
Abstract
Purpose:
To investigate renal pelvic pressures during percutaneous nephrolithotomy (PCNL) in the standard, mini, and ultramini PCNL systems.
Methods:
We studied an ultramini PCNL system (UMP, outer shaft diameter 13F), a mini PCNL system (MPCNL, shaft 18F, nephroscope 12F), and a standard PCNL system (SPCNL, shaft 27F, nephroscope 24F). Pressure profiles were first investigated in an open model setup, subsequently in a closed model, and finally in an ex vivo porcine kidney. Measurements were determined with the nephroscope in an advanced and pulled-back position for all models.
Results:
In the advanced position, maximum pressures of 41.61 ± 0.20 mmHg (UMP), 15.61 ± 0.15 mmHg (MPCNL), and 15.46 ± 0.14 mmHg (SPCNL) were measured in the closed model. In the pulled-back position, maximum pressures were 16.04 ± 0.22 mmHg (UMP), 17.02 ± 0.11 mmHg (MPCNL), and 20.50 ± 0.11 mmHg (SPCNL). In the ex vivo porcine kidney model, maximum pressures were 13.81 ± 6.04 mmHg (UMP), 5.64 ± 0.21 (MPCNL), and 9.21 ± 0.52 (SPCNL) with the nephroscope pushed to end position. After retracting the nephroscope from the outer shaft, pressures in all systems did not exceed 10 mmHg.
Conclusions:
The maximum pressures achieved with the three PCNL systems in all three models were kept below the 30 mmHg critical threshold value. High pressures were only determined for the UMP system with the nephroscope pushed to its end position. This was attributed to the conical shape of the nephroscope, which occupies the space between the nephroscope and outer shaft, resulting in outflow obstruction.
Introduction
Percutaneous nephrolithotomy (PCNL) is the standard of care for large kidney stones. 1,2 Infectious complications (fever, pyelonephritis, systemic inflammatory response syndrome [SIRS], and sepsis) 3,4 may result in and may potentially demand prolonged hospital stay and intensive care unit support. 5
It is thought that infectious complications after PCNL result from systemic absorption of bacteria and endotoxins from the irrigation fluid. Renal pelvic pressures (RPP) of 30 mmHg or greater promote pyelovenous backflow into the collecting system and systemic venous circulation with the potential spread of infection. 6 –8 Zhong and colleagues found a positive correlation between RPP persistently ≥30 mmHg and postoperative fever. 9 In recent studies, high-pressure irrigation during PCNL has also been associated with an increased risk of postoperative SIRS. 10,11 There are limited data on PCNL calibers' influence on RPP. 12,13
We hypothesized that tract size might influence RPP. We therefore measured irrigation-related three-dimensional pressure profiles at the catheters' tips and static pressures with different sized PCNL systems. The measurements were conducted in three different models: an open system, a closed system, and an ex vivo kidney model simulating an in vivo renal pelvis. Possible results might have an impact on clinical decision-making.
Materials and Methods
Open physical model—dynamic pressure profiles
Three-dimensional pressure profiles were determined for three PCNL systems: ultramini PCNL (UMP, outer shaft diameter 13F, inner shaft diameter 12.52F, nephroscope 7.5F), mini PCNL (MPCNL, outer shaft 18F, inner shaft diameter 15.3F, nephroscope 12F), and standard PCNL (SPCNL, outer shaft 27F, inner shaft diameter 24.3F, nephroscope 24F). The configurations were adopted with the nephroscope inside the access sheath in advanced and pulled-back positions. For UMP, two different irrigation channels were tested: the standard irrigation channel within the nephroscope and the special flushing channel within the access sheath, only used for flushing out stone fragments and dust. An irrigation pump (LUT, Denzlingen, Germany) provided a continuous flow of 100 mL/minute for all experiments.
