
Abstract
Objectives:
Ureteral stenting is a widely used method for noninvasive urinary drainage in ureteral obstruction. However, biofilm development due to transient bacteriuria can cause severe complications such as incrustation with subsequent obstruction as well as recurrent urinary tract infection. Apart from local ailment such as dysuria, this increases both stent replacement frequency and incidence of complications. In this work, we investigated in vitro the bacterial adhesion to a surface-attached and cross-linked poly(N,N-dimethylacrylamide) (PDMAA) hydrogel network, which is known for its nonfouling and protein-repellent characteristics.
Materials and Methods:
To mimic the conditions encountered in vivo, PDMAA-coated and uncoated cyclic olefin polymer (COP) slides as well as polyurethane (PU)-coated glass slides were incubated in sterile human urine for 48 hours. Colonization was then simulated by adding known uropathogens, cultivated from clinical urine samples (such as Escherichia coli). After further incubation for 24 and 48 hours, slides were washed, and the remaining adherent bacteria were solubilized by ultrasound. CFUs were counted after plating and incubation for 48 hours of the resulting solution.
Results:
PDMAA reduced adherent E. coli about fivefold on coated PU glass slides as well as in PDMAA-coated COP slides. With adherent Enterococcus faecalis and Klebsiella pneumoniae there was a tendency to decreased biofilm formation, but the difference was not statistically significant.
Conclusions:
PDMAA reduces surface adherence of the most common uropathogen significantly. Assessment of clinical relevance and of the effect on further uropathogens needs further experimental and clinical evaluations. German Clinical Trial Register ID: DRKS00013264 (approved WHO primary register).
Introduction
U
Materials and Methods
Preparation of coated slides
PU-coated glass slides and cyclic olefin polymer (COP; type ZEONOR 1420R) slides were provided by the Laboratory for Chemistry and Physics (IMTEK). PU-coated microscope glass slides were prepared by dip coating at 200 mm/min (Zwick BZ2.5/TN1S; Zwick GmbH & Co. KG, Germany) into a tetrahydrofuran (THF) solution containing 10 mg/mL of dissolved commercially available ureter stents (HYDROPUR®; UROMED Kurt Drews KG, Germany). For the hydrogel coatings, PU-coated glass slides and clean COP slides were dip coated into an ethanol polymer solution of 10 mg/mL polydimethylacrylamide with 5 mol% ( = relative amount of the monomer in reference to the Avogadro number) 4-methacryloyloxobenzophenone (PDMAA-5%BP) for cross-linking. The PDMAA copolymer was synthesized as published 20,21 with the exception that the benzophenone content was set to 5 mol%. Air-dried coatings were immediately cross-linked and surface attached by UV irradiation with 1 J/cm2 at 254 nm in a UV-Stratalinker (Stratagene, CA), which induces C,H-insertion reactions of the benzophenone moieties. The thickness of the hydrogel coatings was varied by dip coating velocities (faster withdrawal speeds result in thicker layer depositions). Withdrawal velocities of 30, 100, and 200 mm/s resulted in approximated dry hydrogel coatings with thin layers (<50 nm), medium layers (50–100 nm), and thick layers (>100 nm). The swelling factor of such surface-attached and cross-linked PDMAA-5%BP layers is in the range of 2–4. 22,23
All slides were autoclaved for 1 hour at 121°C with a Systec DE-45 (Systec GmbH, Germany) before experimentation.
