
Abstract
Objective:
To evaluate whether reducing the dose of fluoroscopy to ¼ of standard dose during unilateral ureteroscopy for ureteral stone treatment would impact in a reduction of total radiation emitted and whether this strategy would impact operation time, stone-free rate, and complication rate.
Methods:
From August 2016 to August 2017, patients over 18 years submitted to ureteroscopy for ureteral stone between 5 and 20 mm were prospectively randomized for ¼ dose reduction or standard dose fluoroscopy. Patients with abnormal urinary anatomy such as horseshoe kidney, pelvic kidney, or duplex system were excluded from the study.
Results:
Ninety-four patients were enrolled. The fluoroscopic dose reduction strategy to ¼ of the standard dose was able to significantly reduce the cumulative radiation emitted by C-arm fluoroscopy and the dose area product (3.6 ± 4.5 mGy vs 16.2 ± 19.3 mGy, p = 0.0001 and 0.23 ± 0.52 mGym2 vs 1.15 ± 2.74 mGym2, p = 0.02, respectively). Fluoroscopy time was similar between groups (74.5 ± 84.8 seconds vs 88.3 ± 90 seconds, p = 0.44). There was no need to increase the fluoroscopy dose during any of the procedures. Surgical outcomes were not affected by fluoroscopic dose reduction strategy.
Conclusion:
Low dose fluoroscopy reduces the emitted radiation during ureteroscopy without compromising surgical outcomes.
Introduction
Several studies support an association between increasing exposure to radiation and increasing cancer risk. 1,2 Also, it is known that the deleterious effects of radiation are cumulative. 2,3 Patients with urinary stone disease are at radiation risk due to its recurrent condition that requires multiple image diagnostic studies like computed tomography (CT) and fluoroscopy guided procedures for treatment. 4 –6 Typical radiation exposure for a patient submitted to ureteroscopy ranges from 2.5 to 100 mSv. 7 The annual occupational radiation exposure limit is no more than 50 mSv per year. 8 Therefore, urologists are encouraged to use less fluoroscopy by adhering to the “as low as reasonably achievable” (ALARA) policy. 9 Despite the use of protective equipment, endourologists are at risk of radiation too because of the frequent exposure to fluoroscopy and the proximity to the source of radiation. 10,11
Our aim was to evaluate whether reducing the dose of fluoroscopy to ¼ of the standard dose during unilateral ureteroscopy for ureteral stone treatment would impact in a reduction of total radiation emitted. Also, to evaluate whether this strategy would impact operative time, stone-free rate, and complication rate owing to less than optimal fluoroscopy image.
Materials and Methods
From August 2016 to August 2017, all patients over 18 years diagnosed with ureteral stone from 5 to 20 mm in diameter by CT were counseled about different treatment options and those willing to be submitted to ureteroscopy were randomized 1:1 using
Patient demographics including age, gender, body mass index (BMI), abdominal waist, abdominal thickness, and American Society of Anesthesiologists score were recorded. All patients had preoperative CT reviewed by a single radiologist blinded for groups and stone features were recorded. Operative parameters as operative time, fluoroscopy time, cumulative radiation, and dose area product (DAP) were also recorded. Ureteroscopy outcomes analyzed were failed ureteroscopy, stone-free rate, ureteral lesion, ureteral stenosis, hospitalization time, and Clavien morbidity score. Procedure failure was defined as impossible to reach the ureteral stone by ureteroscopy.
All patients were operated in a dedicated Olympus surgical room (Evis Exera II; Olympus, Hamburg, Germany) using C-arm fluoroscopy (BV Endura; Philips Medical Systems, Veenpluis, Nederlands). The C-arm recorded fluoroscopy parameters for each procedure. It has automated kV and mAs parameters that vary according to object thickness, density, and distance to the X-ray intensifier. The mAs was adjusted manually to ¼ of the standard dose to obtain the dose reduction for this study.
