
Abstract
Background:
Percutaneous nephrolithotomy (PCNL) requires the urologist to have detailed knowledge of the stone and its relationship with the renal anatomy. Immersive virtual reality (iVR) provides patient-specific three-dimensional models that might be beneficial in this regard. Our objective is to present the initial experience with iVR in surgeon planning and patient preoperative education for PCNL.
Materials and Methods:
From 2017 to 2018 four surgeons, each of whom had varying expertise in PCNL, used iVR models to acquaint themselves with the renal anatomy before PCNL among 25 patients. iVR renderings were also viewed by patients using the same head-mounted Oculus rift display. Surgeons rated their understanding of the anatomy with CT alone and then after CT+iVR; patients also recorded their experience with iVR. To assess the impact on outcomes, the 25 iVR study patients were compared with 25 retrospective matched-paired non-iVR patients. Student's t-test was used to analyze collected data.
Results:
iVR improved surgeons' understanding of the optimal calix of entry and the stone's location, size, and orientation (p < 0.01). iVR altered the surgical approach in 10 (40%) cases. Patients strongly agreed that iVR improved their understanding of their stone disease and reduced their preoperative anxiety. In the retrospective matched-paired analysis, the iVR group had a statistically significant decrease in fluoroscopy time and blood loss as well as a trend toward fewer nephrostomy tracts and a higher stone-free rate.
Conclusions:
iVR improved urologists' understanding of the renal anatomy and altered the operative approach in 40% of cases. In addition, iVR improved patient comprehension of their surgery. Clinically, iVR had benefits with regard to decreased fluoroscopy time and less blood loss along with a trend toward fewer access tracts and higher stone-free rates.
Introduction and Objectives
N
CT provides detailed 2D visual information of the renal anatomy. Recently, Brehmer and colleagues demonstrated that utilizing a three-dimensional (3D) rendering of the CT scans, although on a typical 2D screen display, improved operative outcomes and reduced the number of punctures needed. 7 Similarly, incorporation of 3D CT reconstructions into a tablet-based augmented reality system reduced puncturing time for trainees and fluoroscopy time for trainees and experts alike. 8,9
In a similar attempt to improve surgeons' understanding of renal anatomy, Radecka et al. used CT-based 3D printing to recreate patients' anatomy, and found it to be helpful for preoperative planning. 10 However, there are several limitations to current 3D printing modalities. The technology is time consuming, expensive, and not universally available. In addition, the static nature of the 3D-printed models only provides a surface representation of structures.
To overcome these shortcomings and further advance surgeon and patient preoperative understanding, we created patient-specific, CT-based immersive virtual reality (iVR) models that immerse the observer in an interactive 3D simulation of the patient's renal anatomy in relation to the intrarenal calculus. Using iVR, surgeons manipulate, segregate, and visualize all relevant anatomic components including the boney structures, the vascular anatomy, the renal parenchyma, the collecting system, the stone(s), and the surrounding organs (i.e., spleen or liver). The surgeon could also have the patients view the iVR demonstration to aid their understanding of the planned PCNL. Our pilot study is the first description of iVR for PCNL. Our primary objective was to evaluate the efficacy of iVR technology for preoperative planning. Second, we sought to determine whether the iVR models could enhance patient understanding and comfort with PCNL. Lastly, we sought to assess the impact of iVR on surgical outcomes.