Experimental setting and test protocol
Human urine was collected under aseptic condition from one of the authors (T.S.). Standard urine culture and antimicrobial activity examination (Mueller–Hinton agar plate with Bacillus subtilis) was performed from each collected urine sample to ensure sterility and to exclude the presence of antimicrobial substances. All experiments were performed under aseptic conditions (laminar airflow cabinet; sterile instruments). Slides were incubated in sterile urine at 37°C for 48 hours, while they were shaken continuously to allow adherence of inorganic components to the slide. An overnight preculture was grown on Columbia blood agar (37°C, 5% CO2). Ten microliters of LB broth was inoculated with a single colony and grown to an OD600 of 0.6–0.7 (log-phase). Fluid culture was added to the urine samples with the slides for a final bacterial load of 1 × 105/mL. In our study, uropathogenic strains from Escherichia coli, Enterococcus Faecalis, and Klebsiella pneumoniae were used, originating from anonymized patient samples of the Institute for Microbiology and Hygiene, representing the three most frequently isolated urinary pathogens (from 2014 to 2016) at the Medical Center of the University of Freiburg in a concentration of at least 10 5 CFU/mL. Identification of bacterial strains was performed using matrix-assisted laser desorption/ionization time of flight mass spectrometry (MALDI-TOF). Clinical data on the frequency of stent-related cultures were not available. Slides with the inoculated urine were cultivated under aerobic conditions (at 37°C) for 24 and 48 hours and shaken continuously. After incubation, slides were taken out of the urine and washed in 1% phosphate-buffered saline (PBS) three times to differentiate and remove the nonadherent (planktonic/free-floating bacteria). Ringer solution (50 mL) was pipetted to the washed slides until complete coverage was achieved. Covered slides were then vortexed for 30 seconds and sonicated (frequency, 40 ± 2 kHz and power density, 0.22 ± 0.04 W/cm2, for 1 minute, Bactosonic, Bandelin), followed by additional vortexing for 30 seconds. After this step, 10 and 100 μL of the resulting ringer solution was pipetted onto three agar plates (Columbia blood agar) and incubated for 48 hours (at 37°C, 5% CO2), and the remaining solute was discarded. Afterward colony forming units (CFUs) were counted and are reported in CFU/mL, depicting the bacterial concentration in the solute All experiments were repeated three times. The test protocol is illustrated in Figure 1.

Schematic depiction of test protocol for evaluation of biofilm formation in this study.
Statistical evaluation
CFU counts were evaluated using the Wilcoxon rank-sum test. All statistical computations were performed using Python 2.7 (Enthought, Austin, Canopy distribution 1.1.0.1371; scipy statistical package). The test used in each case is indicated by superscript letters. P-values <0.05 were considered to be significant.
Results
PU-coated glass slides (PU) vs PDMAA-coated PU glass slides (PU-PDMAA)
