
Abstract
Introduction:
Percutaneous nephrolithotomy (PCNL) is the gold standard procedure for large renal calculi but postoperative (PO) pain remains a concern. Modifications of the PCNL technique and intraoperative and PO strategies have been tested to reduce pain. PO pain control reducing risk of long-term pain medication and narcotic use is of considerable importance. Acupuncture is a common medical procedure shown to alleviate PO pain. Some benefits are that it is nonpharmacologic, easy to administer, and safe. The purpose of this study was to evaluate the effects of electroacupuncture (EA) on PO pain in patients undergoing PCNL.
Materials and Methods:
This was a randomized, double-blind, sham-controlled study. The study was Institutional Review Board approved and performed under standard ethical guidelines. Fifty-one patients undergoing PCNL by a single surgeon were randomized to one of the three groups: true EA (n = 17), sham EA (SEA, n = 17), and no acupuncture (control, n = 17). The EA and SEA were performed by a single licensed acupuncturist <1 hour before operation. PCNL was performed without the use of intraoperative nerve block(s) or local anesthetic. Pain scores (visual analog scale [VAS]), narcotic use (morphine equivalents), and side effects were recorded at set intervals postoperatively.
Results:
Mean VAS scores for flank and abdomen pain were lower at all time periods in the EA compared with the SEA and control groups. Mean cumulative opioid usage was lower in the EA group immediately postoperatively compared with both SEA and control groups. Two patients in the EA group did not require any PO narcotics. No differences between groups were found for PO nausea and vomiting. No adverse effects of EA or SEA were noted.
Conclusions:
EA significantly reduced PO pain and narcotic usage without any adverse effects after PCNL. This promising treatment for managing PO pain warrants further investigation.
Introduction
Percutaneous nephrolithotomy (PCNL) is considered the gold standard procedure for removal of large renal calculi. 1 Because of the creation of a percutaneous access tract through the parenchyma and parenchymal shearing, as well as the presence of a stent or nephrostomy tube postoperatively, patients are often bothered by significant pain requiring postoperative (PO) analgesia.
Analgesic medications commonly administered postoperatively include opioid analgesics. However these medications have notable adverse effects, including nausea, decreased intestinal motility, and sedation, all of which can slow recovery. 2 Recent studies have also demonstrated that PO opioid use after various types of operation puts patients at risk for long-term addiction. 3 For patients undergoing PCNL, several adjunctive measures for pain control have been evaluated to attempt to control PO pain. These include injection of local anesthesia through the planned percutaneous tract and region anesthesia through paravertebral blocks. 4 –6
Acupuncture is one of the oldest medical procedures. It involves the insertion of small sterile needles into the body, face, head, and ear, based on documented acupuncture points. Acupuncture has been demonstrated to be an effective treatment for PO pain control for several other procedures, including thoracic, gynecologic, and orthopedic procedures and operation. 7 –10 Because of the fact that acupuncture is safe, nonpharmacologic, and a well-known pain-relieving procedure, we sought to evaluate the use of electroacupuncture (EA) for the treatment of PO pain in patients undergoing PCNL.
Methods
Ethics
Institutional Review Board (#15-0563) approval was obtained from Icahn School of Medicine, Mount Sinai Medical System, New York.
Study design
This was a randomized, double-blind, sham-control clinical trial where patients were randomized in 1:1:1 to receive true EA, sham EA (SEA), or no acupuncture (control). Anticipating a two-point difference in the pain score as measured by a 0–10 visual analog scale (VAS) score as a clinically significant difference, the power analysis indicated that an estimated sample size of 15 patients per group with α = 0.05 and power of 90%. Attrition of 10% was assumed; therefore we aimed to recruit 17 patients per arm.
