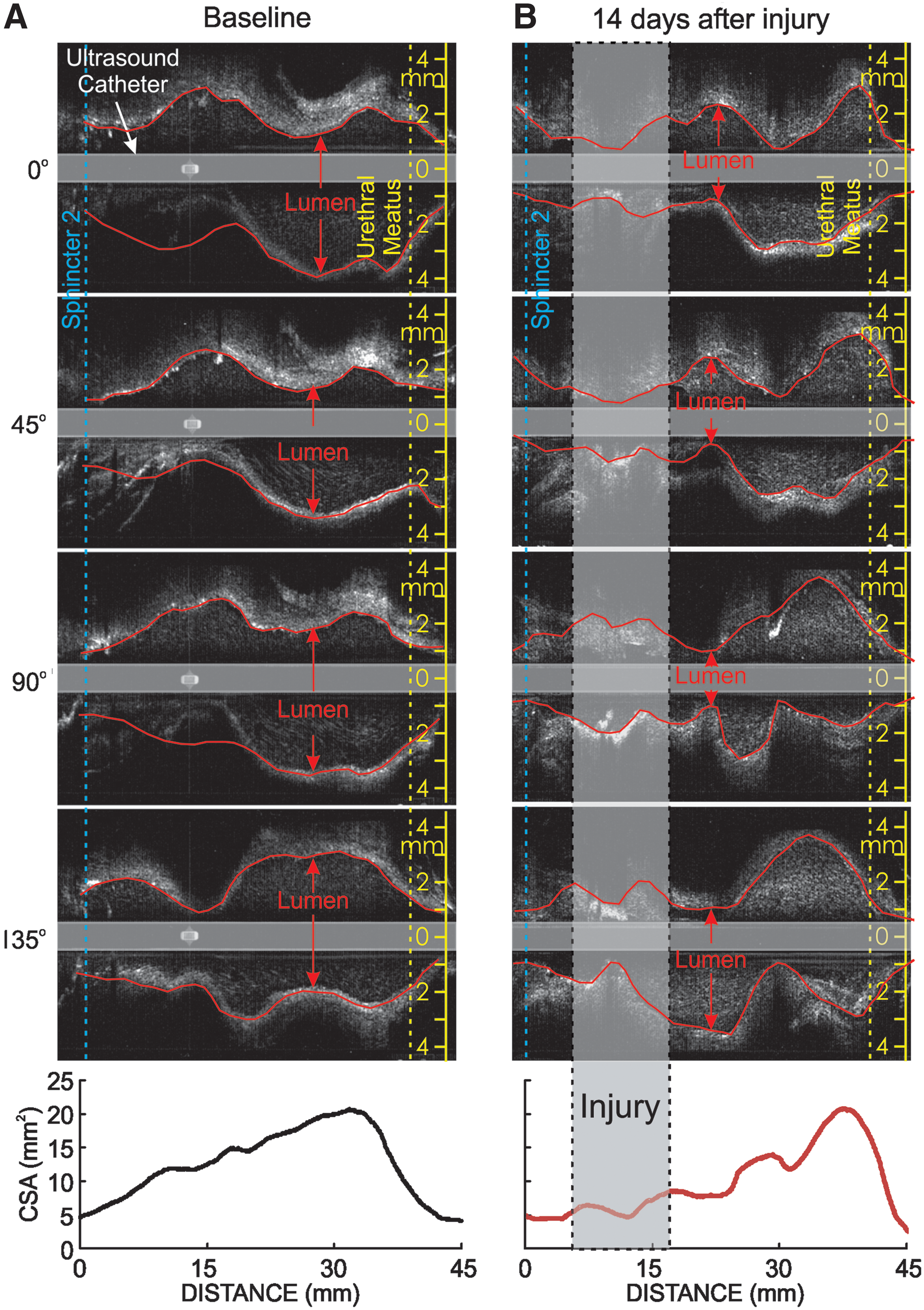
A 5F open-end feeding tube was inserted into the urethra and a 3.2F 40MHz intravascular ultrasound (IVUS) probe (Opticross 6; Boston Scientific Corporation) was introduced transurethrally into the bladder through the feeding tube (Fig. 1B). After US probe placement the feeding tube was removed over the probe. US contrast agent (Definity, perflutren lipid microsphere) was infused to distend the urethra. Urethral pressure was monitored, and excess contrast was aspirated to decrease the urethral pressure to 10 mm Hg. This was performed to maintain a constant pressure during all imaging sessions allowing us to serially compare normal and stricture segment dimensions. Digital 360° cross-sectional or tomographic images were recorded as the US probe was pulled back at 0.5 mm/s (Boston Scientific iLab). ELUS images were obtained at baseline and 14 days postinjury. Four equispaced longitudinal images, 45° apart, were generated, temporally aligned, and luminal edges digitized using commercially available image analysis software (Sigma Scan Pro) (Fig. 2A). Luminal CSA was calculated using a previously created and validated methodology 10 (Fig. 2B, C).