To investigate the influence of PDMAA coating on bacterial colonialization in vitro, we compared glass slides only coated with PU with glass slides coated with PU and an additional coating of PDMAA. Experiments were performed for uropathogenic strains of E. coli, K. pneumoniae, and E. faecalis, as described above. For every parameter (24 and 48 hours of incubation as well as 10 and 100 μL of pipetted solution after sonication) the experiment was repeated three times (Supplementary Table S1; Supplementary Data are available online at
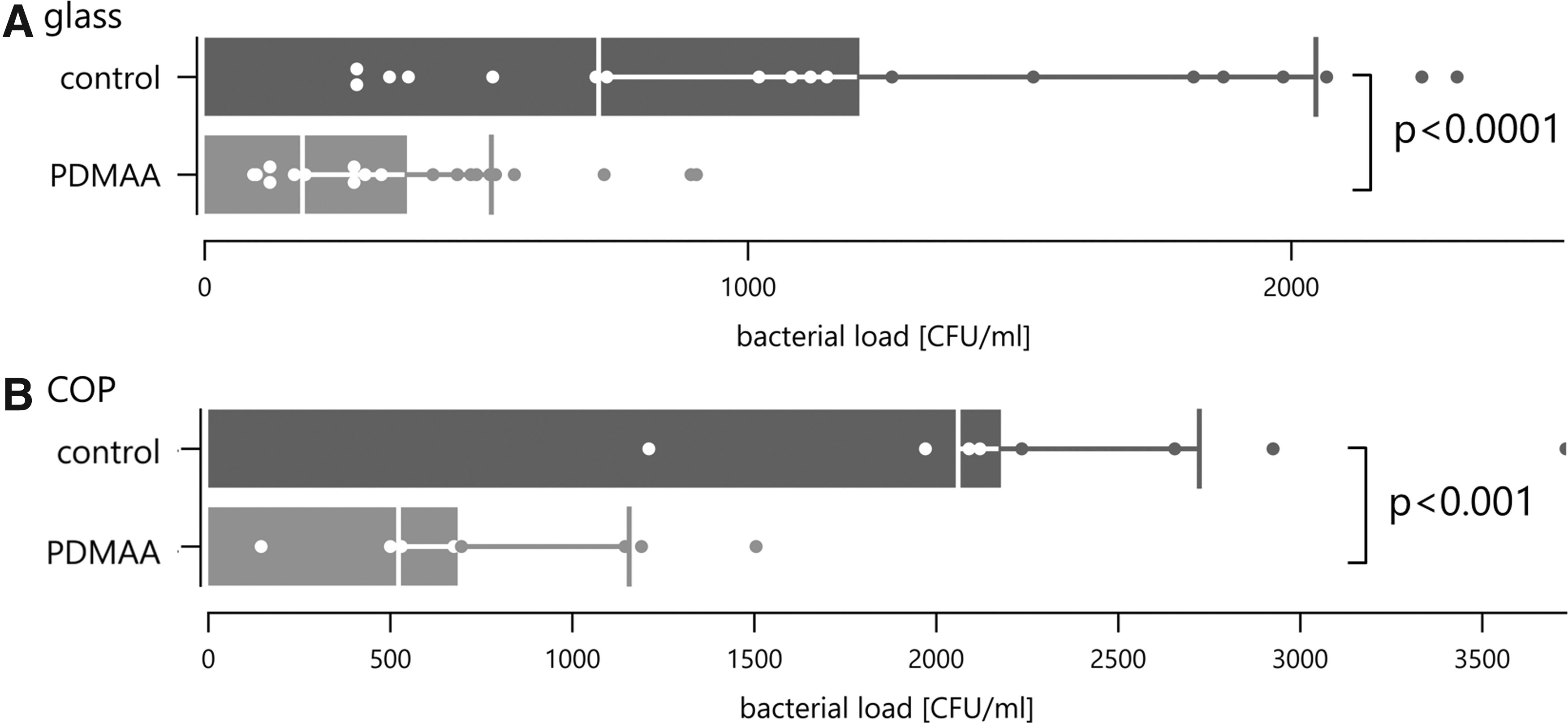
Cumulative bacterial load of PDMAA-coated glass slides

Cumulative bacterial load of PDMAA-coated glass slides in comparison with a control group (PU slides) for all examined bacterial species. All performed experiments have been combined into one data point (incubation over 24 and 48 hours; 10 and 100 μL pipetted solute).
COP slides (COP) vs PDMAA-coated COP slides (COP-PDMAA)
To exclude coating defects of PDMAA coatings due to incompatibilities of noncovalently attached PU coatings on glass slide surfaces, COP slides were used. Compatibility of COP and PDMAA was confirmed previous to our study. Experiments were performed for uropathogenic strains of E. coli, K. pneumoniae, and E. faecalis, as described above (Supplementary Table S1). For E. coli the average number of CFUs was 22,600 ± 1018/mL (10 μL) and 29,800 ± 3652/mL (100 μL) in the control group, and 800 ± 525/mL (10 μL) and 788 ± 4472/mL (100 μL) for the PDMAA-coated COP slides after 24 hours of incubation. After 48 hours of incubation, a similar picture was observed, with 1630 ± 573/mL (10 μL) and 22,560 ± 6084/mL (100 μL) CFUs in the control group and 830 ± 262/mL (10 μL) and 7760 ± 3349/mL (100 μL) for the COP-PDMAA group. Overall, a significantly reduced bacterial load was detected in the COP-PDMAA group after 24 hours (P < 0.001) as well as 48 hours (P = 0.010). No significant difference was seen for bacterial colonialization with E. faecalis and K. pneumoniae; however with an overall average of 70,400 CFU/mL (control group) vs 61,900 (COP-PDMAA) CFU/mL for K. pneumoniae and 42,900 (control) vs 36,000 (COP-PDMAA) CFU/mL for E. faecalis a tendency for a lower bacterial load in the COP-PDMAA group was observed as well (Fig. 2).
Influence of PDMAA copolymer thickness on bacterial colonization
In a third experiment, the influence of the thickness of PDMAA coating on the bacterial load was investigated (Supplementary Table S1). Experiments were performed in the same manner as described above. For E. coli, the overall average values of CFUs were 123,300/mL (control group), 9800/mL (thin layer), 6000/mL (medium layer), and 46,300/mL (thick layer), depicting a significantly reduced bacterial load for the medium layer (P = 0.003) and the thick layer (P = 0.001) of PDMAA coating. In addition, the thick layer of PDMAA coating showed a significantly reduced CFU count compared with the thin coating (P = 0.0079). As in the previous experiments, no type of PDMAA coating caused a significant change in bacterial colonialization of E. faecalis or K. pneumoniae, but again a tendency toward a decreased colonialization was noticed (Fig. 4).