Patients were randomly allocated to the EA, SEA, or control arm after opening opaque, sealed envelopes containing computer-generated random numbers. Subjects randomized to the EA and SEA cohorts were blinded and not aware of which cohort they were randomized to. Between the EA and SEA cohorts, only the person administering the acupuncture procedure and a study coordinator with no patient contact was aware of the procedure administered. All other clinicians including the surgeon and clinical staff involved in routine PO care and VAS assessment were blinded. Subjects in the control group were naturally unblinded, as they knew they did not receive the true EA or SEA procedure.
Patients
Consent for study participation was obtained from patients undergoing percutaneous management for their renal calculi before the operation date, after which they were randomized into one of the three study arms. Inclusion criteria were as follows: adult subjects between 18 and 65 years of age, able to read, understand, and sign the informed consent in the English language, agreeable to being randomized, and medically cleared to undergo elective PCNL by a single surgeon. Exclusion criteria included the following: any bleeding disorders or other coagulopathy that may increase chances of bleeding during the procedure, any skin infections at the site of the operation, inability to fill out a VAS because of physical or mental conditions, inability to use patient-controlled analgesia (PCA) because of physical or mental conditions, pregnancy, malignancy disease in the upper tract, use of any opioid-containing medication ≤48 hours before PCNL, use of acupuncture within 4 weeks of operation, current indwelling stent, use of intercostal nerve block during the procedure, and use of localized anesthetic during the surgical procedure. Figure 1 demonstrates patient flow through the study.
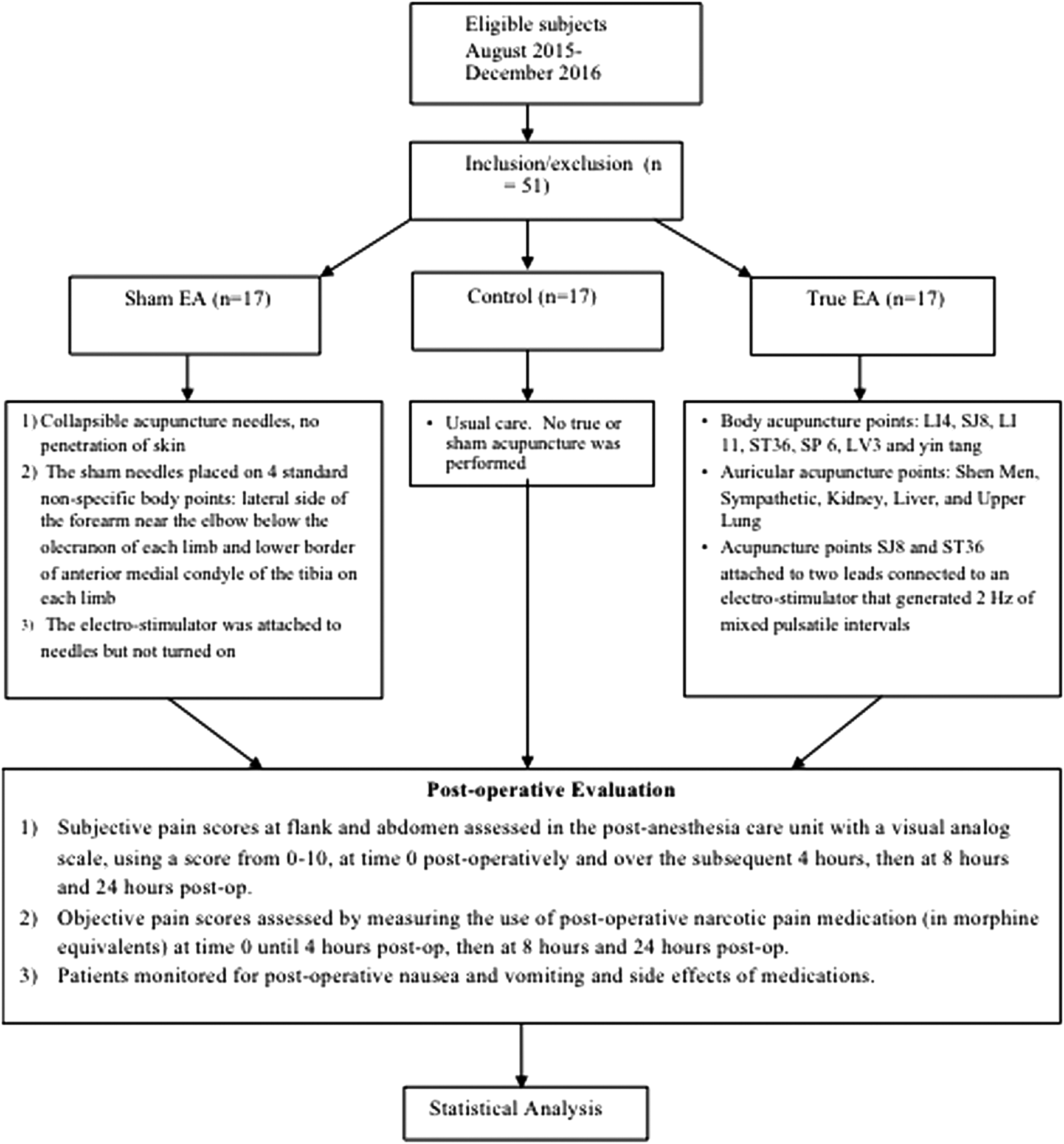
Consort study design flowchart.
PCNL procedure
At our institution a single surgeon performed PCNL in the same manner. The entire procedure was performed in the prone position. A sensor wire was placed up to the renal pelvis during flexible prone cystoscopy. An occlusion device was then deployed over the wire just proximal to the ureteral pelvic junction. Retrograde pyelogram was performed and all caliceal access was attained in the operating room by the urologist (if preexisting nephrostomy placed for obstruction did not exist). Dilatation with either a balloon device or serial dilatation was performed. Serial dilators are only used if the accessed