
Abstract
Objective:
The aim of the study was to evaluate the predictive value of preoperative high-sensitive C-reactive protein/albumin (hs-CRP/Alb) ratio in systemic inflammatory response syndrome (SIRS) after percutaneous nephrolithotomy (PCNL).
Materials and Methods:
We retrospectively reviewed 556 patients who underwent PCNL at our institution between August 2015 and February 2018. The primary endpoint for the study was the development of SIRS after operation. A univariate and multivariate logistic regression analysis was used to identify the independent factors associated with the post-PCNL SIRS. Receiver operating characteristic (ROC) curves were constructed and the areas under the curve (AUC) were calculated to compare the discriminatory ability of systemic inflammation biomarkers.
Results:
Among the 556 patients who underwent PCNL, 123 patients (22.1%) developed SIRS. Multivariate analysis revealed that female gender (OR 1.691; 95% CI 1.045–2.735; p = 0.032), positive urine culture (OR 1.972; 95% CI 1.204–3.231; p < 0.01), hs-CRP/Alb ratio (OR 6.925; 95% CI 4.244–11.300; p < 0.01), neutrophil to lymphocyte ratio (NLR) (OR 2.476; 95% CI 1.471–4.167; p < 0.01), and prognostic nutritional index (PNI) (OR 0.559; 95% CI 0.338–0.924; p = 0.023) were independent predictors of post-PCNL SIRS. The optimal cutoff value of the hs-CRP/Alb ratio was 0.06 from the ROC analysis. The elevated hs-CRP/Alb ratio was significantly associated with female gender, positive urine culture, hs-CRP, albumin, leukocyte, neutrophil, monocyte, platelet, hemoglobin, creatinine, NLR, lymphocyte to monocyte ratio (LMR), platelet to lymphocyte ratio (PLR), PNI, high-sensitive modified Glasgow prognostic score (hs-mGPS), development of sepsis, ICU admission, and length of stay (all p < 0.05). In addition, the hs-CRP/Alb ratio had a higher AUC (0.791) with a sensitivity of 76.4% and a specificity of 73.2% than NLR (0.669), LMR (0.633), PLR (0.594), PNI (0.629), and hs-mGPS (0.739).
Conclusions:
The preoperative hs-CRP/Alb ratio is independently predictive for the development of SIRS after PCNL. Moreover, compared with other systemic inflammation biomarkers, the preoperative hs-CRP/Alb ratio shows a better predictive value.
Introduction
P
Systemic inflammatory response syndrome (SIRS), characterized by fever or hypothermia, hyperleukocytosis or leukopenia, tachycardia and tachypnea, is associated with the development of sepsis and recognized as the first step of the septic cascade. 4,5 Previous studies have reported that female gender, composition of stone, preoperative positive urine culture, operative time, residual stones, and access numbers are associated with post-PCNL SIRS. 6,7 However, most of these risk factors cannot be obtained before operation. In addition, it has been reported that positive preoperative urine culture was only shown to have a 15% positive predictive value for SIRS. 8
There is increasing evidence that systemic inflammation is involved in various pathologic conditions. Systemic inflammation biomarkers such as neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), and lymphocyte to monocyte ratio (LMR) have been reported to be effective predictors of post-PCNL SIRS. 9 The modified Glasgow prognostic score (mGPS) is calculated based on the serum concentrations of C-reactive protein (CRP; cutoff value: 10 mg/L) and albumin (Alb; cutoff value: 35 g/L) levels. With a lower threshold for CRP (cutoff value: 3 mg/L), the high-sensitive modified Glasgow prognostic score (hs-mGPS) has been demonstrated to be a superior prognostic predictor than mGPS in patients with esophageal cancer, 10 gastric cancer, 11 and soft tissue sarcoma. 12 Derived from the same variables, the high-sensitive C-reactive protein/albumin (hs-CRP/Alb) ratio, a novel systemic inflammation biomarker, has been shown to be a significant prognostic factor in several types of cancer. 13 –15 However, up to now, the association between the preoperative hs-CRP/Alb ratio and the post-PCNL SIRS has not been clarified.
