
Abstract
Objectives:
To determine if self-visualization of ambulatory cystoscopy provides a decrease in pain perception in male and female patients.
Methods:
A quasi-randomized controlled trial involving patients scheduled for ambulatory cystoscopy from August to November 2017. The indications were: hematuria, bladder cancer surveillance, lower urinary tract symptoms, and incontinence. The patients were quasi-randomized into two groups by scheduled date. Both groups received the same explanation before and during cystoscopy. The variables analyzed were gender, age, Visual Analog Scale (VAS) score, number of previous cystoscopies, and indication and positivity of the test for bladder neoplasia. All patients were analyzed by group and gender separately. The statistical tests used were: Wilcoxon rank-sum, Kruskal–Wallis, Mann–Whitney U test, Pearson correlation, and linear regression.
Results:
Four hundred four patients were included (318 males and 86 females) and divided into two groups, group A (no self-visualization, n = 239) and group B (self-visualization, n = 165). In males, mean VAS score was 2.6 for group A and 2.5 for group B (p = 0.276); in females, VAS score was 2.78 for group A and 1.64 for group B (p = 0.008). Regarding the remaining variables analyzed, neither positivity of the test for neoplasia (p = 0.14) nor cystoscopy indication (p = 0.597) had any influence. In patients with two or more previous cystoscopies, a reduction in mean VAS score was seen in both genders. In males having their first cystoscopy the mean VAS score was 3.1 and decreased to 2.1 for the third or more (p = 0.001); in females the mean VAS score was 2.89 for the first and 1.56 for the third or more (p = 0.02), although this benefit tended to disappear when the number of previous cystoscopies was taken into account.
Conclusion:
In male patients, self-visualization of cystoscopy did not impact pain perception, while in female patients, it seemed to provide a benefit. The number of previous cystoscopies had an influence, diminishing the perception of pain, regardless of whether the patient visualized the procedure or not.
Introduction and Objectives
Cystoscopy as a diagnostic procedure is performed frequently and generally in an outpatient setting. The procedure is usually well tolerated, causing mild to moderate pain. 1
Since cystoscopy is used for the surveillance of non-muscle invasive bladder cancer (NMIBC), which is characterized by its high rate of recurrence and prolonged follow-up (every 3–4 months for ≥5 years in tumors of intermediate or high risk), 2,3 many patients will undergo multiple cystoscopies throughout their lives.
Given that many of these patients will face multiple cystoscopies, many interventions have been proposed to decrease pain perception and increase tolerance to this procedure, from holding the patient's hand or using TENS (transcutaneous electrical nerve stimulation), to listening to classical music during cystoscopy. 4 –6
Some previous studies have shown the potential of real-time self-visualization of the video monitor by the patient as a distracting element that could diminish the perception of pain. However, the results have been conflicting, and most of these studies have had small samples, making it difficult to draw solid conclusions. 7 –11
Therefore, in this trial we intended to clarify the usefulness of real-time self-visualization of cystoscopy as an element to diminish the perception of pain.
Materials and Methods
All consecutive patients scheduled for an ambulatory cystoscopy (flexible cystoscopy in males and rigid cystoscopy in females) from August 1, 2017 to November 30, 2017 were included. This study was approved by our institutional review board, and all patients included gave their verbal consent to participate. Cystoscopies were performed by two urology residents (D.A.G.-P. and A.G.-D.), both with at least 300 procedures performed as previous experience.
The indications for cystoscopy were: hematuria approach, surveillance of NMIBC, lower urinary tract symptoms, and urinary incontinence. We excluded patients with clinical suspicion of bladder pain syndrome (suprapubic pain related to bladder filling, accompanied by other symptoms such as increased daytime and nighttime frequency, in the absence of proven urinary infection or other obvious pathology) 12 ; those who required additional procedures such as double J stent removal or urethral dilation; those with psychiatric disorders; and those for whom language limitations precluded full understanding of the trial.