Materials and Methods
Subject recruitment
An observational prospective study design was used to recruit patients with large renal calculi scheduled for PCNL at UC Irvine. Using our PCNL database, we retrospectively matched each patient with a similar patient who had not undergone iVR planning. Matching was based on six parameters: stone burden, American Society of Anesthesiologists (ASA), age, body mass index (BMI), gender, and nephrostomy tract placement (upper/lower pole posterior calix). PCNL cases in the iVR group occurred between 2017 and 2018. Retrospectively matched cases occurred between 2015 and 2016. All cases were performed using the endoscope-guided access technique by endourologists with varying experience. 11
Preoperative evaluation
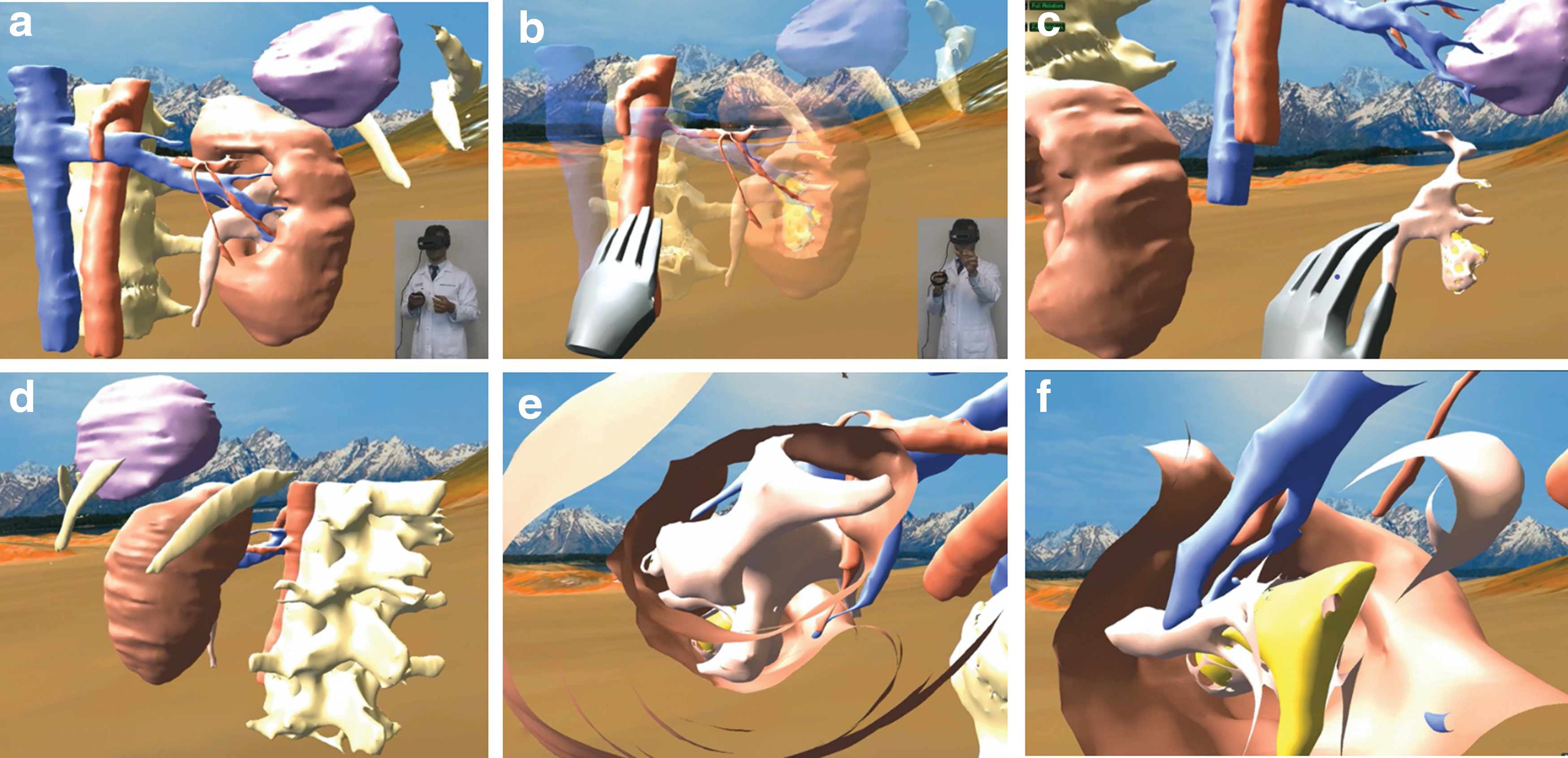
Surgeons were asked to first review a patient's CT images and complete an assessment questionnaire (0 = poor to 10 = excellent) to evaluate their understanding of the patient's anatomy and stone location/burden; then surgeons examined their patient's iVR model (Fig. 1) and again completed the assessment questionnaire (Supplementary Data). Surgeons spent a similar amount of time reviewing each imaging modality. CT images, iVR models, and assessment questionnaires were completed on the day of surgery and were validated by our principle investigators. Surgeons completed a preoperative Likert-style questionnaire (1 = strongly disagree to 5 = strongly agree) to record their experience with the iVR model vs CT alone.
