
Abstract
Objective:
To determine associations between laboratory values and subsequent culture positivity in the acute ureteral calculi patient. Specifically, we aim to develop a predictive model to assist with optimization of patient outcomes and improvement of antimicrobial stewardship.
Methods:
Utilizing the electronic medical record system, we conducted a retrospective review of 3888 patients with ureteral calculi. Relevant demographic information, vital signs, and laboratory parameters obtained in the emergency department were tabulated. We applied a combination of analysis of variance and Pearson Fisher's Exact test for the analysis.
Results:
A total of 3888 patients were included in the analysis of whom 3171 (81.6%) had a negative urine culture and 717 (18.4%) had a positive urine culture. Basic vital signs and laboratory parameters, such as heart rate, temperature, white blood cell (WBC) count, platelet count, and neutrophil differential only varied slightly in the positive and negative culture groups. Urinary nitrite was found to have specificity of 97.2% with a negative predictive value of 83.7%. Urinary leukocyte esterase was found to have a sensitivity of 86.8% and positive predictive value of 46.9%. On microscopy analysis, WBCs per high power field (WBCs/hpf) varied directly with likelihood of a positive urine culture; >150 WBCs/hpf had an 86.1% likelihood of positive urine culture.
Conclusion:
With the data provided from this large cohort analysis, we were able to create the ureteral calculi urinary culture calculator. With this calculator, urologists are better equipped to stratify a patient's risk of having a positive urine culture in the setting of a ureteral calculus.
Introduction
U
Although deviations of baseline creatinine and evidence of hydronephrosis on imaging are often used as surrogates for determining obstruction, diagnosing infection is more challenging. With urine cultures taking >24 hours, physicians heavily rely on clinical intuition to determine which patients require emergent intervention. Although the treatment algorithm for a septic patient with an obstructed and infected urinary system is well described, 3 stable patients with subtle deviations in laboratory parameters are more problematic. There have been attempts to identify objective values to determine patients who would likely benefit from early intervention, with equivocal results. 4 In addition, prediction models have been developed to assist in determining likelihood of ureteral stone intervention. Moore, et al. defined the STONE scoring system to predict the likelihood of adverse findings in acute uncomplicated calculus patient. 5 Tran et al. created the Emergency Ureteral Stone Treatment score to stratify patients who are likely or unlikely to have successful treatment outcomes. 6 Despite these scoring systems, there remains a void for an objective measurement tool that determines the likelihood of predicting positive urine cultures in the presence of ureteral calculi.
Furthermore, with the increasing prevalence of antibiotic resistant microbes, the necessity for avoidance of unnecessary antibiotics is paramount. Ureteral calculi patients are no exception to this epidemic. 7 Oftentimes, physicians will prescribe antibiotics before discharge from the emergency department because we cannot predict the patients who will have a positive urine culture. If physicians are better equipped to discern patients who will have a negative urine culture in the setting of a ureteral calculi, inappropriate antibiotic administration would decline.
The aim of this study is to determine associations between laboratory values and subsequent culture positivity in the acute ureteral calculi patient. Specifically, we aim to develop a predictive model to assist with optimization of patient outcomes and improvement of antimicrobial stewardship.
Methods
We utilized the electronic medical record (EMR) at our institution to conduct a retrospective chart review. The review included the most common demographic information, vital signs, and laboratory parameters obtained at our institution's emergency department. For the entirety of the cohort, basic laboratory work-up for all suspected ureteral calculi patients included urinalysis, urine culture, basic metabolic panel, complete blood count, and computed tomography (CT) scan. Urinary leukocyte esterase is interpreted by three values at our institution—none, small, and large. Leukocyte esterase was deemed positive if the result showed small or large leukocyte esterase. Positive urine cultures were defined as a single bacterial organism with >10,000 colony forming units in the setting of a ureteral stone.