Analysis
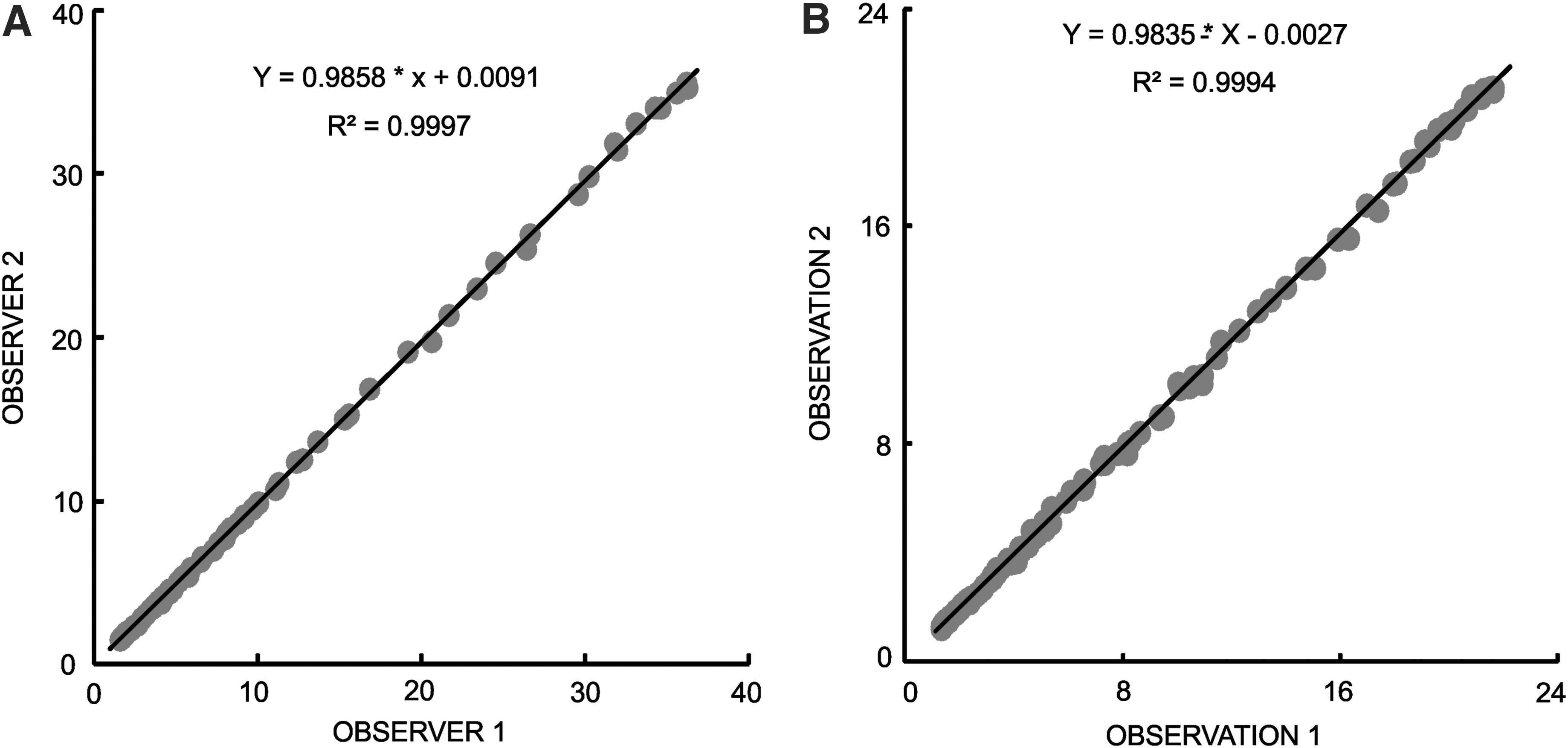
In brief, in each M-mode image derived from the tomographic images, the radial distance between the center of the image (US catheter center line) and the outer luminal edge was determined. 10 Area of the triangular region encompassed by the two adjacent radial lines was calculated (area = 0.5 × R1·R2·sin 45°, where R1 and R2 are two adjacent radius and the angle between the two radial lines is 45°; Fig. 2B). Total lumen CSA was obtained from the sum of the eight triangular areas at each location in the urethra (Fig. 2B). For inter- and intraobserver variability estimation, luminal CSA was determined by two different observers (R.B. and A.C.) and twice by the same observer (R.B.) a week apart on data acquired 14 days after injury.
Statistical analysis
Luminal CSA between two observers (interobserver variability) and of the same observer twice (intraobserver variability) was compared using linear regression analysis. Linear regression analysis was performed on urethral lumen CSA for the entire urethral length from two sets of measurements.
Results
RUG optimization
Figure 3A shows the impact of contrast agent pressure on RUG. At low-contrast pressure (right panels) stricture severity (degree of stenosis) was greater and longer stricture length was likely because of distention of the normal segment. In LAO projection, because of foreshortening, the lesion severity seems to be less than in AP projection for high pressure. In Figure 3B is given RUG images acquired both before and at 14 days postinjury in AP projection.