Virtual reality model.
Postoperative evaluation
After PCNL, surgeons completed a postoperative assessment (1 = strongly disagree to 5 = strongly agree) to determine whether the iVR model affected their operative approach, and how accurately the iVR model reflected the patient's encountered anatomy (Supplementary Data). The operative time, blood loss, fluoroscopy time, and number of renal punctures were also recorded. Postoperative assessment scores were designed to reveal whether the iVR was additive to the CT scan when forming a preoperative plan.
Patient evaluation
Patients completed a preoperative questionnaire (1 = strongly disagree to 5 = strongly agree) to assess their understanding of their renal anatomy, the planned PCNL, and their comfort with the planned surgery (Supplementary Data). This was administered initially after viewing their CT scan with coronal, sagittal, and axial views, and then a second time after viewing their iVR model. Viewing of the CT scan and the iVR was facilitated by a physician or research fellow.
iVR model creation
3D Slicer (National Institute of Health, Bethesda, MA) was used to create 3D models using 2 to 3 mm thick noncontrast CT images in Digital Imaging and Communications in Medicine (DICOM) format. Synthesized 3D models were subsequently uploaded to Bosc, an iVR software (Pyrus Medical, Seattle, WA), to make the images viewable with a head-mounted display. No repeat CT scans were performed to create iVR models. Slice by slice, segmentation of the anatomy was performed manually by either a physician or research fellow. Anatomical structures were delineated on the CT image through the 3D Slicer. The complete vascular anatomy was depicted in all 25 iVR model cases.
The Oculus Rift and Touch controllers (Facebook, Inc., Menlo Park, CA) paired with Leap Motion (Leap Motion, Inc., San Francisco, CA) were utilized as the head-mounted display for iVR model observation/manipulation. Initially, it took 6 to 9 hours to prepare the iVR model; however, after making three to four iVR models, the time stabilized at 1 to 2 hours.
Microsoft Excel 2016 was used for statistical analysis using two-tailed t-tests and chi-squared analysis. The normality of the data was evaluated through MySTAT, a statistical program. The mean and standard deviation were reported for all normally distributed data. p-Values were calculated using a standard, two-tailed t-test. For non-normally distributed data, the median and interquartile range were reported, and the p-value was calculated using a Kruskal–Wallis nonparametric test. Significance was defined as p < 0.05.
Results
Twenty-five PCNL procedures were performed between 2017 and 2018. All data were normally distributed except for fluoroscopy time, preoperative stone diameter, operative time, and blood loss. The mean age of the 25 iVR participants was 55.9 years (SD = 15.5), ASA score was 2.5 (SD = 0.71), and BMI was 29.5 kg/m2 (SD = 5.94) (Table 2). The median preoperative cumulative stone diameter was 35 mm (interquartile range [IQR] = 28.5) and the mean stone density was 1072 HU (SD = 338). The median operative time was 155 minutes (IQR = 63.5)with a median estimated blood loss of 50 mL (IQR = 75); mean number of needle punctures was 1.13 (SD = 0.46) and median fluoroscopy time was 180 seconds (IQR = 122). Upper pole access was established in 21/25 (84%) of cases and lower pole access was established in 4/25 (16%) of cases. Based on postoperative CT scans (n = 23), the complete stone-free rate was 39% (n = 9/23) and <4 mm stone remnant rate was 48% (n = 11/23). A single intraoperative complication occurred in a patient with increasing peak airway pressure requiring early termination of the procedure. There were four postoperative complications in the iVR group (three Clavien grade I and one Clavien grade IIIa) (Table 2).