calix was significantly impacted with stone or a preexisting used access site with tract induration is encountered. Either a Calcuson™ ultrasonic lithotripter (Karl Storz, Inc., Tuttlingen, Germany) or Stone Breaker™ pneumatic lithotripter (Cook Medical, Inc., Bloomington, IN) are used for lithotripsy. All access tract sizes were 24F. At the conclusion of the case either a nephrostomy tube, ureteral stent, or both were placed in addition to a Foley catheter in the bladder. Postoperatively, patients having pain not ameliorated by acetaminophen or toradol, oxycodone then breakthrough morphine are given in oral and intravenous (IV) forms, respectively. Some patients with allergies or intolerance to either acetaminophen or toradol were given narcotics as first-line pain medication. None of the patients required PCA. The nephrostomy was removed the morning of PO day 1 followed by the Foley catheter 1 hour later.
True EA and SEA procedure
A single licensed acupuncturist performed acupuncture <1 hour before operation in the PO area, and lasting roughly 25–30 minutes. The protocol for each group is described hereunder.
True EA protocol
All patients randomized to the true EA group received the same treatment at predetermined acupuncture points (listed hereunder) in supine position. The acupuncture protocol and procedures employed adhered to the Standards for Reporting Controlled Trials in Acupuncture (STRICTA) recommendations. 11 The protocol was selected from the standard Traditional Chinese Medicine (TCM) point prescription and informal practitioner query. Clean needle technique was used for both the true EA and SEA procedures. Stainless steel disposable acupuncture needles were inserted into skin at appropriate depth (∼3–4 mm) and the sensation of de qi was elicited. De qi is described as a warm, tingling, or aching sensation at the site of the needle. Selected acupuncture points (SJ8 and ST36) were then attached to leads connected to an electrostimulator that generated 2 Hz of mixed pulsatile intervals. The following point protocol was used for the true EA group: full body points were applied bilaterally except for yin tang-LI4, SJ8, LI 11, ST36, SP6, LV3, and yin tang. Auricular acupuncture points were applied bilaterally including, shen men, sympathetic, kidney, liver, and upper lung. “After administration of the needles in situ, the electrostimulator machine leads were attached to the needle handles and the timer was set. When the timer was finished, the machine shut off automatically. There was no additional recording of the timed procedure.”