The concept of ALARA for fluoroscopy was adopted as standard in all cases using last image-hold, pulsed fluoroscopy, surgeon foot pedal controlled fluoroscopy, and optimization of patient distance from X-ray intensifier. Collimation was not used in this study. Ureteroscopy was performed under general anesthesia, in lithotomy position, by four different experienced urologists blinded for fluoroscopy dose used in each case. Operating room staff was protected with lead aprons and thyroid shields. An open-ended 5F ureteral stent was placed in the ureteral orifice for a pyelography and 0.035′′ hydrophilic guidewire was positioned in the kidney under fluoroscopic guidance. Stone dusting or fragmentation was achieved with a 270-μm fiber Holmiun LASER (Medilas H 20; Dornier MedTech GmbH, Wessling, Germany) and stone fragments were removed with a four wire stone basket. Double J stent was placed at surgeon discretion and removed after 7–28 days.
Ureteral lesion was recorded by direct vision of the ureteral wall using post ureteroscopy lesion scale (PULS) grade. 12 Postoperative (PO) low dose CT was performed at 3 months to identify residual stone and hydronephrosis. Patients were considered stone free if no residual stones were found at PO CT, reviewed by the same radiologist blinded for groups allocation. Diagnosis of ureteral stenosis was suspected by a combination of persistent lumbar pain and hydronephrosis on CT. The confirmation of stenosis was made by diethylenetriaminepentaacetic acid renal scan.
Sample size was calculated based on the efficacy of dose reduction strategy. The cumulative radiation (mean ± standard deviation [SD]) was 22.08 ± 17.35 mGy in a group of 12 previous ureteroscopies with standard dose. We considered a reduction of 40% in cumulative radiation with the reduction dose strategy, a significance level of 0.05, and a test power of 0.80 for a monocaudal Student t test. As a result, the sample size for each group was 47 patients.
Results
Demographic data and stone features were similar between groups (Table 1). The fluoroscopic dose reduction strategy to ¼ of the standard dose was able to significantly reduce the cumulative radiation emitted by C-arm fluoroscopy and the DAP (3.6 ± 4.5 mGy vs 16.2 ± 19.3 mGy, p = 0.0001 and 0.23 ± 0.52 mGym2 vs 1.15 ± 2.74 mGym2, p = 0.02, respectively). Moreover, fluoroscopy time was similar between groups (74.5 ± 84.8 seconds vs 88.3 ± 90 seconds, p = 0.44) (Table 2) and there was no need to increase the fluoroscopy dose during any of the procedures. None of the surgeons asked for a better image or complained about the quality of the image provided In any case. Table 3 shows that surgical outcomes were not affected by fluoroscopic dose reduction strategy. Stone-free rate was similar between groups (93.6% vs 91.5%, p = 0.69). Surgical complications were also not compromised. PULS grade (p = 0.64) and ureteral stenosis (one each group, p = 0.55) were similar between groups. We also performed a subanalysis between groups of the 41 patients with BMI ≥30 kg/m2 from our study. Cumulative radiation was significantly less in ¼ of the standard dose group. Fluoroscopy time was similar between groups (71.7 ± 71 seconds vs 79.7 ± 79.4 seconds, p = 0.73). The fluoroscopy dose reduction strategy was able to maintain surgical outcomes also in the obese patients. The stone-free rate was similar in both groups (88.9% vs 95.7%, p = 0.7) and no ureteral stenosis were demostrated (Table 4).
Patient's Demographics and Preoperative Computed Tomography Stone Features
ASA = American Society of Anesthesiologists; BMI = body mass index; SD = standard deviation.
Fluoroscopy Parameters
Ureteroscopy Outcomes
Subanalysis of the Forty-One Patients with Body Mass Index ≥30 kg/m2
Discussion
This study is a double-blind randomized clinical trial that demonstrates low dose fluoroscopy is safe and effective for performing ureteroscopy.
Ionizing radiation emitted by radiological imaging studies as CT and fluoroscopy used for diagnosis and treatment of urolithiasis can damage human cells and cause cancer. According to the Biological Effects of Ionizing Radiation Committee, there is a linear, no-threshold dose–response association between exposure to ionizing radiation and the development of cancer. 13 Therefore, strategies to reduce the exposure to ionizing radiation while maintaining diagnostic and treatment outcomes should be encouraged.