All patients were placed in a lithotomy position. Male patients underwent flexible cystoscopy using a 15.5F fiber optic cystoscope (model 11272C; Storz®) and women underwent rigid cystoscopy with a 17F compact cystoscope (Storz®), previously lubricating the distal end of the scope with 10 mL of sterile lubricant with tetracaine in both cases. Immediately after completing the procedure and before leaving the room, patients were asked to register their pain perception using a printed Visual Analog Scale (VAS) from 0 to 10.
The patients were quasi-randomized into two groups in blocks by dates: group A from August 1, 2017 to September 30, 2017 and group B from October 1, 2017 to November 30, 2017.
Group A was not allowed to visualize cystoscopy, while Group B was allowed to self-visualize cystoscopy in real time on the video monitor. Both groups received the same detailed explanation from the nursing staff and urologist before and during the procedure.
The variables analyzed were gender, age, VAS score (as a continuous [0–10] measure), number of previous cystoscopies including the current one (1, 2, ≥3), indication for cystoscopy, and positivity of the test for bladder neoplasia. All patients were analyzed by group and gender separately. The statistical tests used were: Wilcoxon Rank-sum, Kruskal–Wallis, Mann–Whitney U test, Pearson correlation, and linear regression using SAS® software.
Results
A total of 404 patients (318 males and 86 females) were analyzed (group A with 239 and group B with 165), Table 1 summarizes the baseline characteristics of both groups.
Demographics and Characteristics of Male and Female Patients
p-Value calculated using Mann–Whitney U test for nonparametric test.
p-Value calculated by chi-squared test.
Among the 318 male patients analyzed, we found a mean VAS score of 2.6 for group A and 2.5 for group B without statistically significant differences (p = 0.276).
Among the 86 female patients analyzed, we found a mean VAS score of 2.78 and 1.64 for groups A and B, respectively, with a statistically significant difference (p = 0.008).
In contrast, the number of previous cystoscopies did have an influence on pain perception, with a mean VAS score for males of 3.12 for the first cystoscopy and 2.22 for the third or more cystoscopies (p = 0.02), and a mean VAS score of 2.97 for the first and 1.56 for the third or more cystoscopies in females (p = 0.001), both statistically significant. Table 2 summarizes these findings.
Comparison of Mean Visual Analog Scale Scores Between Group A and Group B for Both Males and Females
Statistically significant p values are bolded.
VAS = Visual Analog Scale.
When analyzing separately males and females in both groups, as well as those who underwent their first and third (or more) cystoscopy, the benefit of self-visualization diminished for the female group, remaining only in females with ≥3 cystoscopies, as shown in Table 3.
Comparison of Mean Visual Analog Scale Scores Between Group A (No Self-Visualization) and Group B (Self-Visualization) for Males and Females Separated by Number of Previous Cystoscopies (Including the Current One)
The remaining 37 patients had their second cystoscopy and were excluded from this analysis.
Statistically significant p values are bolded.
Figures 1 and 2 show boxplots representing VAS scores. The whiskers show the minimum and maximum reported values; the horizontal line inside the box represents the median; and the upper and lower edges of the box represent the upper and lower quartiles.
