
Abstract
Objectives:
To present our experience of the Detour extra-anatomic stent (EAS; Porges-Coloplast, Denmark) to bypass ureteric obstruction. Use of the EAS is indicated in patients with complex ureteric strictures or malignant disease, where long-term nephrostomy drainage is undesirable.
Materials and Methods:
Between December 2001 and October 2017, 20 Detour EAS were implanted into 13 patients. The primary indication was ureteric obstruction or injury secondary to metastatic malignancy, or from treatment for malignancy. Five patients required bilateral EAS, with two patients having bilateral EAS following initial unilateral insertion. In 11 patients, the stent was inserted into their bladder, with 2 diverted into a double-barreled stoma. The mean age at the time of implantation was 64 years (range: 50–83 years), and the median follow-up was 12 months (range: 1.5–42 months).
Results:
Four patients required stent revision for urinary leaks, and two developed recurrent urinary tract infections in their stent requiring intravenous antibiotics. All EAS continued to drain successfully following treatment or revision. One patient died due to complications from dislodgement of the stent, leading to laparotomy and intra-abdominal sepsis. Seven patients died due to progression of metastatic malignant disease, and the Detour EAS was functioning in all seven at time of death. The remaining five patients are well with functioning Detour EAS.
Conclusions:
The Detour EAS system provides a suitable alternative option for urinary diversion, affording a good quality of life to carefully selected patients with multiple comorbidities and malignant disease.
Introduction
Extra-anatomic stenting, or nephrovesical/pyelovesical stenting, refers to the formation of an alternative passage for urinary drainage from the renal pelvis to the bladder using a tunneled subcutaneous system, bypassing the ureter. Use of an extra-anatomic stent (EAS) is indicated in ureteric strictures where antegrade stenting and retrograde stenting have failed, traditionally requiring a percutaneous nephrostomy for urinary drainage. 1 –3 Other indications include ureteric obstruction, often secondary to malignancy or invasion of the surrounding structures, and disruption of a ureter deemed unsalvageable for repair. 1 EAS has also been used as a last resort in management of transplant ureteric strictures, a complication in renal allografts. Ureteric obstruction can significantly affect graft function. 4 –6
Patients with complex ureteric disease can have two standard ureteric stents inserted through one ureter to ensure maximal patency, and thus allowing urine flow even if one stent becomes obstructed. Stent encrustation is a significant drawback and the need for regular stent replacement under general anesthetic is both undesirable and unsuitable in patients with predisposing comorbidities.
Formation of a subcutaneous ureter has been described as a “safe alternative” to percutaneous nephrostomy. 7 The use of an EAS provides the option to internalize urinary drainage, enabling natural voiding and freedom from external appliances. Long-term use of nephrostomies in patients with ureteric strictures or obstruction is complicated, due to the risk of infection, dislodgement, and hematuria. 8 Furthermore, there are significant detrimental impacts on the social and psychological aspects of patients' lives with external appliances, and the posterior position of a nephrostomy poses a greater challenge for self-care. Conversion of a percutaneous nephrostomy into a pyelovesical bypass using an EAS was associated with a significant improvement in global quality of life. 9
We present our case series using the Detour EAS system (Porges-Coloplast, Denmark).