In this study, we retrospectively investigated whether the preoperative hs-CRP/Alb ratio was independently associated with the development of SIRS after PCNL. In addition, we further evaluated the predictive value of hs-CRP/Alb ratio compared with other systemic inflammation biomarkers such as NLR, PLR, LMR, hs-mGPS, and prognostic nutritional index (PNI).
Materials and Methods
Study population
The study complied with ethical guidelines and was approved by the Independent Ethics Committee (IEC) of First Affiliated Hospital of Soochow University. A total of 556 consecutive patients who underwent PCNL for renal calculi at our institution between August 2015 and February 2018 were enrolled in our study. Patients with immunosuppressive diseases, hematopathy, tumor, preoperative fever, and a history renal failure were excluded from the study. The clinical characteristics were collected, including age, gender, body mass index (BMI), hypertension, diabetes, and stone side. All patients performed routine laboratory tests, including blood routine, urine routine, and biochemistry analysis, before surgery. Preoperative plain radiography of kidneys, ureters, and bladder and computed tomography or intravenous urography were routinely performed.
Preoperative urine culture was performed in all patients. Patients with positive preoperative urine culture were treated with a minimum 7-day course of culture-specific antibiotic therapy, whereas patients with sterile urine were administered 0.4 g of moxifloxacin, 30 min before surgery, as a standard antibiotic prophylaxis. Also, postoperative data were collected, including the development of sepsis, ICU admission, and length of stay.
Systemic inflammation biomarkers
The systemic inflammation biomarkers in this study were defined as follows. The hs-CRP/Alb ratio was calculated by dividing the hs-CRP level by the Alb level. The hs-mGPS was calculated using the hs-CRP and Alb values as follows. Patients with both hypoalbuminemia (<35 g/L) and an elevated hs-CRP level (>3 mg/L) were given a score of 2. Those who had only an elevated hs-CRP level were assigned a score of 1. The remaining patients were assigned a score of 0. 16 The NLR was defined by dividing the neutrophil count by the lymphocyte count. The PLR was defined by dividing the platelet count by the lymphocyte count. The LMR was defined by dividing the lymphocyte count by the monocyte count. The PNI was defined by the following formula: PNI = serum albumin +5 × lymphocyte count.
Endpoint
The primary endpoint for the study was the development of SIRS during postoperative hospitalization stay. SIRS was defined by two or more of the following: (1) body temperature <36°C or >38°C, (2) heart rate >90 bpm, (3) respiratory rate >20 breaths/min or PaCO2 < 32 mm Hg, and (4) white blood cell count >12 × 109 or <4 × 109 cells/L. 17
Statistical analysis
Continuous variables were presented as median and interquartile range, and were transformed into dichotomous variables at median value. Categorical variables were presented as numbers and percentages. Differences in groups were compared by using the Mann–Whitney U test for continuous variables and the chi-square test for categorical variables. The optimal cutoff value of the hs-CRP/Alb ratio, NLR, PLR, LMR, and PNI was determined by receiver operating characteristic (ROC) analysis. A univariate and multivariate logistic regression analysis was used to identify the independent factors associated with the post-PCNL SIRS. Variables significant in the univariate analysis were tested subsequently in the multivariate logistic regression.
The areas under the curve (AUC) were calculated to compare the discriminatory ability of the systemic inflammation biomarkers. The ROC analysis was performed using MedCalc statistical software version 15.2.2 (MedCalc Software bvba, Ostend, Belgium). Other analyses were performed using SPSS version 21.0 (Chicago, IL). All p-values were two tailed, and p < 0.05 was considered statistically significant.