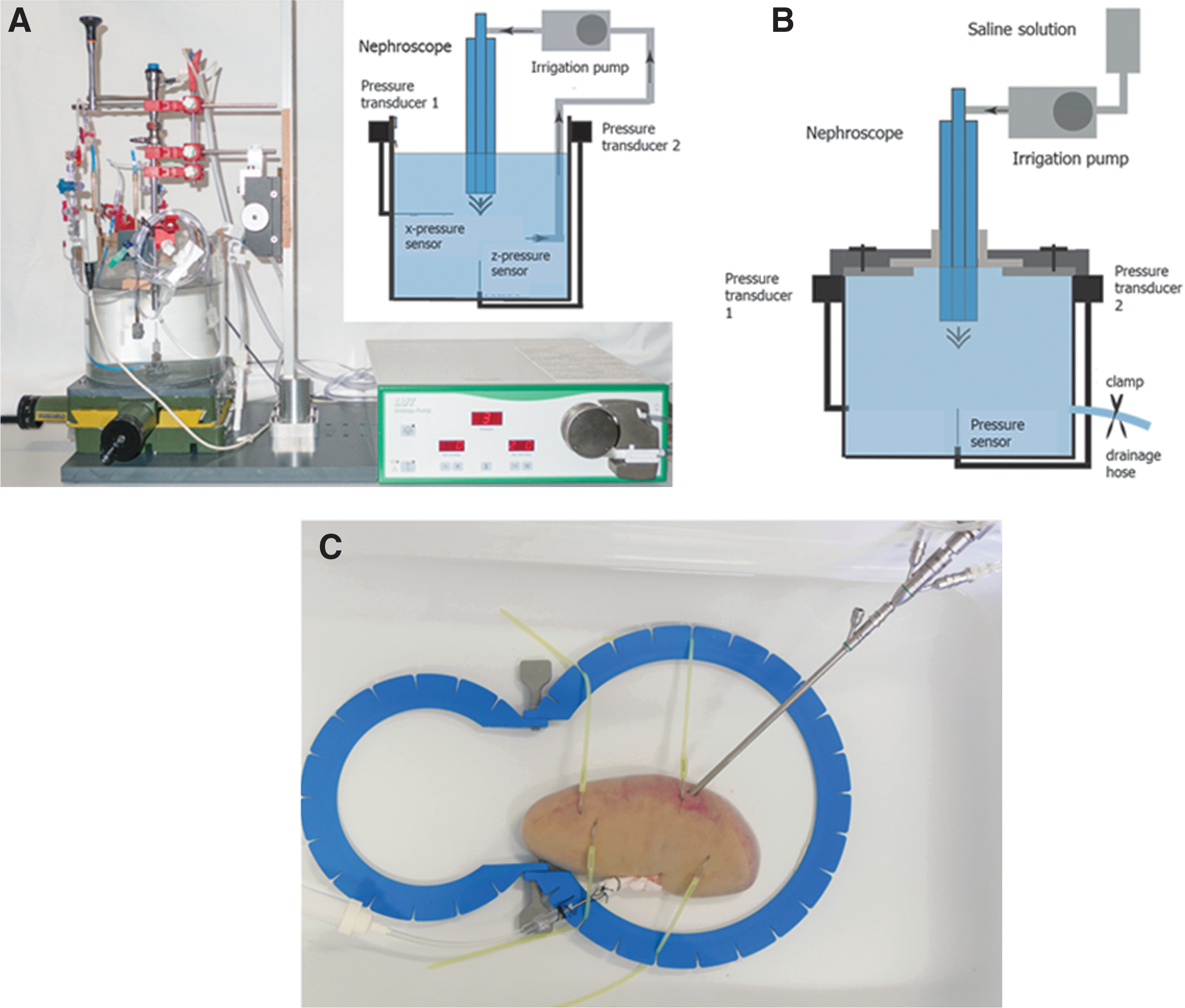
A cylindrical, open-topped Plexiglas tube with an inner diameter 19.5 cm and height 20 cm was filled with 4.4 L of physiologic sodium chloride solution. At the center of the vessel base, a 30-mm-long z-pressure probe was positioned to measure the vertical component of the flux generated pressure. The z-probe reached 7.5 cm in height. Two 57-mm-long x- and y-pressure probes were mounted at the vessel wall at 7.5 cm height to measure the horizontal components of the flux generated pressure. All pressure probes were perpendicular to each other. A 7.5-cm-high column of liquid was maintained above the tip of all three pressure probes. All corresponding pressure transducers were fixed at the same height of 19.5 cm at the top of the vessel to avoid potential hydrostatic artifacts. The respectively tested nephroscope was positioned perpendicular to the liquid level from the top of the vessel (Fig. 1A).
Experimental models.
To characterize the pressure distribution around the nephroscope, pressure profiles were measured in horizontal planes at 5 mm intervals. Within each horizontal plane, pressure values were acquired for a 4 mm × 4 mm range divided into a grid with 0.5 mm distance between the measurement points. Each measurement was repeated three times. For convenient visualization, data were smoothed with a three-dimensional cubic spline interpolation, generating a grid with virtual resolution of 0.05 mm in both horizontal directions and 0.5 mm in the vertical direction. In preparation for the subsequent models, the localization of maximum pressure points was of particular interest. We aimed to clarify whether the maximum pressure should be measured centrally, laterally, or behind the tip of the nephroscope.
