
Abstract
Purpose:
To evaluate the feasibility and effectiveness of the navigation of intelligent/interactive qualitative and quantitative analysis (IQQA) three-dimensional (3D) reconstruction technique in laparoscopic or robotic assisted partial nephrectomy (LPN or RAPN) for renal hilar tumors.
Patients and Methods:
The study retrospectively reviewed 26 patients with hilar tumors from February 2016 to February 2018. IQQA 3D reconstruction technique was applied for the purpose of navigation and resection of the tumors. Relevant clinical parameters and surgical outcomes were recorded.
Results:
All 26 LPN or RAPN were effectively completed without conversion to a hand-assisted or an open approach. Under the navigation of IQQA, all tumors were found precisely at the first time during surgeries. The mean operative time was 142 minutes (142 ± 35), with a mean warm ischemia time of 24.3 minutes (24.3 ± 9.5). The estimated blood loss was 156 mL (156 ± 112). No intraoperative complications occurred. Two patients suffered from postoperative complications. All patients had negative margins on the final pathological examination. At a mean follow-up period of 3 months, the mean glomerular filtration rate is 22.5 mL/min (22.5 ± 7.1) without tumor recurrence.
Conclusions:
With peculiar features, such as accurate location, complete resection, and fewer perioperative complications, the navigation of IQQA 3D reconstruction technique in partial nephrectomy represents a safe and effective procedure for hilar tumors.
Introduction
With the development of modern medical technology, more and more renal tumors are diagnosed at early stage. 1 Partial nephrectomy has been recommended by many official guidelines as gold standard for the treatment of T1a renal tumors, 2,3 as it confers ideal tumor control while reducing the risk of progression to chronic renal disease. 4 Compared with open nephron sparing surgery (NSS), laparoscopic or robotic assisted partial nephrectomy (LPN or RAPN) is less traumatic to patients and shortens postoperative recovery time; these advantages make them more and more popular. 5,6 However, renal hilar tumor has a unique anatomy, that is, it is close to renal pedicle vessels. This makes it difficult to excise renal hilar tumors laparoscopically and confers high risk of perioperative complications. 7,8
Recent advances in imaging technology, such as imaging-guided precision surgery, have brought new ideas and methods for laparoscopic management of renal hilar tumors. Intelligent/interactive qualitative and quantitative analysis (IQQA) three-dimensional (3D) reconstruction technique is based on preoperative CT/MRI images of the patient. Remote real-time interactive preoperative evaluations were done through IQQA cloud platform and delicate operation plans were made. Surgeries were done accordingly. In our study, 26 renal hilar tumor patients were treated using this technique with satisfactory results. In this study we present our preliminary experiences with this novel surgical navigation technique.
Patients and Methods
Study population and clinical information
After institutional review board of the Second Military Medical University approval, 26 patients with renal hilar tumors who underwent LPN or RAPN by a single surgeon (B.Y.) at a single tertiary care center (Changhai Hospital, Shanghai, China) between February 2016 and February 2018 were enrolled in this study. The inclusion criteria is renal hilar tumor ≤4 cm or renal hilar tumor >4 cm with compromised contralateral renal function. The detailed clinical information is summarized in Table 1.
Demographic Data
GFR = glomerular filtration rate.
IQQA 3D reconstruction technique
The software used in this study for preoperative 3D reconstruction and virtual treatment planning is a commercially available system, IQQA 3D software (cleared by the US FDA and China CFDA, by EDDA Technology, Inc., Princeton, NJ). It provides tools for automated segmentation of renal structures from multidetector computed tomography (MDCT), 3D reconstruction of segmented renal anatomy, display of the reconstructed 3D model, and the corresponding overlay views of the 3D model on two-dimensional (2D; including on original Digital Imaging and Communications in Medicine [DICOM] axial) for user confirmation and local adjustment, geometry analysis of user-selected renal vascular branch based on user-confirmed segmentation of renal vascular tree, user-adjusted tumor margin in 3D, and user-defined virtual cutting surface in 3D and 2D. In using the system, 3D technical first checks and adjusts automated segmentation results, then reviews together with surgeon for his confirmation and further planning.