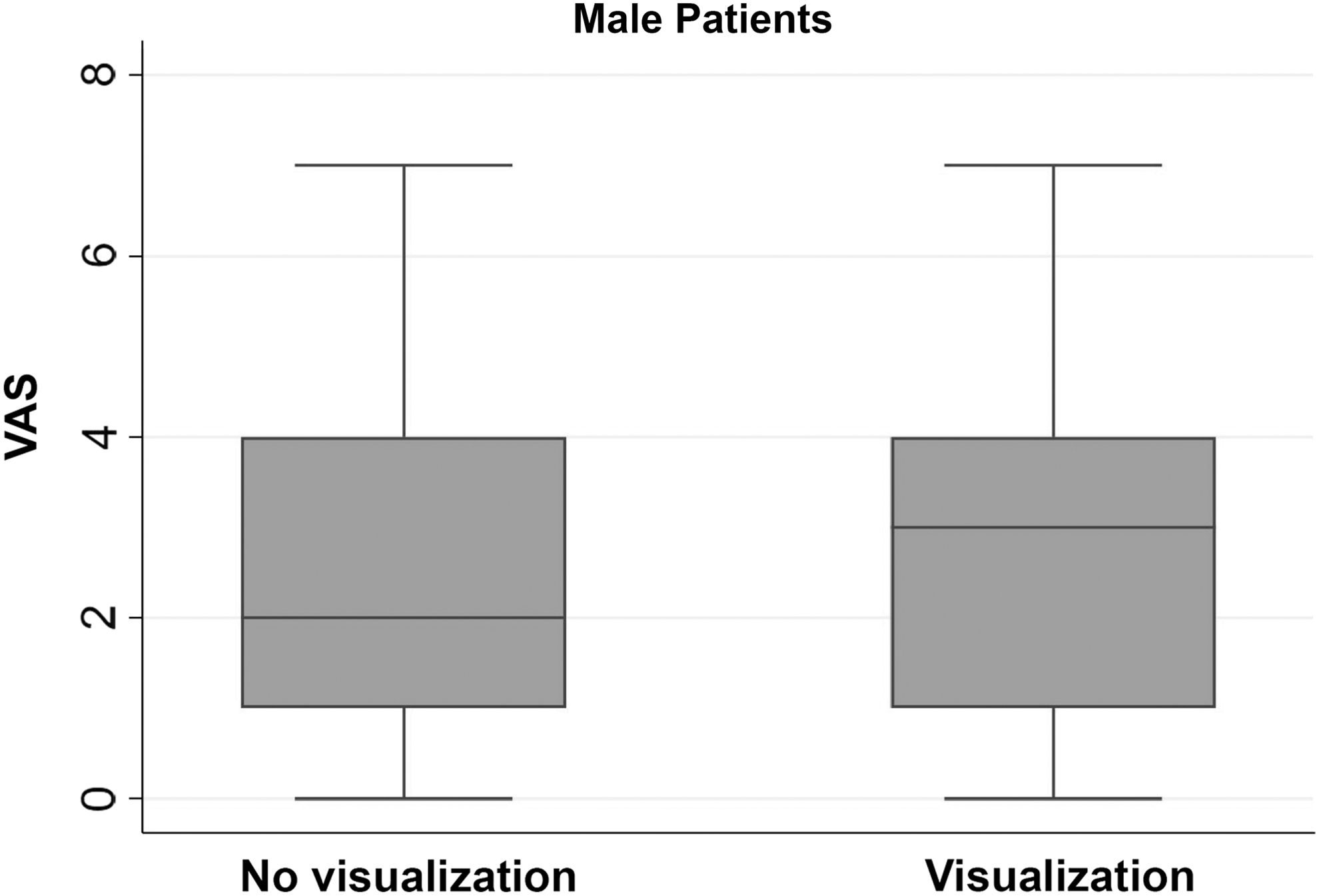
Boxplot representing VAS scores for male patients. Median score of 2 for group A (no visualization) and 3 for group B (visualization) with equivalent upper and lower quartiles (4 and 1, respectively). VAS = Visual Analog Scale.