SEA protocol
The sham acupuncture protocol consisted of superficial transverse needling of nonacupuncture points. The sham needles were placed on four standard nonspecific body points. The leads from the electrostimulator machine were then attached to the needle handles and the machine was made to look like it was turned on (i.e., a green light indicated it was on but no electrical pulse was generated) for the duration of the procedure. “After administration of the needles in situ, the electrostimulator machine leads were attached to the needle handles and the timer was set. When the timer was finished, the machine shut off automatically. There was no additional recording of the timed procedure.” The points used were superficial, nontraditional acupuncture points located on the lateral side of the forearm near the elbow below the olecranon of each limb and lower border of anterior medial condyle of the tibia on each limb. Figure 2 provides acupuncture needle locations of the true EA and SEA procedure.
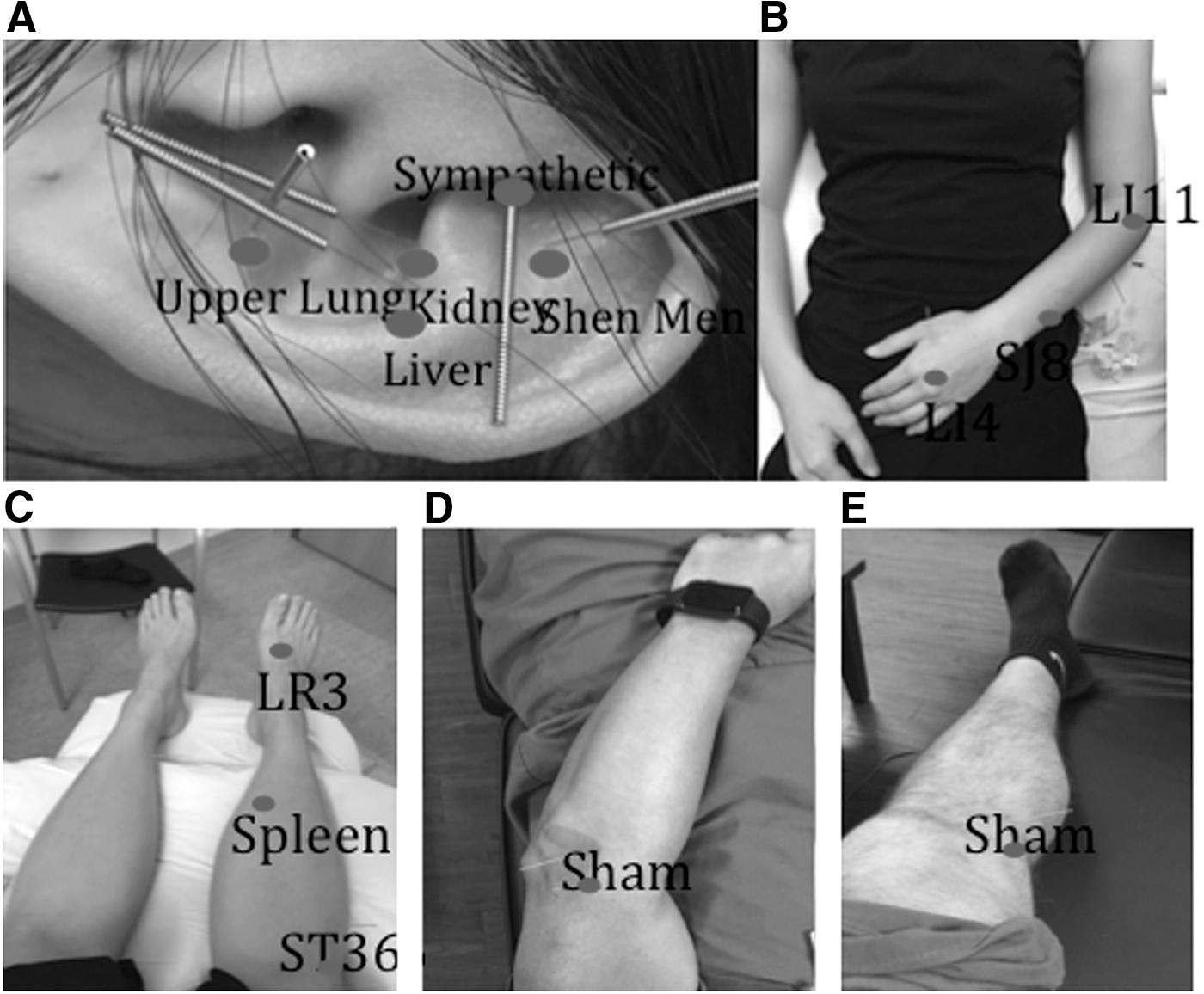
Representative images of true and sham acupuncture points.