We searched our institution's EMR for a diagnosis of ureteral calculi based on ICD 9 and 10 codes from January 1, 2009, to August 1, 2017. Exclusion criteria included patients who were younger than 18 years old, patients without necessary laboratory values and urine cultures that were contaminated, or had polymicrobial growth. A total of 4339 patient records were obtained. After applying the exclusion criteria, a total of 3888 patients were eligible for analysis.
The primary endpoint of the study is to determine which parameters present an increased likelihood of a positive urine culture in the setting of a ureteral calculus. The secondary endpoint is to create the ureteral calculi urinary culture (UCUC) calculator as an equation to determine the likelihood of a negative or positive urine culture based on our data. This was created based on a canonical discriminate function analysis and prediction model. The parameters were chosen based on clinical applicability and statistical strength of the canonical discriminant function coefficients. The parameters utilized are gender, urinalysis LE, urinalysis white blood cell (WBC) count, and urinalysis nitrite. The cut point of 6 for a positive test was set because this allowed the maximization of accuracy in both the positive and negative growth groups.
Data were analyzed using means and standard deviations for continuous variables. Means were compared using analysis of variance. Categorical variables were further examined using Pearson Fisher's Exact tests. Sensitivity, specificity, positive predictive value, and negative predictive values for urinary nitrate and leukocyte esterase were obtained by comparing respective urinary values to positive and negative cultures.
Results
Patient demographics
Of the 3888 patients included in the analysis, 3171 (81.6%) had a negative urine culture and 717 (18.4%) had a positive urine culture. Caucasians represented 3487 (89.7%) patients and non-Caucasians represented 401 (10.3%) patients. Gender was represented almost equally, with 2177 (56%) men and 1711 (44%) women. Nondiabetic patients represented 3591 (92.4%) and diabetic patients represented 297 (7.6%).
Subgroup analysis (Table 1)
On subgroup univariate analysis, women were found to have an increased likelihood of positive urine culture at 35.4% vs 5.1% in men (p < 0.001). Non-Caucasians were found to have an increased likelihood of positive urine culture at 23.4% vs 17.9% in Caucasians (p < 0.006). Patients with diabetes were also found to have an increased likelihood of positive urine culture at 20.5% vs 18.3% in nondiabetic patients, although this was not statistically significant (p = 0.332).
Comparison of Positive and Negative Cultures with Objective Laboratory Parameters
LE = leukocyte esterase, WBC = white blood cell.
There was no difference in patient age and urine culture results (p = 0.085). Heart rate was elevated in the positive culture group with an average of 86 beats per minute (bpm) vs 78 bpm in the negative culture group (p < 0.001). Temperature was higher in the positive culture group with an average of 98.23°F (36.8°C) vs 98.02°F (36.7°C) in the negative culture group (p < 0.001). The serum WBC count was higher in the positive culture group with an average of 11.2 (10 3 /μL) vs 10.2 (10 3 /μL) in the negative culture group (p < 0.001). The WBC differential was higher in the positive culture group with an average of 71.2% neutrophils vs 69.3% neutrophils (p < 0.001). The platelets were higher in the positive culture group with an average of 251 (10 3 /μL) vs 235 (10 3 /μL) in the negative culture group (p < 0.001). Creatinine was lower in the positive culture group with an average of 1.07 (mg/dL) vs 1.14 (mg/dL) in the negative culture group (p < 0.001). Blood pressure was lower in the positive culture group with an average of 142/85 mmHg vs 146/89 mmHg in the negative culture group (p < 0.001).
Urinary parameters
In the setting of ureterolithiasis, urinary nitrite was found to have a sensitivity of 16.7%, specificity of 97.2%, positive predictive value of 57.7%, and negative predictive value of 83.8% in predicting a positive culture. Urinary leukocyte esterase was found to have a sensitivity of 86.8%, specificity of 77.8%, positive predictive value of 46.9%, and negative predictive value of 96.3%. On urine microscopy, there was a correlation with the number of WBCs per high power field (WBCs/hpf) and the increased likelihood of a positive urine culture. When, respectively, looking at the most commonly recorded values of WBCs/hpf, 0–4, 5–10, 11–20, 21–50, 51–150, and >150, there was a 4.7%, 33%, 51.2%, 58%, 75.9%, and 86.1% likelihood of positive urine culture (Fig. 1).