Radiation exposure during ureteroscopy is significant and equivalent to that of an abdominopelvic X-ray study. 14 Radiation exposure can be reduced decreasing the fluoroscopy time, but usually this strategy demands expertise that is accomplished only with experience. 15,16 Also, time reduction may not reflect in reduction of cumulative radiation delivered because this depends on fluoroscopy dose. 17 Other measures to reduce radiation during fluoroscopy are last image-hold, pulsed fluoroscopy, surgeon foot pedal controlled fluoroscopy, low dose setting, and optimization of patient distance from X-ray source and intensifier. 10 Even the simple feedback of how much fluoroscopy the surgeon is using may reduce the radiation exposure. 18 One of the most effective strategies to decrease radiation exposure during ureteroscopy is to use low dose. However, the quality of the image obtained is inferior to standard dose image (Fig. 1). The main concern is to maintain the stone-free and complication rates despite the inferior quality of image obtained.
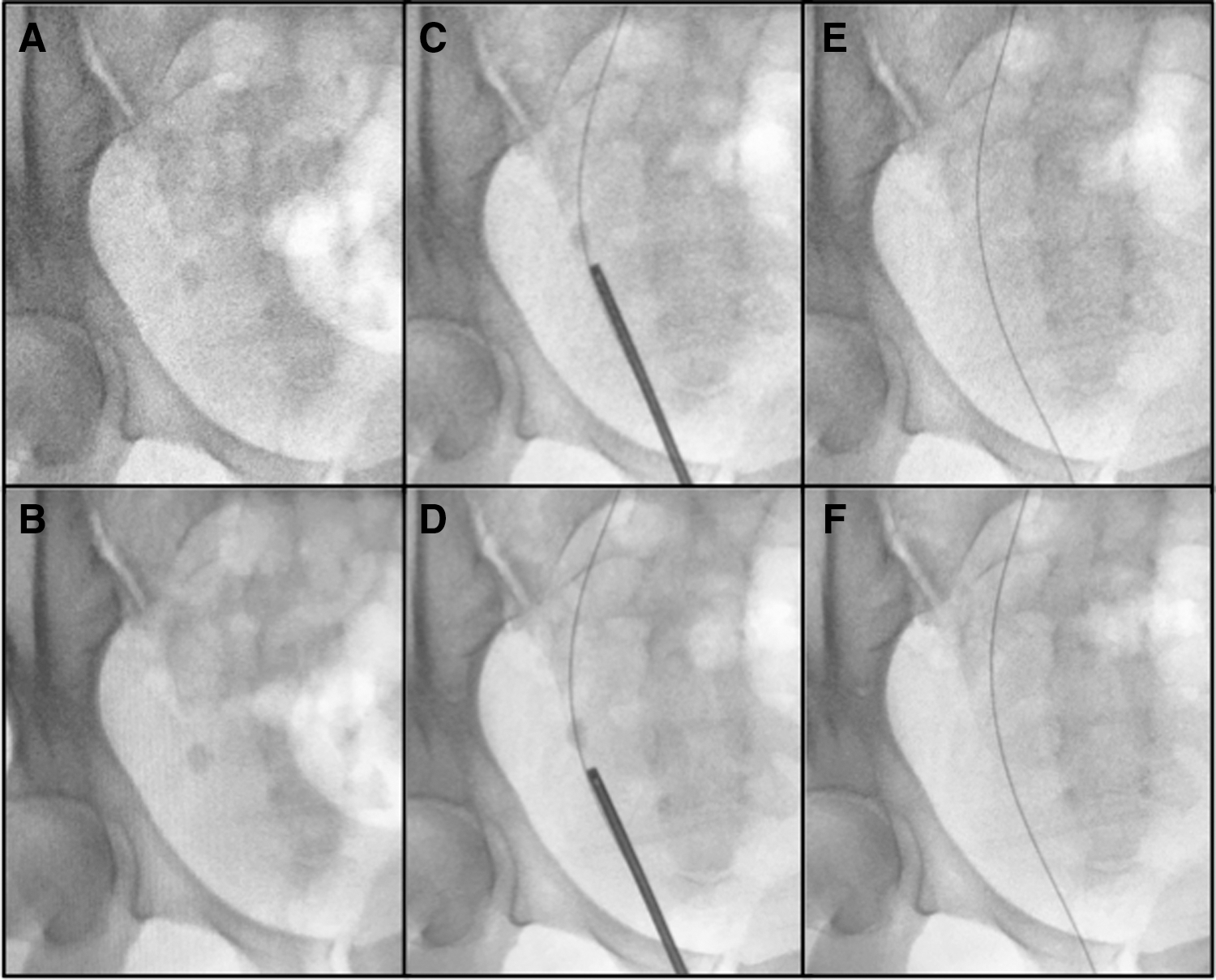
Subtle differences between ¼ and standard dose fluoroscopy during ureteroscopy.