Control group protocol
Subjects randomized to the control group were informed that they would not receive the true EA or SEA. The subjects in this arm were unblinded to the PO procedure. However after the PCNL, they were subject to the same study evaluations as the true EA and SEA groups and received the same rescue pain medications.
Safety monitoring
During true EA and SEA treatment, subjects were evaluated for vasovagal responses, intractable nausea/vomiting, bleeding, and signs of preexisting infection (skin rash, fever, chills, cough, etc.). It was predetermined that any adverse events would result in an end to a subject's participation.
PO evaluation
Subjective pain scores were assessed in the postanesthesia care unit (PACU) once the patient was awake and oriented using a VAS, with a score from 0 to 10, at time 0 postoperatively and at 60-minute intervals over the subsequent 4 hours, then at 8 and 24 hours postoperatively. The sites assessed were the site of operation (flank) and the abdomen (referred pain). The objective pain scores were also assessed by measuring the use of PO narcotic pain medication (in morphine equivalents) at time 0 until 4 hours PO and then at 8 and 24 hours PO. Patients were also assessed for incidence of PO nausea and vomiting and side effects of medications. All patients among the three cohorts had access to the same PO pain control, which is our standard protocol for patients receiving PCNL. The pain medication was administered by the anesthesia team and the PACU care team, none of whom had knowledge of subject participation in the study or whether they received acupuncture before the procedure. Statistical differences were assessed using Student's t-tests, at p < 0.05.
Results
Seventeen patients were recruited for each arm of the study, for a total of 51 patients. There were no significant differences in patient age, body mass index, gender, laterality of operation, procedure duration, size of PO nephrostomy tube, or change in hematocrit (Table 1). The rate of stent placement was higher in sham and acupuncture patients compared with control patients (53% and 59% vs 12%, respectively, p < 0.05).
Demographics and Patient Characteristics
BMI = body mass index; EA = electroacupuncture; SEA = sham EA.
Stone-free rates were determined by ultrasound and kidney, ureter, and bladder radiograph at 1-month follow-up. Stone-free rates were higher in acupuncture patients compared with sham and control patients (91.7% vs 69.2% and 61.5%, respectively, p < 0.05). No secondary procedures were necessary.
Mean VAS scores for flank in the acupuncture group (n = 17) were significantly lower at 2 hours (p = 0.02), 8 hours (p = 0.05), and 24 hours (p < 0.001) postoperatively compared with the control group (n = 17) (3.06 vs 5.18, 3.24 vs 5.18, and 1.53 vs 4.00, respectively). Pain scores were also significantly lower at 24 hours (p = 0.02) postoperatively compared with the sham group (1.53 vs 3.11). Mean VAS scores for abdomen were significantly lower in the EA group at 24 hours PO (p = 0.04) compared with the control group (0.18 vs 4.0; Table 2).