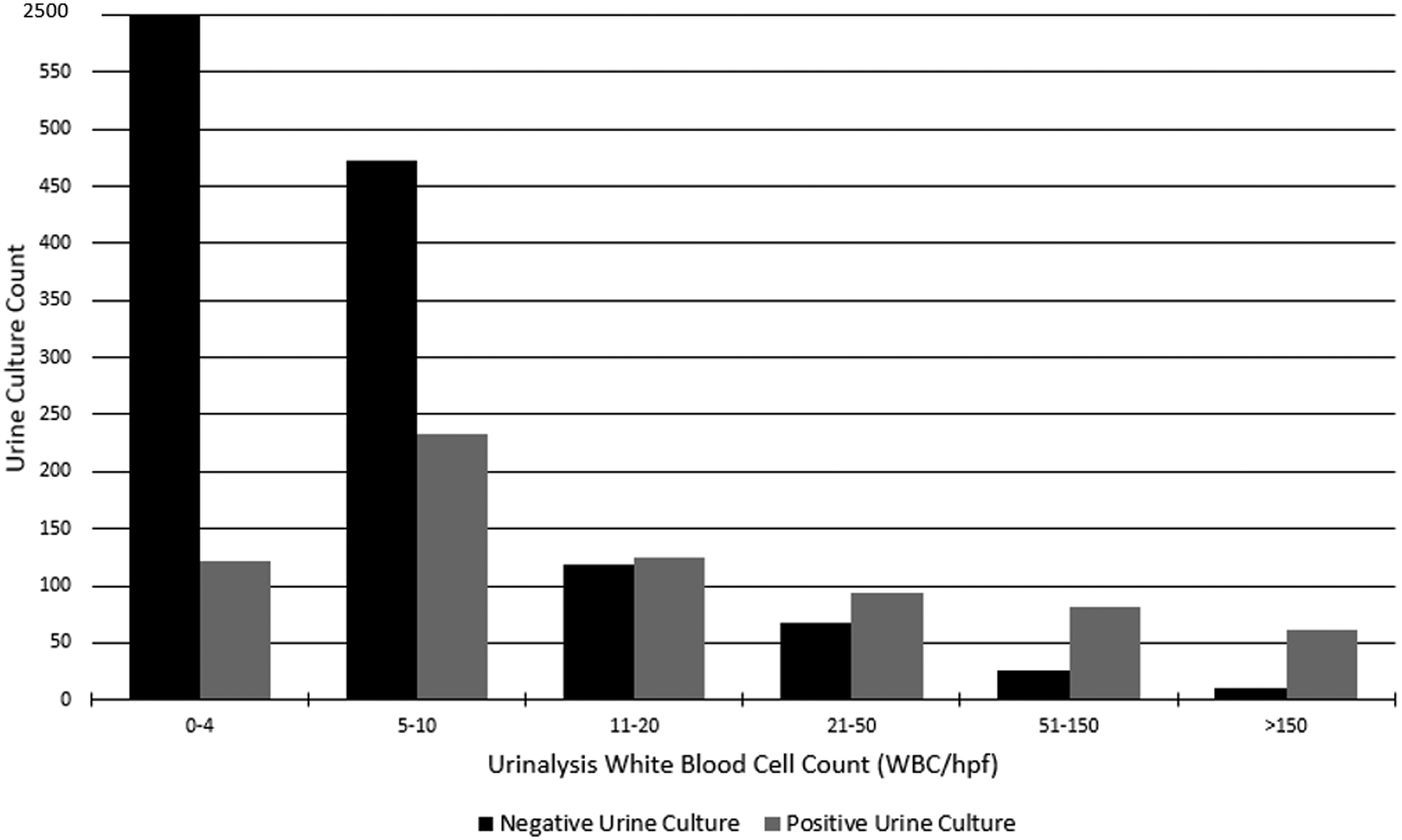
Urinalysis WBC count and corresponding likelihood of positive vs negative urine culture. WBC = white blood cell.