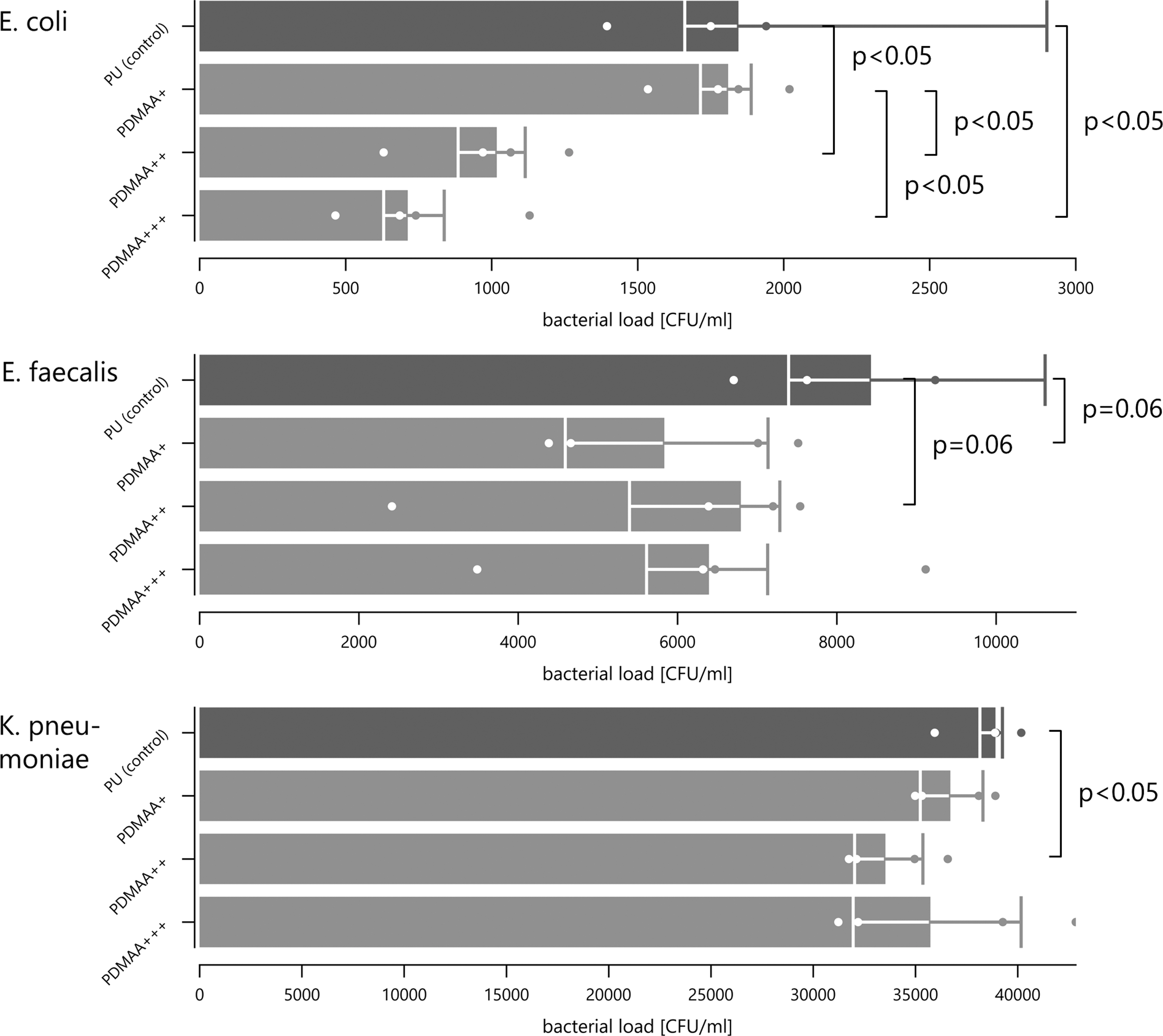
Cumulative bacterial load of PDMAA-coated glass slides compared with a control group (PU slides) for thin layers (PDMAA+; <50 nm), medium layers (PDMAA++; 50–100 nm), and thick layers (PDMAA++; >100 nm) of PDMAA. Results are depicted for all examined bacteria. All performed experiments have been combined into one data point (incubation over 24 and 48 hours; 10 and 100 μL pipetted solute).