Comparison of Visual Analog Scale Results Between True Electroacupuncture, Sham Electroacupuncture, and Control Patients
VAS on 0–10 scale.
True EA vs control p < 0.05.
True EA vs SEA p < 0.05.
VAS = visual analog scale.
Mean cumulative opioid usage was lower in the EA group at time 1 hour (p = 0.04), 2 hours (p = 0.01), 3 hours (p = 0.01), and 4 hours (p < 0.04) postoperatively compared with the control group (Table 1) (0.99 vs 3.62, 1.76 vs 5.64, 2.73 vs 7.07, 4.28 vs 9.98, respectively). Two patients in the EA group did not require any PO narcotic pain medication. No differences between groups were found for Foley bother or nausea and vomiting (data not given). No patients in either the true EA or SEA groups reported pain, bleeding, or bruising at the needle insertion site or reported any other adverse effects. There were no additional complications of the PCNL in any of the study groups.
Discussion
In this prospective randomized, double-blind, sham-controlled clinical trial, we found significant reductions in PO pain and narcotic usage as measured by morphine equivalents between patients randomized to true EA vs SEA or untreated control group after PCNL for renal calculi.
PO pain after PCNL is of concern and common strategies to control PO pain include administration of intraoperative nerve block(s) and oral and intravenous analgesic medications. In the medical literature, the use of acupuncture and EA have been demonstrated to improve PO pain and reduce pain medication use after tonsillectomy in adult and pediatric patients, total knee arthroplasty, and arthroscopic shoulder operation, 12 –14 but to our knowledge there have been no randomized controlled studies of acupuncture testing PO pain control in patients undergoing PCNL.
Acupuncture is one of the oldest medical procedures. It involves insertion of small, sterile needles into the body, face, head, and ear based on a traditional medicine theory and acupuncture meridians and points on the human body. In the United States, acupuncture was acknowledged in the late 1800s in William Osler's “Principles and Practice of Medicine.” It gained more traction and interest in the 1970s after an American journalist described the impact of acupuncture on his postappendectomy recovery. To date, acupuncture is the most commonly recommended complementary medicine procedure by conventional physicians and millions of patients receive acupuncture annually in the United States, primarily for the treatment of pain-related conditions. 15 –17
The physiologic mechanisms of acupuncture needling are currently thought to work through both central and peripheral nervous system activation. First, acupuncture needling has been shown to release endorphins from the hypothalamus that are capable of binding to mu-opioid receptors. 18 More recent studies also suggest that acupuncture modulates pain pathways and areas in the cerebral cortex that play a role in pain perception such as the amygdala. 19
Acupuncture has also been shown to have an effect on the peripheral nervous system effects. It stimulates the local tissue environment that causes an inflammatory response that may affect various systemic conditions. 20 Finally acupuncture has been shown to modulate nerves that can affect the pain response such as the vagus nerve. 21
PCNL is a relatively safe and efficient method for removal of large renal calculi; however, PO pain control remains a challenge as it can cause distress, additional side effects related to oral medications such as constipation, and these often result in overall patient dissatisfaction. 22 Although commonly utilized, opioid narcotics also bear the risk of adverse effects including constipation, nausea, and put patients at risk for chronic use. 23,24
In patients undergoing PCNL, various adjunctive pain control methods have been investigated. These include infiltration of the planned percutaneous tract with local anesthetic and local nerve blocks. Many of these procedures have been shown to be effective, as authors' have noted reductions in visual analog pain scale scores. For example a recent study by Hatipoglu and colleagues compared ultrasound-guided paravertebral block (P) vs intravenous tramadol (T) for PO pain control in 53 subjects. Results demonstrated that total PCA was lower in group P vs group T (p < 0.001). Visual analog scores were also ∼2 points lower in the P vs T groups at 6, 12, and 24 hours. 25 Maghsoudi and colleagues evaluated the opioid (meperidine)-sparing effect of IV paracetamol in patients undergoing PCNL. This study randomized 100 subjects to IV paracetamol vs placebo (saline) and evaluated pain in the 24-hour period after PCNL. Patients were allowed to receive intramuscular meperidine in cases with persistent pain. Results demonstrated that pain intensity scores were significantly lower in the paracetamol vs placebo group (p < 0.001) at 6 and 24 hours. There was an approximate two-point difference in VAS pain scores between the intervention vs control group. There was also a significantly reduced usage of meperidine in the treatment group vs the control (p < 0.001). 26
Finally, investigators have noted that forgoing the percutaneous nephrostomy tube (tubeless PCNL) can lead to significant improvements in pain. Several randomized trials have been conducted that generally demonstrate decreased narcotic use and patient pain scores after PCNL. 27 However, tubeless PCNL is typically reserved for uncomplicated cases where risks of bleeding are low as it is not appropriate for all patients in particular those with large stone burden.