All patients received computed tomographic angiography (CTA) preoperatively. The original 2D DICOM images are sequentially imported into IQQA-3D analyzing system for preoperative evaluation and virtual treatment planning. The software used supports remote login session, which offers remote real-time interaction between surgeon and technical 3D laboratory staff. Before surgery, surgeon and technical 3D laboratory staff work together interactively for adjustment and confirmation of the 3D model. Finally, a quantitative 3D model was reconstructed, to show the volume, position, and spatial relationship among renal hilar vasculatures, blood supply of the tumor, and so on (Fig. 1). Then, the model was subsequently brought to the operation room (OR) for intraoperative navigation. During the RAPN, the IQQA graphical user interface, including the 3D model, is integrated into the robotic console using the Tile Pro multidisplay input, and displayed with real-time operative video on the same screen. During the surgery, an assistant surgeon drives the software GUI according to the surgeon's command to rotate, show/hide/measure specified anatomy, for the surgeon to view. For the LPN, the GUI is displayed side by side next to the visual monitor of the laparoscopic system.
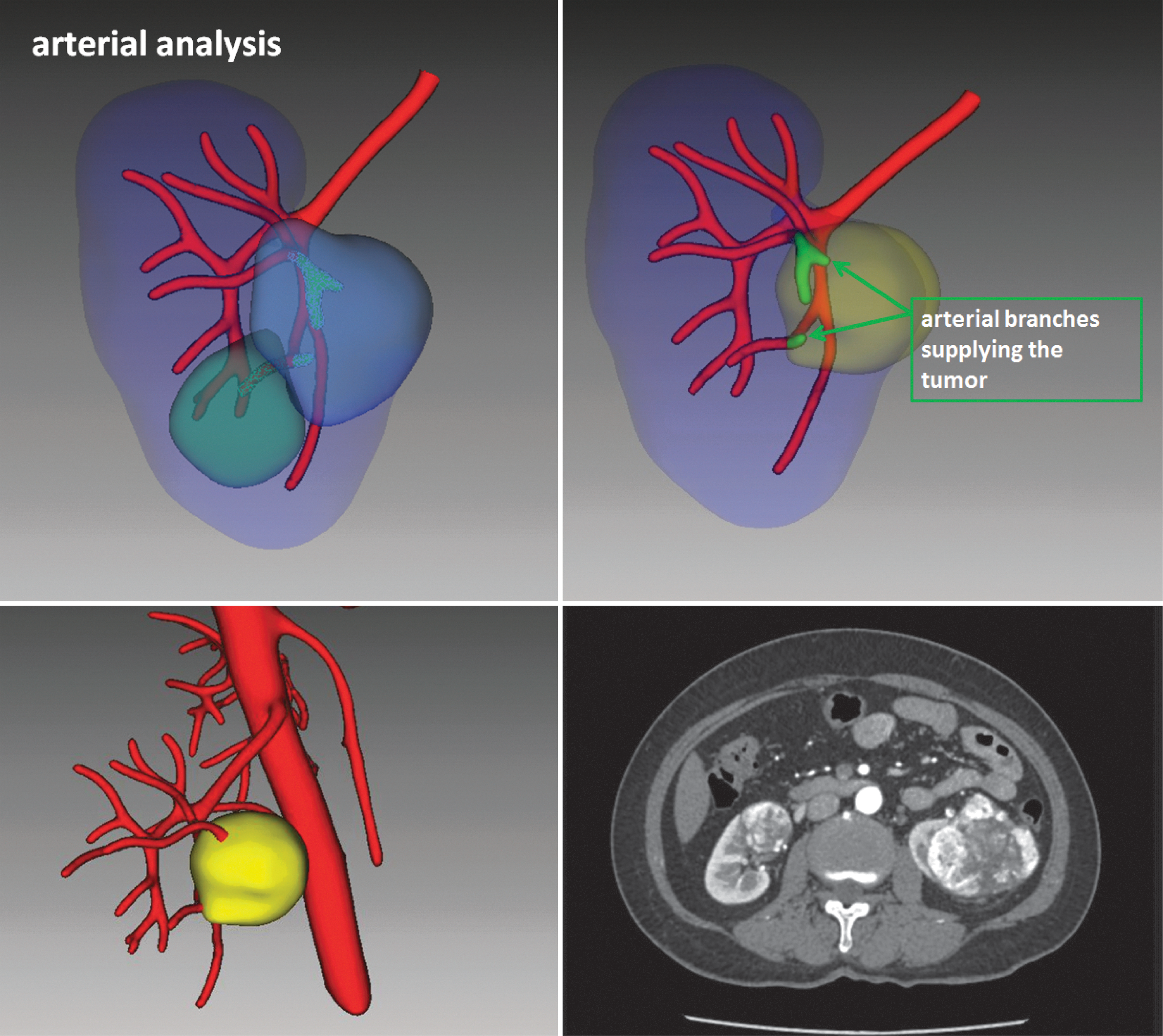
CTA images of the patients were uploaded to IQQA cloud platform. Remote real-time interaction was used for preoperative 3D reconstruction. After preoperative evaluation, tumor size, tumor location, the branch artery supplying the tumor, the relationship between tumor and renal pedicle vessels, and the exact suture points were determined. 3D, three-dimensional; CTA = computed tomographic angiography; IQQA = intelligent/interactive qualitative and quantitative analysis.