Results
Patient characteristics
The patient characteristics are presented in Table 1. A total of 556 patients who underwent PCNL were included in the study, with 331 males (59.5%) and 225 females (40.5%). The median age was 52 (range 45–61) years. Of the total patients, 123 patients (22.1%) had developed SIRS and 22 patients (4%) had ultimately developed sepsis. All patients were divided into two groups according to the development post-PCNL SIRS. Levels of gender, urine culture, hs-CRP, albumin, leukocyte, neutrophil, lymphocyte, monocyte, hemoglobin, hs-CRP/Alb, hs-mGPS, NLR, PLR, LMR, and PNI were significantly different in the SIRS group compared with the no-SIRS group (all p < 0.05). Patients who experienced SIRS were more likely to be admitted to ICU postoperatively (21.1% vs 1.4%, p < 0.01) and had a longer length of stay (median 17 days vs 14 days, p < 0.01). Of the six patients who were in no-SIRS group admitted to ICU, the primary reasons for transfer were intraoperative hemorrhage (n = 4) and advanced age with poor conditions (n = 2). There were no significant differences with regard to age, BMI, hypertension, diabetes, stone side, stone size, creatinine, and platelet between the two groups (all p > 0.05).
Baseline Characteristics
BMI = body mass index; hs-CRP/Alb = high-sensitive C-reactive protein/albumin; hs-mGPS = high-sensitive modified Glasgow prognostic score; IQR = interquartile range; LMR = lymphocyte to monocyte ratio; NLR = neutrophil to lymphocyte ratio; PLR = platelet to lymphocyte ratio; PNI = prognostic nutritional index; SIRS = systemic inflammatory response syndrome.
Relationship between the hs-CRP/Alb ratio and post-PCNL SIRS
The optimal cutoff value of the hs-CRP/Alb ratio, NLR, PLR, LMR, and PNI was 0.06, 2.9, 129.5, 3.4, and 49, respectively, from the ROC analysis with a maximal Youden index (sensitivity + specificity −1). The results of the univariate analysis and multivariate analysis are shown in Table 2. In the univariate analysis, variables (female gender, positive preoperative urine culture, neutrophil, lymphocyte, hemoglobin, albumin, hs-CRP, NLR, LMR, PLR, PNI, hs-CRP/Alb ratio, and hs-mGPS) were associated with the development of post-PCNL SIRS. Multivariate analysis revealed that female gender (OR 1.691; 95% CI 1.045–2.735; p = 0.032), positive preoperative urine culture (OR 1.972; 95% CI 1.204–3.231; p < 0.01), hs-CRP/Alb ratio (OR 6.925; 95% CI 4.244–11.300; p < 0.01), NLR (OR 2.476; 95% CI 1.471–4.167; p < 0.01), and PNI (OR 0.559; 95% CI 0.338–0.924; p = 0.023) were independent predictors of post-PCNL SIRS.
Univariate and Multivariate Analyses for Predicting Systemic Inflammatory Response Syndrome After Percutaneous Nephrolithotomy
Relationship between the hs-CRP/Alb ratio and clinical characteristics
To further verify the relationship between the hs-CRP/Alb ratio and clinicopathologic factors, patients were categorized as low hs-CRP/Alb group (n = 346) and high hs-CRP/Alb group (n = 210) according to the optimal cutoff value. The correlations of hs-CRP/Alb ratio with clinical characteristics are shown in Table 3. The elevated hs-CRP/Alb ratio was significantly associated with female gender, positive preoperative urine culture, hs-CRP, albumin, leukocyte, neutrophil, monocyte, platelet, hemoglobin, creatinine, NLR, LMR, PLR, PNI, hs-mGPS, development of sepsis, ICU admission, and length of stay (all p < 0.05).
Correlations of the High-Sensitive C-Reactive Protein/Albumin Ratio with the Clinical Characteristics of Patients
ROC curves of the systemic inflammation biomarkers
The ROC curves were constructed and the AUC values were used to compare the predictive value of the hs-CRP/Alb ratio and other systemic inflammation biomarkers. The results are shown in Table 4. The hs-CRP/Alb ratio had a higher AUC (0.791) with a sensitivity of 76.4% and a specificity of 73.2% compared with NLR (0.669), LMR (0.633), PLR (0.594), PNI (0.629), and hs-mGPS (0.739) (Figure 1).