In our randomized, sham-controlled study, we found significantly reduced pain scores and narcotic use in patients in the true EA groups vs the sham-acupuncture group and usual care control group at various points over the 24-hour PO monitoring period after PCNL. Flank pain intensity scores were lower in the true EA vs control at 2, 8, and 24 hours and flank and abdominal pain intensity scores were lower at 24 hours in both the sham-acupuncture and control groups. Moreover there was significantly lower opioid use at 1, 2, 3, and 4 hours in the patients receiving true EA vs controls.
Limitations of our study include the inability to blind patients in the control or usual care group as those patients did consent to be in the study and were randomized to one of the three groups however new that they did not receive the intervention. Therefore those in the usual care group were most likely to be aware that they were not receiving any potentially pain-relieving intervention. Moreover, we evaluated the use of PO EA on patients undergoing PCNL. As the PCNL procedure is relatively short <120 minutes, other studies of acupuncture for PO pain have examined the administration of acupuncture in the preoperative and PO periods that may improve its therapeutic effects on pain control and/or medication usage. 28 Finally, the control group had the lowest percentage of stent placement of the three groups. Although we attempted to control for stent placement, it would be unethical to place stents if not clinically indicated. Good clinical practice dictates that ureteral stents be placed when there is worry of obstruction. Given this, stent placement even in a prospective randomized control trial is challenging. In our experience, more patients complained of ureteral stent discomfort compared with nephrostomy tube that has been studied previously. 29 If we postulate patients with stents would have increased pain and require more narcotics, then the control group we have required even more pain medication. Our results may have even been more significant if the rate of stent placement in the control group equaled that of the sham and acupuncture group.
A counterargument can be made that a double-drained system may have less pain because of less likelihood of obstruction. To prevent this, all pain scores were measured while the patients had the nephrostomy tube in place. Therefore, obstruction should not be a differentiating concern assuming proper positioning and patency of the nephrostomy tube that were verified with intraoperative antegrade pyelogram and PO output measurements. We matched all groups by having the same-sized nephrostomy tube.
Strengths of our study include its prospective, randomized, and sham-controlled design. There have been numerous methodological challenges to selecting a proper placebo/control group for interventional procedures such as acupuncture; however, the use of a sham-procedure that mimics the real procedure is well documented and described in the literature.
In conclusion true EA was superior to SEA and usual care in patients undergoing the common endourologic procedure of PCNL for renal calculi. This study demonstrates that the administration of a simple, nonpharmacologic procedure can lead to improved pain control and potentially lower usage of possibly addictive opioid-containing drugs. This is an important clinical and research question that warrants further investigation.
Conclusion
True EA significantly reduced PO pain scores and opioid use at various time points vs a sham-procedure and control in patients undergoing PCNL for removal of renal calculi. The true EA procedure was safe, easy to administer, and well tolerated. Further studies are needed to assess the effects of preoperatively administered true EA on overall costs and patient satisfaction.
Footnotes
Author Disclosure Statement
No competing financial interests exist.