Surgical technique
Patients were given general anesthesia and placed in the lateral decubitus position with proper fixation. All operations were done transperitoneally. After inflation of the abdomen, the colon was mobilized medially, the liver or spleen is properly mobilized to expose appropriate surgical field. The ureter is identified at iliac vessel and mobilized ventrally. Continue dissecting along psoas muscle until renal pedicle. Renal artery and vein are properly isolated and marked with a thread around each vessel. Then an “in-depth dissection” of renal hilum is done. Dissection was performed along renal parenchyma to isolate vessels inside renal sinus fat. Dissection went toward tumor base to expose branch vessels and renal hilar structures. Then renal tumor was separated from renal hilar vessels and renal pelvis (Fig. 2a). Perirenal fascia and fatty capsule were then incised to expose renal parenchyma. Dissection went along renal parenchyma to expose tumor margins and ultrasound was used to confirm the margins of the hilar tumors. Renal artery and vein were sequentially clamped using bulldogs. With the navigation of IQQA 3D reconstruction technique, the main segmental vessel (14 out of 26 cases had a main segmental vessel directly supplying the tumor in this study) as well as other branches that supply the tumor were accurately located and the area or volume of tumor as well as normal tissue supplied by each branch artery were calculated. Dissection was then made from main artery to the branch arteries supplying the tumor. And the tumor blood supply arteries were subsequently clipped with small Hem-o-lok (Fig. 3). The renal capsule was incised along the tumor margin and the tumor was excised along the tumor bed in a backward manner from renal hilum toward the normal renal parenchyma. The tumor was excised by sharp and blunt dissection to preserve renal hilar vessels (Fig. 2b). 3-0 barbed suture was used in a “point-to-point” manner to close transected vessels at tumor base and repair injured collecting system. Then a “C” shaped renorraphy was done (Fig. 2c). Renal vein and artery were sequentially unclamped. The surgical field was inspected and no active bleeding was noted. A drainage tube was placed and the tumor was sent for pathological examination. Operation time, warm ischemia time (WIT), estimated blood loss (EBL), perioperative complications, and postoperative renal glomerular filtration rate (GFR) of the impacted kidney on the 3-month follow-up were recorded.
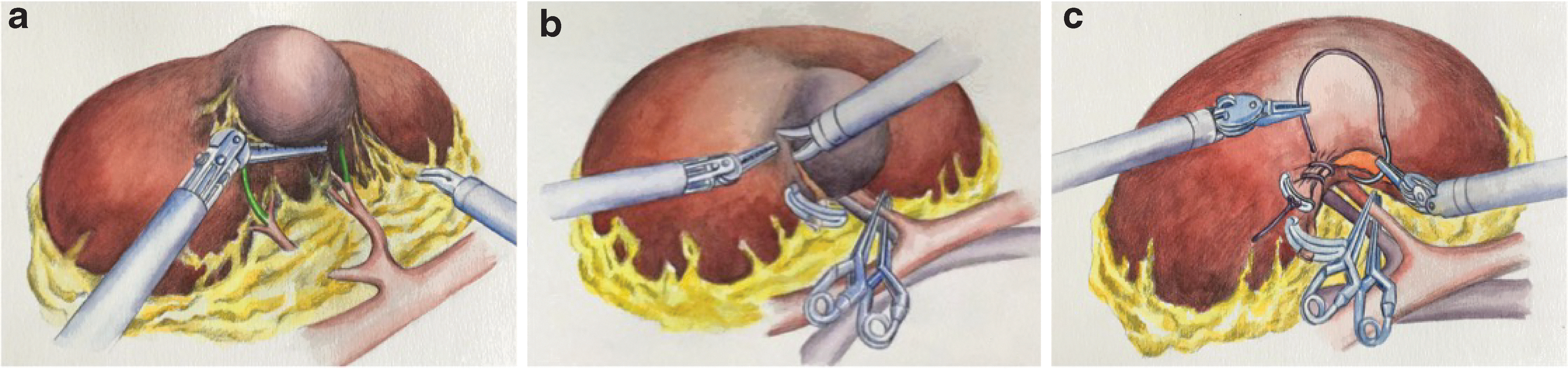
The schematic diagram of IQQA 3D reconstruction technique-guided partial nephrectomy for renal hilar tumors.