Materials and Methods
Insertion technique
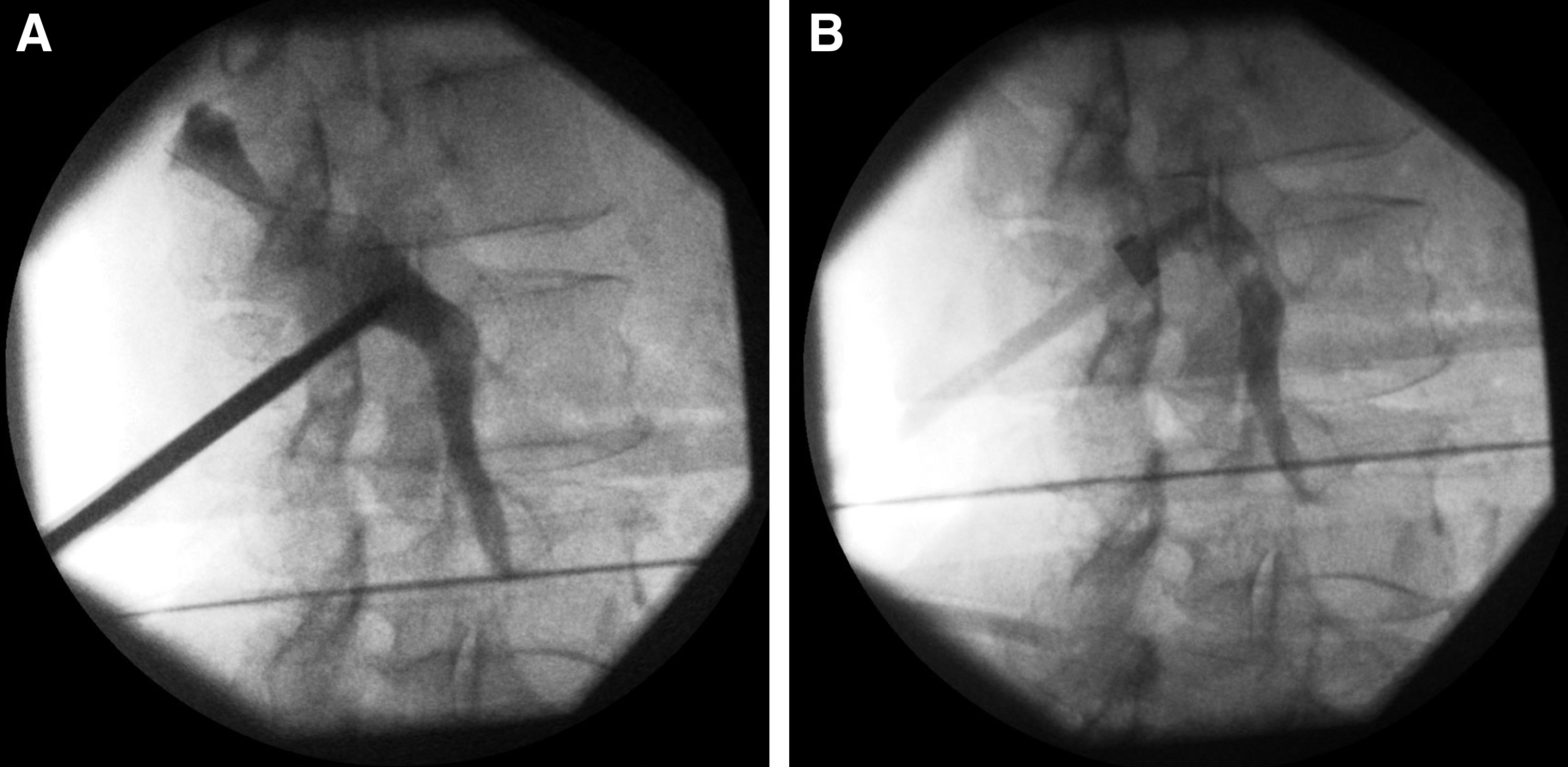
Detour EAS insertion and revisions have been performed by a single consultant with a specialist Endourology interest in a standard manner. The operation is performed under general anesthesia with the patient inclined in three-quarters dorsal decubitus, with prophylactic antibiotics given to local guidelines. The renal cavities are punctured under ultrasound guidance, with the tract dilated to 30F (Figs. 1 and 2A); all patients in our case series had existing nephrostomy tracts, which were used to access the renal cavity if deemed suitable. An Amplatz sheath is introduced under fluoroscopic guidance, and the Detour EAS is introduced through the sheath and positioned with the aid of a radio-opaque ring on the proximal end of the Detour EAS (Fig. 2B). Using a Seldinger technique, the Amplatz sheath is withdrawn, and the subcutaneous tunneling device is used to create a tract from the kidney to the suprapubic region (Fig. 3). The distal end of the Detour EAS is introduced into the tunneling device. The bladder is distended using a three-way catheter, to enable safe access to the bladder via a suprapubic Pfannenstiel incision. An open cystotomy is performed and the distal end of the Detour EAS (Fig. 4) is introduced into the bladder. The bladder is closed over the outer polytetrafluoroethylene (PTFE) tube with 3-0 Vicryl sutures (Fig. 5). A Foley catheter is removed after 1 week.