(
Quantitation of stricture severity by RUG and ELUS
Representative RUG images are given in Figure 3B and ELUS images in Figure 4. US images from all five animals showed a reproducible reduction in lumen CSA in the region of urethral injury. In Figure 4A and B is given the urethral luminal CSA of a rabbit over the entire length before and after experimental stricture development (Fig. 4A baseline; Fig. 4B, 14 days after injury) US images and the corresponding CSA plots are given at the bottom of the figure. Plots show reduction in luminal CSA in panel B (shown in the gray shaded region) where the urethral injury was created. This plot shows a reduction of luminal CSA by 62% at the injury site (gray shaded region) and lesion length of 5 mm. The stricture length was calculated by estimating the length where the CSA is smaller than that at baseline.
Longitudinal US images at
Inter- and intraobserver variability
Figure 5A shows the interobserver variability and Figure 5B the intraobserver variability. Both analyses yielded an excellent correlation coefficient as given in Figure 5A and B, respectively (r > 0.99). These analyses produced a slope of 0.986, 0.984 and an intercept of 0.01, −0.003 respectively, suggesting that the method is reproducible.
Discussion
A high-resolution IVUS catheter and contrast agent were used to longitudinally image the entire urethral luminal CSA allowing characterization of normal urethral diameter and induced stricture diameter and its length. There was strong inter- and intraobserver reproducibility for this technique. CSA quantitation of normal urethral and urethral stricture segments represents a tremendous translation potential for future clinical applications.
At present, RUG and VCUG are commonly used clinically to diagnose urethral strictures and to determine stricture location and severity. 1 RUG limitations include poor definition of detail, variability of stricture parameters because of patient orientation, image projection, and the risks of ionizing radiation. Because of projection-related problems (orientation and foreshortening), RUG may lead to erroneous and inaccurate estimation of stricture severity. 11 VCUG necessitates either suprapubic tube placement or urethral catheter placement and the quality of the images are operator and subject dependent. An adequate voiding effort for bladder neck opening is required but variably accomplished to define the proximal extent of the stricture.
Urethral ultrasonography has traditionally been performed by transpenile or perineal approaches. 4,8 This technique avoids ionizing radiation and may be more accurate than RUG. For penile ultrasonography a 5 MHz transducer is placed to the dorsum of the penile shaft, and the urethral lumen is distended with retrograde instillation of saline (unknown pressure). The areas of stricture are observed based on inelasticity as compared with healthy urethral tissue, which is easily distensible. However, this technique seems to be ideal for imaging bulbar urethra but determination of entire stricture length is not feasible. This method is operator dependent and may be influenced by the probe pressure, probe angulation, and saline pressure similar to RUG. ELUS methodology, in contrast, can image the entire luminal length and provide 360° cross-sectional image of the urethral lumen with well-observed urethral wall edges. This method has enabled us to determine luminal CSA, which is a direct quantitative measure of luminal constriction consequent to stricture/fibrosis and permits serial assessment of disease progression.
ELUS approaches using IVUS catheters have been used safely with reliable luminal coronary artery CSA quantitation for more than three decades. In cardiac interventional procedures IVUS has the unique ability to provide real-time, high-resolution tomographic and longitudinal images of a vessel lumen. 12 IVUS can estimate CSA and diameter more accurately than quantitative coronary arteriography. 13 This approach has also been used to assess esophageal luminal CSA and esophageal muscle wall thickness. 14,15 However, the ELUS approach using IVUS catheters has never been used to assess urethral strictures and represents an exciting opportunity to gather more accurate and safer diagnostic information.
Conclusions
In summary, our findings prove the feasibility of ELUS as a viable minimally invasive technique to determine urethral luminal CSA and stricture length. This imaging technique has several advantages over RUG such as: (1) reduction in establishment costs of the imaging equipment, (2) elimination of need for a lead-lined radiographic room and a highly trained radiographer, and (3) prevention of potential untoward effects of radiographic contrast agents. Thus, our novel ELUS method presents translational potential for future clinical applications without exposure to ionizing radiation.
Limitations of our study include use of a high-frequency (40 MHz) IVUS catheter that produces reproducible high-resolution images but unfortunately does not provide large depth of field. The US machine (Boston Scientific) that we used in this study does not provide the degree of spongiofibrosis, a critical stricture characteristic, to best choose surgical technique and counsel patients on potential outcomes. However, there are other IVUS machines (Volcano Therapeutics) that can provide some of these details.
Footnotes
Acknowledgments
The research was supported in part by the Department of Veterans Affairs, Veterans Health Administration, Rehabilitation Research and Development Service. Award, 1I01RX001694-01A2, to M.R.R., and VA San Diego Healthcare System. This work was supported in part by a UCSD academic senate grant (J.C.B.) and by a VA Rehab R&D Merit Award.
Authors' Contributions
Study concept and design (M.R.R., V.B.), acquisition of data (H.Y., R.B., A.C., H.S.Y., J.K., S.Y., S.R.L.), analysis and interpretation of data (R.B., A.C., M.R., V.B.), drafting of the article (M.R., V.B.), critical revision of the article for important intellectual content (J.B., T.W.F., M.R., V.B.); statistical analysis (M.R., R.B., A.C., V.B.), funding support (M.R.).
Author Disclosure Statement
No competing financial interests exist.