Discussion
Biofilm formation on artificial surfaces is a clinical problem in all fields that use medical implants, and extensive research has been dedicated to this issue. However, stent infection remains the major cause for ureteral stent failure, 12 and although most complications occur in chronically stented patients, even patients with short-term stenting are at risk. 24 In this study, we investigate the coating agent PDMAA as a means to reduce microbial colonialization in an in vitro setting. Since the adsorption of cytokeratin plays an important role in the multistep process 25 of bacterial adherence, PDMAA is thought to be able to disrupt this process. It is presumed that after the conditioning film proteins have attached to the implant surface, the attachment of other molecules, such as collagen, fibrinogen, and albumin, 26 is facilitated, and subsequently microorganism can attach more easily to the surface. By preventing the adsorption of these initial conditioning film proteins through “entropic shielding” the PDMAA coating is supposed to prevent the first step of biofilm formation, and therefore inhibit the bacterial colonialization of the coated implant. However, other studies have suggested that biofilm formation only plays a minor role in the colonialization of ureteral stents and the mechanism that allows bacteria to attach to the implant is still not fully understood. 27 In this study, we were able to demonstrate an in vitro beneficial effect of a PDMAA coating on the colonialization with E. coli, reducing the bacterial load significantly. E. coli is the most common uropathogen responsible for ∼80% of all UTIs 28 and the most dominant colonizer of ureteral stents. 29 On the contrary, while a tendency for a decrease in bacterial colonization was observed, the PDMAA coating did not significantly reduce the attachment of other important uropathogens (K. pneumoniae, E. faecalis), suggesting that no protective effect against these pathogens can be generated by covering ureteral stents with PDMAA. We speculate that these pathogens are not fully dependent on protein adsorption, but adherence to the implant surface is achieved by other mechanisms. In addition, since only specific strains and the urine of one test subject were used, a smaller effect of PDMAA might only become statistically apparent in a larger sample size. Further studies are necessary to investigate this issue. Our study has some limitations. First, we performed an exclusive in vitro study. Biofilm-associated infections and bacterial colonialization not only depend on bacterial biological behavior but also on the host environment, and therefore our results cannot be applied directly to an in vivo setting. Furthermore, we examined only the most common uropathogens found in urine cultures at our medical center without a correlation to the frequency of stent-related infection, balancing known biofilm formers (such as E. faecalis 30 ) against clinically important bacteria (such as E. coli and K. pneumoniae) with our chosen bacteria. Since it was demonstrated previously that uropathogens isolated from urine cultures often differ from stent cultures 31 and no regional data on the most common bacteria in stent-related infection are available, this is a potential limitation to our study. However, our intention was to investigate the effect of PDMMA coating on bacterial colonialization and biofilm formation in general, and we were able to demonstrate a potential benefit of our coating. To fully evaluate our approach, other uropathogenic bacteria need to be tested, and the effect was evaluated over a longer period of time. Further studies also have to determine the feasibility of PDMAA as a material for stent coating regarding technical implementation and biocompatibility. Ultimately, clinical studies in humans will be necessary to determine if the reduction in bacterial load by PDMAA results in a clinical benefit. Despite the limitations of our study and the missing effect on non E. coli uropathogens we believe that further development of PDMAA as a coating material for ureteral stents is a promising way to reduce complications of indwelling ureteral stents. As suggested in previous studies on prevention and eradication of biofilm on urological devices, 24 the development of a biofilm-resistant stent will most likely need to entail a combination of different strategies to target all different ways of bacterial adsorption and proliferation. PDMAA should be considered as one building block in the development of this combination.
Conclusions
Protein-repellent PDMAA coatings reduce surface adherence of uropathogenic E. coli significantly. Although a significant effect on K. pneumoniae and E. faecalis was not detected, suggesting a variable relevance for protein adsorption in bacterial colonization of urological implants, PDMAA showed a tendency to decrease biofilm formation also for these uropathogens. Identification of the underlying mechanisms and assessment of clinical relevance need further evaluation.
Footnotes
Disclaimer
The work has not already been published and has not been submitted simultaneously to any other journal.
Authors' Contribution
Tamas Szell, MD, Protocol/project development, conduction of experiments, data collection and management, data analysis,
Franz Friedrich Dressler, MD, Data analysis, manuscript and figure writing/editing
Hanna Goelz, MD, Supervision and conduction of experiments
Benjamin Bluemel, MD, Supervision and conduction of experiments
Arkadiusz Miernik, MD, PhD, Protocol/project development, manuscript and figure writing/editing, supervision
Thomas Brandstetter, PhD, Protocol/project development, developed coating agent
Frank Scherag, PhD, Protocol/project development, developed coating agent
Dominik Stefan Schoeb, MD, Protocol/project development, data collection and management, data analysis, manuscript and figure writing/editing, supervision.
All authors have made a significant contribution to the findings and methods in this paper. All authors have read and approved the final draft.
Ethical Approval
The study was approved by our local ethics committee and was therefore performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All participants gave their informed consent to provide stone material prior to their inclusion in the study. Number 221/17, Ethics Committee of the University Medical Center Freiburg.
Author Disclosure Statement
None of the authors have any conflict of interest or financial ties to disclose.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.