Dilatation of the percutaneous track with metal dilators.

Creation of a subcutaneous tunnel from the renal pelvis to the suprapubic region, with the distal end of the EAS passed through the tunneling device.

Urine drainage from the distal end of the Detour EAS.
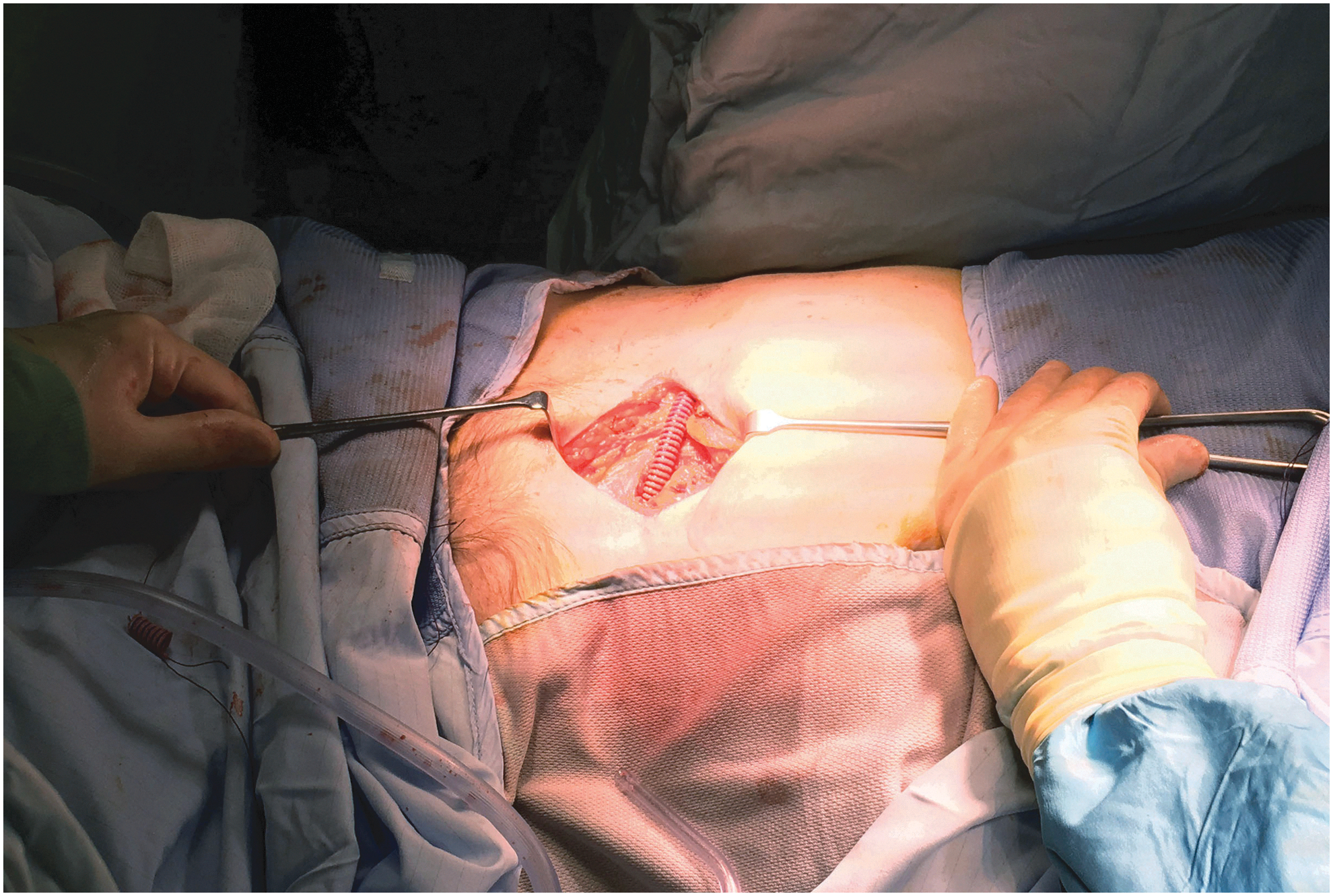
The distal end of the Detour EAS secured with 3-0 Vicryl in the bladder.