Preoperative surgeon evaluation
The surgeon preoperative assessment showed surgeons felt capable of formulating a surgical plan and felt confident going into surgery after reviewing CT imaging alone (4.00/5 and 4.08/5, respectively) (Table 1). After iVR model review, surgeons strongly agreed that their overall understanding and confidence of performing the operation improved (4.76/5). Surgeons strongly agreed that the iVR model is a valuable surgical planning tool (4.72/5), that they would use iVR technology in future cases (4.88/5), they would recommend iVR technology to their colleagues (4.84/5), and that they would use iVR as an educational tool for residents (4.92/5).
Virtual Reality Model Questionnaires
Bold type indicates statistically significant p values.
iVR = immersive virtual reality.
On the surgeon imaging assessment, the iVR model provided a significantly greater understanding of stone location (9.60 vs 8.08, p < 0.01), stone size (9.24 vs 8.63, p < 0.01), shape and orientation of the stone (9.68 vs 6.84, p < 0.01), and optimal calix of entry (9.52 vs 7.56, p < 0.01) than CT imaging alone. The iVR model and CT imaging alone measured similarly in understanding the ease of navigation with a rigid nephroscope (7.72 vs 6.88, p = 0.129).
Preoperative patient evaluation
Of the 25 patients recruited for our iVR study, 20 completed a patient assessment. Patients strongly agreed that the iVR model enhanced their understanding of the location and the size/shape of their stone (4.95/5, 4.95/5, respectively) (Table 1). Patients agreed that the iVR model made them less anxious about PCNL (4.00/5) and improved their understanding as to why the PCNL procedure was indicated (5/5). Neither patients nor surgeons experienced motion sickness while using iVR. Of note, no sound accompanied our virtual reality models.
Postoperative surgeon evaluation
Postoperatively, surgeons agreed that the iVR model assisted in navigating the intrarenal anatomy (4.12/5) (Table 1). Surgeons also indicated that iVR models were accurate with regard to the chosen calix of entry (4.44/5), and offered an improved understanding of the patient's collecting system and its relationship with the stone compared with CT alone (4.40/5). Surgeons strongly agreed that the iVR model demonstrated an accurate location, size of the stone, and degree of hydronephrosis (4.64/5, 4.68/5, 4.68/5, respectively). The iVR technology altered the operative approach in 40% of the cases (10/25).
Retrospective matched outcomes analysis
The iVR group was compared with patients in our PCNL data base from 2015 to 2016. Twelve iVR patients matched with non-iVR patients on at least five of the aforementioned six criteria, and the remaining 13 patients matched on at least four criteria. Fourteen patients could be retrospectively matched for both stone burden and nephrostomy tract location (Table 2). The median estimated blood loss was 50% less in the iVR vs the retrospective group (50 vs 100 mL, p < 0.01). Moreover, the median fluoroscopy time was significantly reduced in the iVR group (180 vs 226 seconds, p < 0.01). There was a trend for fewer punctures in the iVR vs the non-iVR group (1.13 vs 1.46, p = 0.09), and the complete and <4 mm stone-free rates were higher in the iVR vs the non-iVR group (39% vs 20%, p = 0.15 and 48% vs 28%, p = 0.16).
Patient Demographics and Intraoperative Data for Virtual Reality and Retrospective Groups
Bold type indicates statistically significant p values.
p-Values calculated with the nonparametric Kruskal–Wallis test as associated data are not normally distributed.
ASA = american society of anesthesiologists score; BMI = body mass index; IQR = interquartile range.
Discussion
Current imaging software is capable of creating volume-rendered 3D images of the CT scans; however, these images currently can only be displayed on a 2D screen and are largely not interactive beyond rotating the anatomy vertically/horizontally. 12 –14 Recent advances in technology have allowed 3D printing to create physical models of the renal collecting system and stones. 15 –17 However, this technology has several limitations as it is time consuming, expensive, and not universally available. In addition, the 3D-printed models only provide an isolated surface-level representation of the kidney and, if made with a clear resin, the underlying stone.