We studied the effects of reducing the fluoroscopy dose during unilateral ureteroscopy for ureteral stone treatment to ¼ of the standard dose. This is a very simple strategy and can be accomplished by adjusting the settings of the C-arm. We selected patients with ureteral stone only to keep the uniformity of the study as other authors already published that renal stones are associated with 27% higher radiation exposure compared to ureteral stones. 19 Our study randomization warranted that groups were comparable regarding body habitus as BMI, abdominal waist, and abdominal thickness, since it is known that obesity is associated with higher radiation dose rates under fluoroscopy. 20,21
Our results demonstrated a significant reduction in cumulative radiation emitted by C-arm fluoroscopy and DAP while maintaining similar stone-free rate, operative time, hospitalization time, and complication rate. Although the quality of the image generated by ¼ dose is inferior to the standard dose, there were no cases in which one of the four different surgeons asked for an increase in the fluoroscopy dose. Also, fluoroscopy times were similar between groups. Therefore, the images were equally adequate to perform the procedure.
The most important measure of radiation exposure is DAP expressed in Gray square centimeters (Gycm2). It correlates to overall malignancy risk. 17 The ¼ dose reduction in fluoroscopy was able to reduce DAP roughly to 1/5 (0.23 ± 0.52 mGym2 vs 1.15 ± 2.74 mGym2, p = 0.02).
We also performed a subanalysis of the 41 (43.6%) patients with BMI ≥30 kg/m2. We were able to demonstrate a reduction in the cumulative radiation in the ¼ dose group. The dose reduction strategy maintained surgical outcomes in obese patients demonstrating that it is safe and effective also in this group of patients.
We expected to observe higher cumulative dose and DAP in patients with BMI ≥30 kg/m2 than in overall group because more radiation is needed to produce fluoroscopic images in thicker objects as patients with higher BMI. However, we would like to highlight that the difference was not statistically significant (Overall standard dose vs BMI ≥30 kg/m2 standard dose: mean cumulative radiation ± SD, mGy, 16.2 ± 19.3 vs 13.8 ± 14.5, p = 0.481 and mean DAP ± SD, mGym2 1.15 ± 2.74 vs 0.76 ± 1.2, p = 0.314). It is possible that other studies with larger groups would clarify this matter.
This strategy should also be tested in different procedures as retrograde intrarenal surgery (RIRS) and percutaneous nephrolithotomy to verify whether the expected inferior quality of the images could have an impact on stone-free rate and complications in these more challenging procedures. Other authors evaluated the impact of the adoption of a low dose protocol during RIRS in a retrospective study and demonstrated a continuous reduction of the amount of radiation used over the years without compromising surgical outcomes. 22
Olgin et al. retrospectively compared fluoroscopy assisted to no fluoroscopy ureteroscopy and concluded for the feasibility of this zero radiation technique. 23 However, complications may occur during surgery and it is wise to have the C-arm ready and set to ¼ dose to use in a very low threshold.
Our study has several strengths. It is a randomized clinical trial, using index patients for a very straightforward procedure of the urological practice performed by four different surgeons and the results were verified by the gold standard image tool for urolithiasis. We do not recommend CT for follow-up after ureteroscopy. We used low-dose CT in this particular study to have the best evidence possible to prove our hypothesis.
The weak point of this study is its single-center nature. Other multicentric prospective studies are needed to confirm our findings.
Conclusion
Low dose fluoroscopy reduces the emitted radiation during ureteroscopy without compromising surgical outcomes.
Footnotes
Acknowledgment
Fundação de Amparo à Pesquisa do Estado de São Paulo 2014/05130-2.
Author Disclosure Statement
No competing financial interests exist.