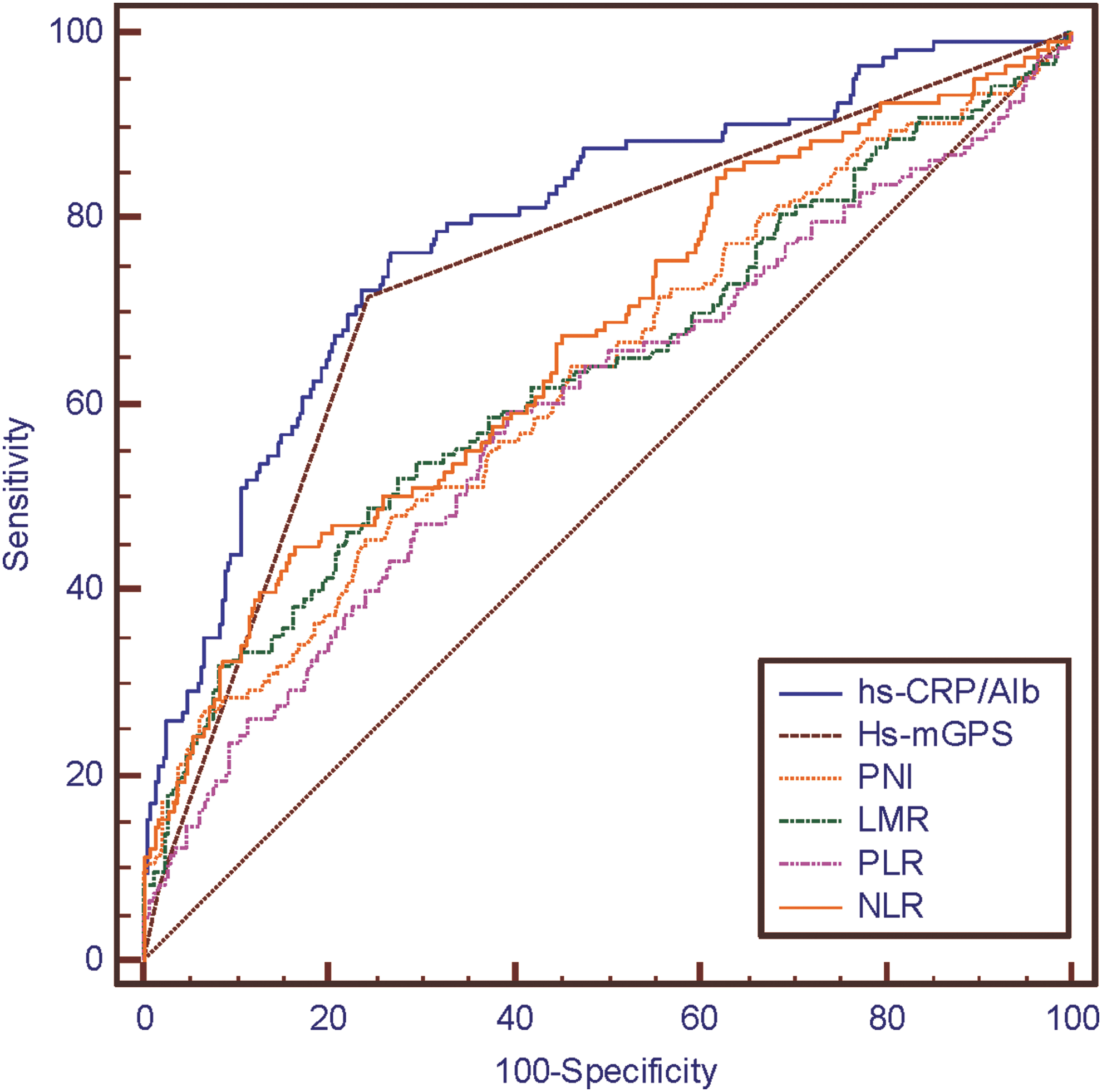
Comparison of areas under the receiver operating curves between the hs-CRP/Alb and other systemic inflammation biomarkers. hs-CRP/Alb = high-sensitive C-reactive protein/albumin.