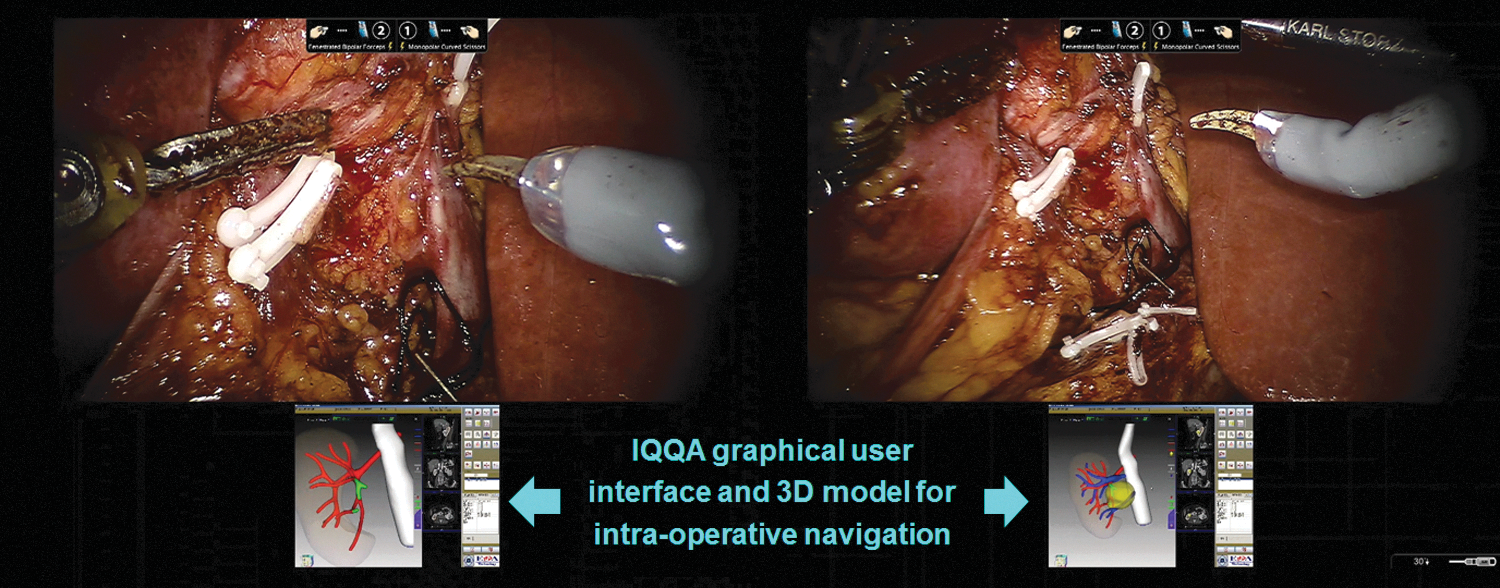
Intraoperative application of IQQA 3D reconstruction technique and location of tumor blood supply vessel.