In contrast to these renderings/models, iVR technology allows the observer to view and manipulate the model of the kidney and the intrarenal anatomy; indeed, the surgeon can actually peer along the planned nephrostomy tract to virtually travel along it into the planned calix of entry. 17 This interaction is both visual and tactile as the operator's virtual hand manipulates the anatomy and the stone. Indeed, in this study, each anatomical component could be separated to help clarify the anatomy, and individual components could be “ghosted” to allow the surgeon and the patient to optimally understand the anatomic relationship of the stone and its relationship with the collecting system (Fig. 1) (Supplementary Video S1).
With our iVR system, surgeons had a significantly improved preoperative understanding of the stone location, size, shape, and orientation using iVR models compared with CT alone. More importantly, the surgeons noted that after viewing the anatomy in iVR, they had a significantly improved preoperative understanding of the optimal calix of entry. In fact, the surgeons initially agreed they were uniformly confident in formulating a surgical plan using the CT scan alone. However, after these same surgeons viewed the iVR model of their patients, they altered their plan of approach in 40% of cases. Among these, alterations were changing from an initial upper pole access to a lower pole access, identifying a more optimal upper pole calix, and the identification of both an unsuspected duplicate system and a bifid system. Not surprisingly, these surgeons strongly agreed to use iVR technology for future surgery and for resident teaching.
Although 3D technology has been effectively used in other surgical specialties, and a few studies have similarly identified its beneficial role in urology for PCNL and partial nephrectomy, this is the first report of iVR for preoperative surgical planning and patient education. 10,15,16,18 –24 Of note, unlike the intraoperative system developed by Rassweiler and associates, our iVR system is a preoperative system specifically designed for preoperative PCNL planning. 8,9
The educational aspect of the iVR technology in our study was helpful in allaying patient anxiety—allowing patients to view their iVR model improved their understanding of the location, size, and shape of the stone. They were better able to comprehend why they were undergoing PCNL, and felt less concerned about their pending surgery.
In addition, the surgeon's postoperative assessment highlighted the accuracy of the iVR models as they agreed that it correlated with the patient-specific collecting system, location and size of the stone, and the chosen calix of entry (Table 1).
To our knowledge, this is the first study using a retrospectively matched PCNL comparison to evaluate the potential benefits of iVR technology in performing PCNL. There was a statistically significant drop in both blood loss and fluoroscopy time; furthermore, there was a trend (p < 0.10) toward fewer nephrostomy tracts and an improved stone-free rate in the iVR group. We believe that there might be similar benefits of iVR reconstruction in other aspects of renal surgery such as partial or donor nephrectomy.
iVR also benefits from the fact that models can be constructed from either noncontrast or contrast CT scans, and the software is such that the iVR model can be constructed without having to hire a software engineer. Finally, the 3D Slicer software is open source and free. The iVR hardware (i.e., Oculus Rift, touch controllers, Leap Motion, and iVR capable laptop) is off the shelf and commercially available; the total equipment cost is around $1700. There was no additional cost for personnel required to run the iVR software.
There are limitations to our study. The iVR models are dependent upon the quality of the CT scans. If the CT scan is of poor quality or the stone has shifted in the interim, iVR will be of a poorer quality or inaccurate, respectively. Furthermore, the 3D Slicer software requires additional training (see Materials and Methods: iVR Model Creation section) and there is a learning curve associated with creation of the 3D iVR models. Also, the iVR model creation process is currently dependent upon the user's experience in reading CT scans, and his/her ability to accurately label/color anatomical structures of interest.
Conclusions
Patient-specific iVR models accurately depicted surgical anatomy and improved surgeons' understanding of the individual patient's renal anatomy and the optimal location for PCNL access. Preoperative use of iVR models modified the surgical approach in 40% of patients. Furthermore, the iVR experience improved patient comprehension of the PCNL procedure and decreased their preoperative anxiety. Finally, the iVR patient group had a statistically significant decrease in both blood loss and fluoroscopy time, along with a trend toward fewer nephrostomy tracts and better stone clearance rates when retrospectively matched with similar patients in our PCNL data base.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.