The UCUC calculator
The UCUC calculator was created using a discriminate function analysis and prediction model to determine the likelihood of negative and positive urine cultures based on the most influential parameters (Table 2). The parameters decided upon were gender, urinalysis LE, urinalysis WBC count, and urinalysis nitrite (Fig. 2). The calculator is able to successfully predict urine culture positivity or negativity in 87% of cases. The cut point for a positive urine culture is a total score of 6 or greater.

Equation to determine urine culture.
Ureteral Calculi Urinary Culture Calculator Scoring System
LE = leukocyte esterase, WBCs/hpf = white blood cells per high power field.
Discussion
Ureteral stones in the setting of an infection can result in significant patient morbidity. Consistent with other studies, we have found that approximately one in five patients will have a positive urine culture in the setting of a ureteral calculi. 8 This represents a substantial population that could be at risk for urosepsis.
All patients presenting to the emergency department with signs and symptoms of ureteral calculi will receive a basic work-up including vital signs, urinalysis, and laboratory panels. Based on our results given in Table 1, we found that heart rate, temperature, blood pressure, WBC count, and percentage of neutrophils and platelets have a large amount of statistical significance; however, the clinical significance remains uncertain. For example, the difference in WBC count only varied minimally and it would be difficult to extrapolate a positive urine culture over a negative culture based on a one point difference. This was corroborated in a study done by Morrison et al., wherein they found the positive predictive values of Systemic inflammatory response syndrome criteria (heart rate >90 bpm, body temperature >38°C or <36°C, respiratory rate >20 breaths per minute, and WBC count >12,000/mm 3 or <4000 mm 3 ) were not significantly clinically associated with a septic calculus. 8 This was also confirmed in a study by Kamei and colleagues 9 that looked at risk factors for septic shock in acute obstructive pyelonephritis. In their data set, they evaluated the same parameters as in our study. Although they found that thrombocytopenia was an independent risk factor for septic shock, the variance between septic patients and stable patients was not great enough to have clinical utility. 9 Overall, our results showed statistical significance, but the clinical significance is not apparent. Based on this, it is difficult to correlate a positive urine culture with mild deviations in serum parameters and vital signs.
Conversely, we have found the urinary parameters have a much better predictive value on patients that will ultimately have a positive urine culture as our results showed clinical and statistical significance. A common clinical vignette in the emergency department is an acute calculi patient with stable vital signs and a mild leukocytosis that presents with leukocyte esterase positive and nitrite negative urine. Coupled with a mildly elevated creatinine and evidence of hydronephrosis on CT, this is often diagnosed as an infected ureteral stone.
Leukocyte esterase is a measurement of WBC byproducts in the urine and can be elevated by inflammation or infection. In contrast, urinary nitrite is a parameter that measures Gram negative organisms in the urine, the most common etiology of urinary tract infections. With a positive predictive value of 47%, urinary leukocyte esterase is a poor test to determine whether a patient will have a positive urine culture. Alternatively, urinary nitrite is a great indicator of predicting a negative urine culture. With a negative predictive value of 84% and a specificity >97%, we can say with high confidence that nitrite negative urine in the setting of a ureteral calculi is unlikely to have a positive urine culture. This was consistent with a study completed by Koeijers et al. 10 In this study, they looked at urinary tract infections in men and found that urinary nitrite had a specificity of 98%. 10 Although there are exceptions to the rules, if a patient is medically stable, only has slight elevations in baseline creatinine, and is amenable to conservative management, based on our data, there is low likelihood of a positive urine culture when urinary nitrite is negative.