Results
From February 2016 to February 2018, with the navigation of intraoperative IQQA 3D reconstruction technique, 26 renal hilar tumor patients received minimally invasive partial nephrectomy, including 18 laparoscopic and 8 robotic partial nephrectomies. All operations were effectively performed and all patients were pathologically diagnosed as renal clear cell carcinoma. The mean operative time was 142 minutes (142 ± 35), with a mean WIT of 24.3 minutes (24.3 ± 9.5). The EBL was 156 mL (156 ± 112). For the complications under the Clavien–Dindo classification, 10 patients had grade I complication (6 patients experienced vomiting and were given antiemetics and 4 patients were given analgetics), 2 patients had grade II complication (1 patient experienced gross hematuria probably because of severely damaged pelvis and recovered spontaneously with continuous intravesical instillation and the other patient had a sharp hemoglobulin drop probably caused by oozing of blood in renal wounds and was given blood transfusion), and none of the patients had grade III or higher complication. None of the patients had vascular injury or a positive surgical margin. At the third month follow-up, the average GFR for the diseased kidney is 22.5 mL/min (22.5 ± 7.1) and no tumor relapse or metastasis was noted.
Discussion
NSS is the gold standard for the treatment of stage T1a renal tumors. With the advent of minimally invasive surgery era, laparoscopic partial nephrectomy gradually gains popularity and becomes recommended surgery for stage T1a and some technically viable T1b or T2 renal tumors. 9 Renal hilar tumor refers to renal tumor located <5 mm to renal hilum, regardless of tumor size or exophytic/endophytic location. 7 Renal hilar tumor is very close to renal pedicle vessels, renal arterial branches, and collecting system. These anatomic characteristics greatly increase technical complexity for surgical removal of renal hilar tumor. 10 –12
In 2005, Gill et al. 8 first reported a retrospective study adopting laparoscopic partial nephrectomy for the treatment of renal hilar tumors. In the 25 patients, the average of tumor diameter was 3.7 cm (range 1–10.3 cm), WIT was 36.4 minutes (range 27–48 minutes), EBL was 231 mL (range 50–900 mL), and all patients' surgical margins were negative. This literature proved that laparoscopic partial nephrectomy for renal hilar tumors is viable and safe and established a basis for the wide adoption of endoscopic treatment of renal hilar tumors. In the same year, Reisiger and colleagues 7 reported eight cases with similar results, further validating the feasibility for laparoscopic resection of renal hilar tumors. In 2008, Lattouf and colleagues 13 reported short-term results for renal hilar tumors treated with NSS of 18 patients. The patients were followed up for 26 months (range 1–59 months); no tumor relapse or metastasis was found. In the same year, Rogers et al. 14 first reported a multi-institutional research of 11 patients with renal hilar tumors undergoing robot-assisted NSS, validating the safety and efficacy of robot-assisted NSS in the treatment of renal hilar tumors.
Recently, the Cleveland Clinic retrospectively reviewed 364 patients undergoing robot-assisted NSS, including 70 hilar tumors and 294 nonhilar tumors. Compared with nonhilar tumors, hilar tumors had larger tumor size (3.9 vs 2.6 cm, p < 0.001) and higher R.E.N.A.L scores (58.6% vs 5.4% with high complexity tumors, p < 0.001). Surgeries for hilar tumors were associated with longer operative time (210 vs 180 minutes, p < 0.001), greater WIT (27 vs 17 minutes, p < 0.001), increased EBL (250 vs 200 mL, p = 0.04), and increased incidence of intraoperative conversion to radical nephrectomy (2 vs 0 patient, p = 0.036). However, the technical complexity for renal hilar tumors is still apparently greater than that of nonhilar tumors. 15
Arora and Rogers 16 summarized the keys for NSS in central renal tumors, that is, to maintain good preoperative hydration, achieving adequate exposure of tumor, and the use of intraoperative ultrasound to plan the resection plane, which will greatly benefit the urologists to carry out such complex operations. Recently, Isotani et al. 17 evaluated the feasibility of virtual partial nephrectomy and reported a retrospective study on 20 patients using software support on 3D reconstruction of renal anatomy and virtual surgical simulation. However, the article did not state the then regulatory clearance status of the software used. And in that study, selective clamping was only carried out in 10 out of 20 patients. In our study, we stated clearly how to use the IQQA software and how it worked during the procedure of LPN or RAPN. Another 3D-printing technology for preoperative planning and surgical rehearsal before RAPN was reported. 18 Indeed, authors developed a patient-specific presurgical simulation protocol for RAPN in that study. Meanwhile, the procedure added the complexity of surgery and was somehow time consuming. Unlike this simulation protocol, our study showed that the IQQA software offered remote real-time interactive preoperative evaluations and intraoperative navigating.