Patients
Between December 2001 and October 2017, 20 Detour EAS were implanted into 13 patients (6 male, 7 female) (Table 1). Five patients required bilateral EAS, and two patients had a contralateral EAS inserted after initial unilateral insertion, at 18.5 and 34.5 months, respectively. Demographics as well as intraoperative and postoperative complication data were collected retrospectively, and 30-day surgical complications were classified according to the Clavien–Dindo classification system. 10 The mean age at the time of implantation was 64 years (range: 50–83 years), and the median follow-up was 12 months (range: 1.5–42 months). The median follow-up for the cohort that died with the Detour EAS in situ was 7.8 months, and 26 months for the cohort alive at last follow-up. Before insertion, mean hemoglobin was 107 g/dL (range: 73–137 g/dL); mean creatinine 169 μmol/L (range: 99–358 μmol/L); and mean estimated glomerular filtration rate (eGFR) 39 mL/min (range: 11–63 mL/min). The primary cause for ureteric obstruction was metastatic malignancy, or ureteric injury from treatment for malignancy, where ureteric stenting has failed. All patients had existing nephrostomies in situ on the affected collecting systems. Eleven patients had EAS inserted into their bladder, and two diverted into a double-barreled stoma sited in the iliac fossa. Postoperatively, all patients were followed up in the outpatient clinic.
Summary of Patients and Outcomes
EAS = extra-anatomic stent.
Contralateral insertion after initial unilateral insertion.
Results
Perioperative complications
Grade I complications were recorded in 20%, grade II in 20%, grade IIIb in 20%, and grade IVa in 6.7% of cases (Table 2). Patients 3, 7, 10, and 13 developed fevers in the postoperative period, with three of them requiring intravenous antibiotics. Patients 3, 5, and 9 developed early urinary leaks, requiring stent revision, and patient 6 developed a urinary leak at 3 months requiring revision.
Postoperative Complications
Following insertion, the mean creatinine was 132 μmol/L (range: 77–215 μmol/L) and mean eGFR 48 mL/min (range: 20–66 mL/min); an improvement of 37 μmol/L and 9 mL/min, respectively.
Patient 12 had bilateral Detour EAS insertion for ureteric obstruction secondary to retroperitoneal fibrosis complicating cervical cancer radiotherapy, causing bilateral hydronephrosis. The patient had bilateral nephrostomies in situ before Detour EAS insertion. Postoperatively, the left EAS dislodged, and the subsequent laparotomy to replace the stent, although successful, was complicated by sigmoid bowel perforation. An end colostomy was fashioned following bowel perforation, which subsequently required resiting. The patient developed a pelvic abscess and intra-abdominal sepsis following laparotomy and died 6 weeks following the initial procedure. The right EAS remained patent and functioning at time of death.
Long-term complications
Infection
Patient 12 developed urinary tract infections 3 months after insertion, which were managed with oral antibiotics and did not require hospital admission. Patients 4 and 10 had recurrent infections in the EAS, requiring intravenous antibiotics.
Obstruction
Patient 4 developed obstruction in the EAS at 36 months, which was successfully recanalized with waterjet by interventional radiologists. No other episodes of obstruction have occurred in the case series.