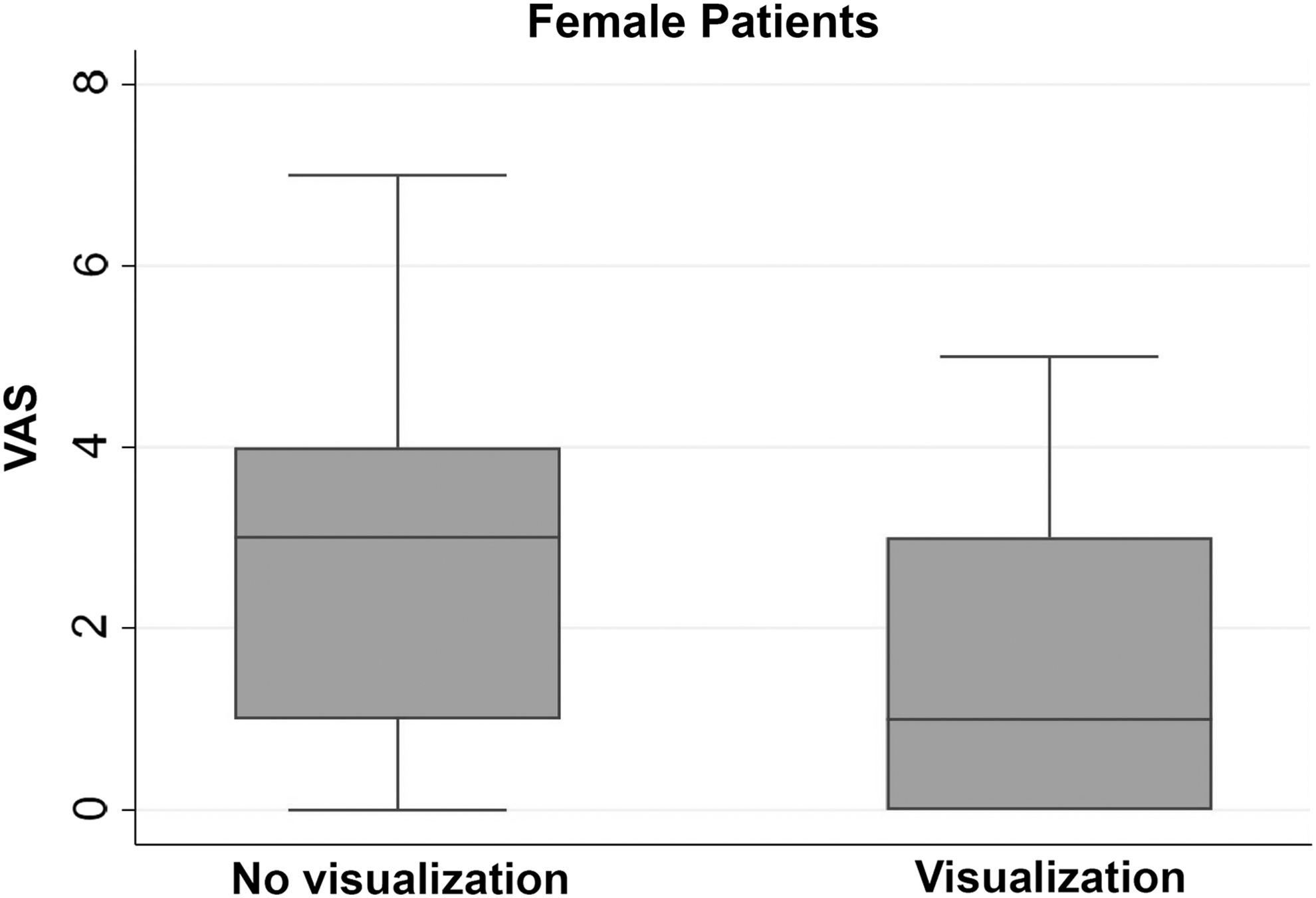
Boxplot representing VAS scores for female patients. Median score of 3 for group A (no visualization) and 1 for group B (visualization) with upper and lower quartiles for group B having lower values.
Regarding the other variables, no statistically significant differences were found regarding the positivity of the test for neoplasm (p = 0.14) or the indication for cystoscopy (p = 0.597).
Discussion
With this study, we sought to definitely determine the influence of real-time self-visualization of cystoscopy on the patient's pain perception measured by the VAS. Previously conducted studies had small samples and showed conflicting results.