In this study, with the support of IQQA, we also modified NSS for renal hilar tumors to lower surgical risks and maximally preserve perirenal structures. In our study, all 26 renal hilar tumors were effectively treated by laparoscopic NSS with the navigation of IQQA 3D image-guided technology. None of the patients had vascular injury or a positive surgical margin. With the assistance of navigation of IQQA 3D reconstruction technique, we present our technical tips and tricks as follows: Preoperative evaluation: the key to maximally preserve renal parenchyma for renal hilar tumor is to make a reasonable surgical plan preoperatively by identifying anatomical structures of the tumor, the relationship among tumor, renal hilar vasculature and collecting system, and the branch artery supplying the tumor. For all 26 patients in our study, the original CTA images were uploaded to IQQA cloud platform and remote real-time interactive preoperative evaluations were done subsequently. Most importantly, the target branch artery supplying the tumor was identified, making the operation well informed preoperatively and the artery precisely located intraoperatively. In-depth dissection of renal hilum: after isolation of renal artery and vein trunk, an in-depth isolation of renal hilar structure adjacent to tumor margins is made. The key is to dissect deep into renal hilum and tumor bed, thereby exposing vital structures fully at renal hilum. In this way, these vital structures at renal hilum are separated from the tumor to the largest extent and the chance to injure renal pedicle is lowered. This lays a foundation for maximal preservation of renal parenchyma. Renal hilar clamping: as renal hilar tumors are close to renal pedicle, excessive venous blood backflow may blur the surgical field if only clamping the renal artery. This will severely hamper excision of the tumor and suture of the wound. In our study, we marked and clamped both the renal artery and vein, providing a blood-free field for the operation and making subsequent key techniques done in a blood-free surgical field. Intraoperative navigating: after reconstructing the tumor and renal hilar structures with IQQA, these images were transmitted into video and taken to the OR. Renal segmental arteries were isolated with the guidance of IQQA intraoperatively. In traditional ways, urologists could only identify second branch of renal artery; however, with the guidance of IQQA, we could identify third branch or even fourth branch of renal artery, thereby precisely clamping only the blood supply artery of the tumor and reduce the risk of hemorrhage. Precise excision of the tumor: traditionally, partial nephrectomy starts from renal parenchyma close to the tumor and the tumor gradually excised, thereby maximally preserving nephron. However, the renal hilar tumor is in a unique location that renal hilar vasculature and collecting system are prone to injury or damage. In our excision, we started from the tumor margin and excised along the tumor bed in a backward manner toward the normal renal parenchyma. In this way, we achieved the goal of maximally preserving nephron and minimally injuring or clamping the branches of renal artery or vein. Meanwhile, the tumor was excised by sharp and blunt dissection. The transected vessels in the tumor bed were accurately clamped using Hem-o-lok clips to lower the risk of hemorrhage and maintain a clear operative field. “C” shaped renorrhaphy: during excision of the tumor, we adopted a “point-to-point” suture technique, that is, to suture only the transected vessels and injured collecting system. In this way, unintentional suturing renal hilar arteries could be avoided, thus preventing further nephron loss. The in-depth dissection of renal hilum could maximally preserve renal hilar vasculature and collecting system, reduce “point-to-point” suture, avoid extensive suturing the wound with a large needle, simplify suture steps, and possibly shorten WIT. No obvious hemorrhage was noted after unclamping the artery.
Therefore, the combination of IQQA 3D reconstruction technique and partial nephrectomy makes NSS for renal hilar tumors safe and viable. Compared with Cleveland Clinic's results, our study had better results in operation time (142 vs 210 minutes), WIT (24.3 vs 27 minutes), EBL (156 vs 250 mL), and so on. However, the results published by Cleveland Clinic included patients between 2006 and 2011, during which time some of the surgeries were still in the pilot phase and the results could be biased.
The study has a few limitations. First, this is a retrospective study that aims to evaluate the safety and efficacy of a new technology, which still lack of a comparison with standard procedure to assess its superiority. Second, only a small sample size enrolled in the study. Consequently, the results might be biased.Thus, a large-scale long-term randomized controlled study needs to be conducted to prove its efficacy and superiority.
Conclusions
With peculiar features, such as accurate location, complete resection, and fewer perioperative complications, the navigation of IQQA 3D reconstruction technique in partial nephrectomy represents a safe and effective procedure for hilar tumors.
Footnotes
Author Disclosure Statement
No competing financial interests exist.