Erosion
Patients 5, 9, and 11 developed erosion of the skin overlying the EAS. Patient 9 had a revision to due erosion bilaterally; erosion was otherwise managed conservatively.
In all these patients, the EAS continued to drain successfully following treatment or revision. Eight patients died during follow-up. Seven patients died due to complications from their progressive metastatic malignancy, and the Detour EAS was functioning in all seven at time of death. Five patients remain well with functioning Detour EAS in situ.
Discussion
Findings and complications from our case series of a procedure with niche indications are comparable to other similar centers. The majority of our patients had metastatic malignancy affecting the ureters, except two which had obstruction secondary to retroperitoneal fibrosis. Mortality is high and follow-up duration limited as these patients have multiple comorbidities with underlying poor prognosis and life expectancy.
Complete ureteric obstruction in malignancy is traditionally managed with percutaneous nephrostomy, leading to a reliance on collecting appliances and reduced quality of life. 7 The first successful EAS insertion was reported in the literature by Schulman et al. in 1976 11 ; however, it is only within the last 20 years that use of double pigtail EAS have been established reported practice. Due to its relatively infrequent use, it proves challenging to formally evaluate the success of extra-anatomic stenting methods. Clinical experience of using a double pigtail EAS was first reported by Ahmadzadeh in 1991, 12 then subsequently by Lingam and colleagues and Nakada and colleagues. 7,13 These were single lumen rigid stents between 7F and 11F in diameter, 50 to 70 cm in length. The small diameter predisposed to encrustation, 7,12 necessitating frequent changes. For this reason, Andonian and colleagues suggested a minimum diameter of 17F to reduce the risk of obstruction. 4
Desgrandchamps and colleagues reported the first use of the Detour EAS (Porges-Coloplast); a permanent large bore, dual lumen stent, composed of an 18F silicone inner lumen and a 28.5F to 29F, 70 cm expanded PTFE outer tube. 2 Their follow-up series in 2001 concluded that the Detour EAS was an efficient and minimally invasive method to bypass ureteric obstruction. 14 Several other small case series using the Detour EAS have been reported in the literature since the initial findings from Desgrandchamps and colleagues. In our series, only one EAS was complicated by obstruction, demonstrating the effectiveness of increasing lumen size to reduce the risk of obstruction. This occurred at 34 months after insertion and compares favorably with the results of Schmidbauer et al., who used two connected 12F stents (Rüsch, Germany) and reported obstruction in 5 of 28 patients (17.9%), at a mean of 10.2 months. 15 In their series, this required replacement of the bypass system; in our patient, the obstruction was successfully cleared using interventional radiology.
Other complications to consider include the risk of urinary tract infection, which are increased primarily due to the insertion of an artificial device, and immunocompromise from malignancy. The use of prophylactic antibiotics during the perioperative period can help to minimize this. The complications highlighted by Patient 12 indicate the high risk of the procedure and the importance of patient selection, particularly in the presence of previous radiotherapy and the likelihood of a “frozen pelvis,” and the need to be aware that the pelvic dissection and open suprapubic insertion can be technically challenging. However, in carefully selected patients, particularly those where malignant obstruction has proved resistant to complex reconstruction or repeat stenting, the opportunity to internalize nephrostomy drainage can significantly improve quality of life, even in the short term. Two patients with unilateral EAS proceeded to have bilateral EAS insertion. To date, this is one of the largest case series published in the United Kingdom.
Conclusions
Understandably, as the primary indication for the Detour EAS is for malignant ureteric obstruction, and hence palliation, longer term outcomes are challenging to measure. The Detour EAS system provides a suitable alternative option for urinary diversion, affording a good quality of life to patients with multiple comorbidities and progressive malignant disease. This must be balanced against the complexity and risk of complications of the insertion and requires careful patient selection.
Footnotes
Acknowledgment
We thank Mr. Ian Donaldson for the intraoperative photographs.
Author Disclosure Statement
No competing financial interests exist.