The most studied intervention to reduce pain during cystoscopy has been the use of lubricating gel with or without local anesthetic. 13,14 Multiple studies have been published in the literature, although these articles show contradictory results. A study by Kobayashi and colleagues suggested that even the administration of intraurethral lubricant (with or without lidocaine) is as painful as the insertion of the cystoscope, making this prior step probably unnecessary. 15
In two consecutive years (2008 and 2009), two systematic reviews with meta-analyses were published by different authors, with similar inclusion criteria and reaching opposite conclusions. The study by Patel and coworkers 13 suggested that the benefit is exclusively due to the lubrication of the urethra, while the study by Aaronson and coworkers concluded that lidocaine does provide a benefit. 14
Regarding self-visualization of cystoscopy, there are a few studies that have evaluated the perception of pain and the influence of cystoscopy self-visualization, also with conflicting results in both male and female patients.
In 2007 Patel and colleagues published the first randomized trial with 100 males undergoing flexible cystoscopy in which the group that was allowed to watch the screen had a statistically significant difference toward lower pain perception. 9 Subsequently, in 2008 Cornel and coworkers conducted a randomized trial with 154 males, in which no benefit was seen with the visualization of the screen. 16 Also in 2008, Patel and colleagues published a similar study with 100 female patients undergoing rigid cystoscopy, concluding that there was no benefit from self-visualization. 17 In 2011 Zhang and coworkers published a study of a similar methodology with 86 men, which suggested that visualizing cystoscopy did decrease the perceived pain. 11 In the same year, Soomro and colleagues published their study with 76 men, also with positive results. 10 Finally, Koenig and coworkers published an observational study in 2015, where they concluded that visualizing cystoscopy is useful in men but not in women (although it should be noted that the patients chose whether or not to see the screen). 8 These studies are summarized in Table 4.
Previous Studies That Have Analyzed the Perception of Pain During Cystoscopies in Association with Self-Visualization of the Procedure
In our study, we also decided to analyze the positivity of the test for bladder neoplasia due to the possible psychological impact it could have on the patient and its impact on the perception of pain. However, in the 30 positive cystoscopies (18 in group A and 12 in group B) there was no relationship between positivity of the test and perception of pain with a mean VAS score of 2.78 for group A and 1.67 for group B (p = 0.587).
The main strengths of our study were that we had a large sample with more than twice the number of patients than any previously published trial; we analyzed men and women under the same circumstances in a pragmatic manner; all patients were questioned about their perception of pain immediately after the procedure using a printed VAS available in the same room; and all of them had the procedure explained in the same manner by the nursing staff and physician.
As for the weaknesses of our study, we had a limited sample of female patients (n = 86), which, despite being the second largest sample in studies of this kind, did not allow us, in our view, to draw solid conclusions.
It should be noted that cystoscopies performed by residents in training (compared with staff) did not influence the perception of pain in a study by Nguyen and colleagues with 506 patients, 18 so we do not consider this as a weakness in our trial.
Another theoretical weakness is quasi-randomization, which was chosen due to logistic reasons. However, we believe that the groups were balanced and all relevant characteristics were equilibrated, so that this did not affect the reliability of the results considering that this was an open trial and the outcome measured was pain perception.
Finally, our study showed a clear association between the number of previous cystoscopies and the perception of pain, with a decrease in VAS score when comparing patients undergoing their first cystoscopy vs patients with ≥2 previous cystoscopies, independently of group and gender. This might be explained due to increased procedure tolerance and decreased anxiety that has been previously correlated with pain perception during cystoscopy, 19 and this could probably explain previous positive trials with small samples where this variable was not taken into consideration
Conclusion
With this trial, we conclude that in male patients undergoing ambulatory flexible cystoscopy, the self-visualization of cystoscopy in real time through the video monitor did not provide a reduction in the perception of pain as measured by a VAS.
In contrast, self-visualization in females provided a benefit in the perception of pain during rigid cystoscopy; however, these benefits were only shown in females with ≥2 previous cystoscopies, yet our female sample had a limited size and the clinical relevance of such improvement could be debated.
Finally, the number of previous cystoscopies influenced the perception of pain in males and females, with a clear correlation between decreased pain perception and number of previous cystoscopies.
Footnotes
Acknowledgment
The authors would like to acknowledge i + 12 institute for help with statistical analysis.
Author Disclosure Statement
No competing financial interests exist.