Comparison of Areas Under the Curve Values Between the Systemic Inflammation Biomarkers
Comparison of AUC values between hs-CRP/Alb and other systemic inflammation biomarkers was done using Z test method.
AUC = areas under the curve.
Discussion
To our knowledge, this is the first study to investigate the predictive value of the preoperative hs-CRP/Alb ratio in post-PCNL SIRS. Several studies have investigated the risk factors for post-PCNL SIRS. Sharifi Aghdas et al. reported that female gender, preoperative urine culture, and nephrostomy tube insertion were associated with the development of post-PCNL SIRS. 18 Chen et al. found that number of tracts, operation time, receipt of a blood transfusion, and stone size were risk factors. 19 Liu et al. found that female gender and diabetes mellitus were independently related to post-PCNL SIRS. 20 Although previous studies have shown a few risk factors associated with post-PCNL SIRS, most of which are unobtainable before the operation. Hence, there is a great need for a preoperative predictor that has the ability to predict the development of post-PCNL SIRS.
In recent years, systemic inflammation biomarkers, including NLR, PLR, LMR, and PNI, have been a hotspot due to the advantage of being accessible and measurable. Accumulating evidence has indicated that the preoperative systemic inflammatory response is related to the presence of postoperative complications and the prognosis of patients. Tang et al. have reported that the preoperative NLR is significantly associated with post-PCNL SIRS. 9 Cetinkaya et al. also have validated the preoperative PLR as an independent factor for predicting post-PCNL SIRS. 21 In our study, the SIRS rate is 22.1%, which is similar to previous studies. 19,22 In the multivariate analysis, female gender and preoperative urine culture were important risk factors for the development of post-PCNL SIRS, identical with previous studies.
However, no relationship between diabetes and post-PCNL SIRS was observed in univariate or multivariate analysis, which was different from a previous study. The possible reasons may be as follows. Preoperative blood glucose control in diabetic patients is always one of the most important contents before surgery. All the diabetic patients in our study took hypoglycemic drugs regularly, and the blood glucose of diabetic patients was monitored three times a day. If it was obviously abnormal, the blood glucose should be monitored before and after every meal and the diabetic patients should be treated accordingly, after consulting an endocrinologist, until the blood glucose returned to normal before surgery. The blood glucose of each diabetic patient was required to be normal before surgery. Besides, it is a single-center study and large-scale multicenter studies are needed to investigate the correlation between diabetes and post-PCNL SIRS.
With regard to systemic inflammation biomarkers, the univariate analysis revealed that hs-CRP/Alb, NLR, LMR, PLR, PNI, and hs-mGPS were significantly associated with the development of post-PCNL SIRS. Furthermore, multivariate analysis demonstrated that the hs-CRP/Alb ratio (OR 6.925; 95% CI 4.244–11.300; p < 0.01), NLR (OR 2.476; 95% CI 1.471–4.167; p < 0.01), and PNI (OR 0.559; 95% CI 0.338–0.924; p = 0.023) have remained as independent predictors of post-PCNL SIRS.