Another way to assist with determining whether a patient will have a positive urine culture is urine microscopy. WBCs on urine microscopy result from two separate sources: infection or inflammation. Based on Figure 1, increasing number of WBCs/hpf portends a higher likelihood of infection. For example, at >50 WBCs/hpf, there is more than a 75% likelihood of culture positivity, but when the WBCs/hpf is <10, there is only a 33% likelihood that it is due to an infection.
As discussed by Borofsky and coworkers, surgical decompression is associated with decreased mortality in patients with sepsis and ureteral calculi. 3 The authors noted the lack of evidence-based recommendations to determine when surgical decompression is warranted. Obstructing infected ureteral calculi represent one of the instances where immediate decompression is necessary. With urine cultures taking >24 hours, urologists are required to make decisions on what circumstances constitute an infected ureteral calculi. Relying on clinical suspicion over objective evidence can lead to misdiagnosis, increased hospital costs, and patient morbidity. By falsely diagnosing an infected calculus, this exposes the patient to the risks of anesthesia and surgery, unnecessary antibiotics, and increases hospital expenditures. In contrast, misdiagnosis of an uncomplicated ureteral calculi exposes the patient to morbidities associated with sepsis. This highlights the delicate balance of clinical decision-making and further defines the necessity for evidence-based recommendations. To help fill the void in the urologic literature, the UCUC calculator was developed. Utilizing a discriminate analysis and prediction model, the calculator is able to determine the likelihood of positive urine culture in the setting of a ureteral calculi with 87% certainty (Fig. 2). The values incorporated into the scoring system included gender, urinalysis LE, urinalysis WBC count, and urinalysis nitrite. If the score is ≤5, the culture is read as negative. If the score is ≥6, the culture is read as positive. With a calculator that nears 90%, this provides a reliable tool that immediately assists in patient decision-making. This not only provides prompt direction for treatment, but also helps differentiate the subset of patients who would benefit from antimicrobial therapy.
There are limitations to the presented study. First, the retrospective nature of the study introduces inherent biases and flaws. For instance, we are unable to control for potential confounding comorbidities leading to abnormal laboratory values. Furthermore, we are not able to control for patients who could have been on antibiotics for unrelated comorbidities before evaluation in the emergency department. In this instance, this would lead to culture negativity because the patient was on antibiotic therapy before evaluation. In addition, the calculator was created as a tool to assist in clinical decision-making. Despite the calculator reaching 87% certainty of culture results, that leaves 13% of patients who could potentially be misdiagnosed based on the calculator alone. It is always important to take into account the entire patient presentation and not discounting clinical intuition. Ultimately, a prospectively designed study is required to validate the presented calculator. This would allow for control of potential confounding variables and increase the validity of the scoring system.
Aside from the limitations to the study, a population of almost 4000 patients represents the largest documented analysis evaluating urine cultures in the presence of ureteral calculi. The population size provides a large amount of statistical significance to its values. In addition, the study does not rely on subjective information to make conclusions; we are able to make evidence-based evaluations centered on objective data. Furthermore, given the community setting of our institution, our results are generalizable to other community-based hospitals. Finally, we are able to help promote antimicrobial stewardship within our urologic community, a problem that has become increasingly apparent. 7
Conclusion
This study represents a large subset of patients, which has shown that approximately one of every five patients with a ureteral calculus will have a positive urine culture. Basic vital signs and serum laboratory parameters showed no clinical significance when comparing positive and negative urine cultures. However, urinary parameters, such as urinary nitrite positivity and number of WBCs/hpf, were most important in determining the likelihood of a positive urine culture. Utilizing these data, the UCUC calculator was designed to assist in clinical decision-making and proper antimicrobial stewardship.
Footnotes
Author Disclosure Statement
No competing financial interests exist.