CRP is an acute-phase reactant produced by hepatocytes and regulated by proinflammatory cytokines such as interleukin-6. The hs-CRP, a sensitive marker of systemic low-grade inflammation, has been reported as an independent risk factor for coronary events, 23 ischemic stroke, 24 and acute kidney injury. 25 In our institution, hs-CRP is a routine laboratory test included in the biochemistry analysis before surgery. Albumin is considered an indicator of nutritional status in patients. Hypoalbuminemia has been reported to be associated with a sustained systemic inflammatory response. 26 Combined with hs-CRP and albumin, the hs-CRP/Alb ratio has been shown to be associated with a poor outcome in patients with acute medical admissions. 27
In our study, the preoperative hs-CRP/Alb ratio has been demonstrated to be independently associated with the development of post-PCNL SIRS. In addition, we have evaluated the relationship of hs-CRP/Alb ratio with clinical characteristics. With the optimal cutoff value of 0.06, the elevated hs-CRP/Alb ratio was associated with female gender, preoperative urine culture, hs-CRP, albumin, hemoglobin, creatinine, and other systemic inflammation biomarkers. To further compare the predictive value of hs-CRP/Alb ratio with other systemic inflammation biomarkers, ROC curves were constructed. It was shown that the hs-CRP/Alb ratio has a higher AUC value (0.791) than NLR (0.669), LMR (0.633), PLR (0.594), PNI (0.629), and hs-mGPS (0.739). Thus, we thought that the hs-CRP/Alb ratio displayed superior predictive value than other systemic inflammation biomarkers.
Based on the serum concentrations of hs-CRP (cutoff value: 3 mg/L) and albumin (cutoff value: 35 g/L), the hs-mGPS has been validated as an independent prognostic factor in various malignancies. Although derived from the same variables as hs-CRP/Alb, the hs-mGPS has the potential to overestimate or underestimate the inflammatory level for the separate hs-CRP and Alb score system. 13 Some high-risk patients may be ignored by the hs-mGPS score system. In contrast, the hs-CRP/Alb ratio, as a continuous variable, combines the hs-CRP and albumin more closely, reflecting the host systemic inflammation response preferably. In the current study, 28.5% (35/123) of patients in the SIRS group were assigned a score of 0 in the hs-mGPS score system, while 23.6% (29/123) of patients were categorized into the low hs-CRP/Alb (hs-CRP/Alb <0.06). In addition, the ROC curves show that the hs-CRP/Alb ratio has a higher AUC value (0.791) than hs-mGPS (0.739).
According to our study, preoperative hs-CRP/Alb ratio is independently associated with the development of post-PCNL SIRS. The results of our study can help identify high-risk patients before surgery. Thus, high-risk patients with an elevated preoperative hs-CRP/Alb ratio should be paid more attention to and targeted for an increased duration of antibiotic prophylaxis before surgery, especially for those with negative preoperative urine culture. Appropriate nutritional support for patients with poor conditions before surgery is also necessary. In addition, surgeons should be more careful and try to lower the intraoperative and postoperative risk factors that previous studies reported, including the number of tracts, operation time, and receipt of a blood transfusion.
Although our study suggests that the preoperative hs-CRP/Alb ratio is independently associated with the development of post-PCNL SIRS, several potential limitations should be taken into account. First, our findings resulted from a retrospective, single-center study. Large-scale prospective studies are needed to validate the predictive value of the preoperative hs-CRP/Alb ratio in post-PCNL SIRS. Besides, the hs-CRP is a nonspecific inflammatory marker. Although patients with preoperative fever have been excluded from the study, the preoperative hs-CRP/Alb ratio can be elevated by factors other than infection. Finally, the current study investigates the predictive value of the preoperative systemic inflammation biomarkers for post-PCNL SIRS. Further researches should investigate the relationship of postoperative inflammation markers with post-PCNL SIRS.
Conclusions
In conclusion, our study demonstrates that the preoperative hs-CRP/Alb ratio is independently associated with the development of post-PCNL SIRS. Moreover, compared with other systemic inflammation biomarkers, the hs-CRP/Alb ratio displays superior predictive value. Based on our results, the preoperative hs-CRP/Alb ratio can be used to help clinicians identify high-risk patients and carry out targeted therapy in advance.
Footnotes
Acknowledgments
This study was supported by the National Natural Science Foundation of China (No. 81500572), The Key Discipline of Medicine of Jiangsu Province (ZDXKA2016012), the Outstanding Medical Academic Leader Program of Jiangsu Province (CXTD2017009), and the Science and Technology Key Project on Clinical Medicine of Jiangsu Province (BL2013013).
Author Disclosure Statement
No competing financial interests exist.