Closed model—maximum pressures
A cylindrical, completely sealable vessel made of PVC with 12 cm inner diameter, 6.4 cm inner height, and a capacity of 720 mL was used to simulate conditions of a closed system. The vessel was filled with physiologic sodium chloride solution. In the center of the vessel bottom, we fixed the z-pressure probe, whose tip reached 3.6 cm in height. During the measurements, the access sheath was mechanically fixed and the test vessel was pneumatically sealed. Excess liquid could therefore only flow out via the nephroscopy system itself. To simulate the ureter, a 30.5 cm silicone hose with 2 mm inner diameter was attached to the vessel wall at 3.5 cm height and clamped. A slight drainage was possible via this tube (Fig. 1B).
The center of the respective access sheath was defined as the central zero position. A coarse grid was created with a 10 mm gap between the individual measuring points to determine the global pressure prevailing in the test vessel. In addition, a fine grid in the direct flow field of the flushing channel with a distance of 0.5 mm between the individual measuring points was measured. Overall, five planes with a distance of 0.5 cm were measured.
Ex vivo model of porcine kidneys
In an ex vivo model, the maximum RPP were measured for each nephroscopy system, taking into account kidney compliance. Two fresh, nonperfused pig kidneys with intact renal pelvis and ureter were used. The ureter was shortened to the appropriate length for the 57-mm-long pressure probe. The lower calix groups of the kidneys were punctured under ultrasound guidance with a 17.5G needle (Angiomed, C.R. Bard GmbH, KA, Germany) and a guidewire was advanced into the renal pelvis. The dilatation up to 13F for the UMP, 18F for the MPCNL, and 27F for the SPCNL was carried out using sequential plastic bougies (Amplatz Renal Dilator Set, Cook Medical, IN) and the access sheath and obturator placed over the guidewire.
The nephroscope and pressure probe positions were monitored via an endocamera (Karl Storz, TUT, Germany), connected to the nephroscope. The pressure probe was attached to the prepared ureter, fixed with a surgical suture (2/0, SERAG-WIESSNER, Naila, Germany), and sealed against the lumen of the ureter. The kidneys were fixed with surgiloops to lie flat in a large basin and covered with physiologic sodium chloride solution (Fig. 1C).
A constant irrigation flow of 100 mL/minute via the respective PCNL system was applied, and intrarenal pressure was measured while aiming with the nephroscope on the tip of the pressure probe to ensure measurement at the maximum pressure point. After completion of all measurements, the water tightness of the renal pelvis was checked again to exclude a potential renal pelvic rupture with alteration of our results.
Statistical analysis
The data were analyzed with the statistical software GraphPad PRISM 6.0c (GraphPad Software, Inc., La Jolla, CA). Data are presented as mean ± standard deviation. Pressure differences ≥5 mmHg were determined clinically relevant. Continuous variables for different PCNL systems were tested with ANOVA. Statistically significant group differences were considered if p < 0.05.
Results
Open model—pressure profile
For all PCNL systems, three-dimensional characteristic pressure profiles of the dynamic flux pressure could be identified (Fig. 2A, B).

Exemplary spatial pressure profiles of a UMP system.
Pressures were highest at the nephroscope tips and decreased with increasing distance. No relevant pressure elevations were observed in more than 3 cm distance from the tip of the endoscope. No pressure differences were measured behind the flushing channel (Fig. 2C).
Closed model
With the nephroscope advanced maximally inside the access sheath, the UMP presented maximum pressures above 40 mmHg (Fig. 3A). With both irrigation methods, through the nephroscope and through the accessory flushing channel inside the shaft, the UMP generated pressures more than twice as high than the MPCNL and SPCNL. There was no statistically significant difference between the maximum pressure values for the MPCNL or SPCNL setup (p = 0.6173).

Pressures at different distances from the nephroscope tip.
With a pulled-back distance of 0.5 cm, significantly higher pressures were found for UMP compared with the other two setups during irrigation via the access sheath and at distances between 0 and 1 cm (Fig. 3B).
On the wall of the test vessel, significantly higher pressures were found in the advanced position for the UMP with both irrigation methods, compared with MPCNL and SPCNL (Fig. 4A). The highest pressure was recorded when the UMP was flushed via the nephroscope, the lowest pressure in the MPCNL (48.5 mmHg vs 15.5 mmHg).
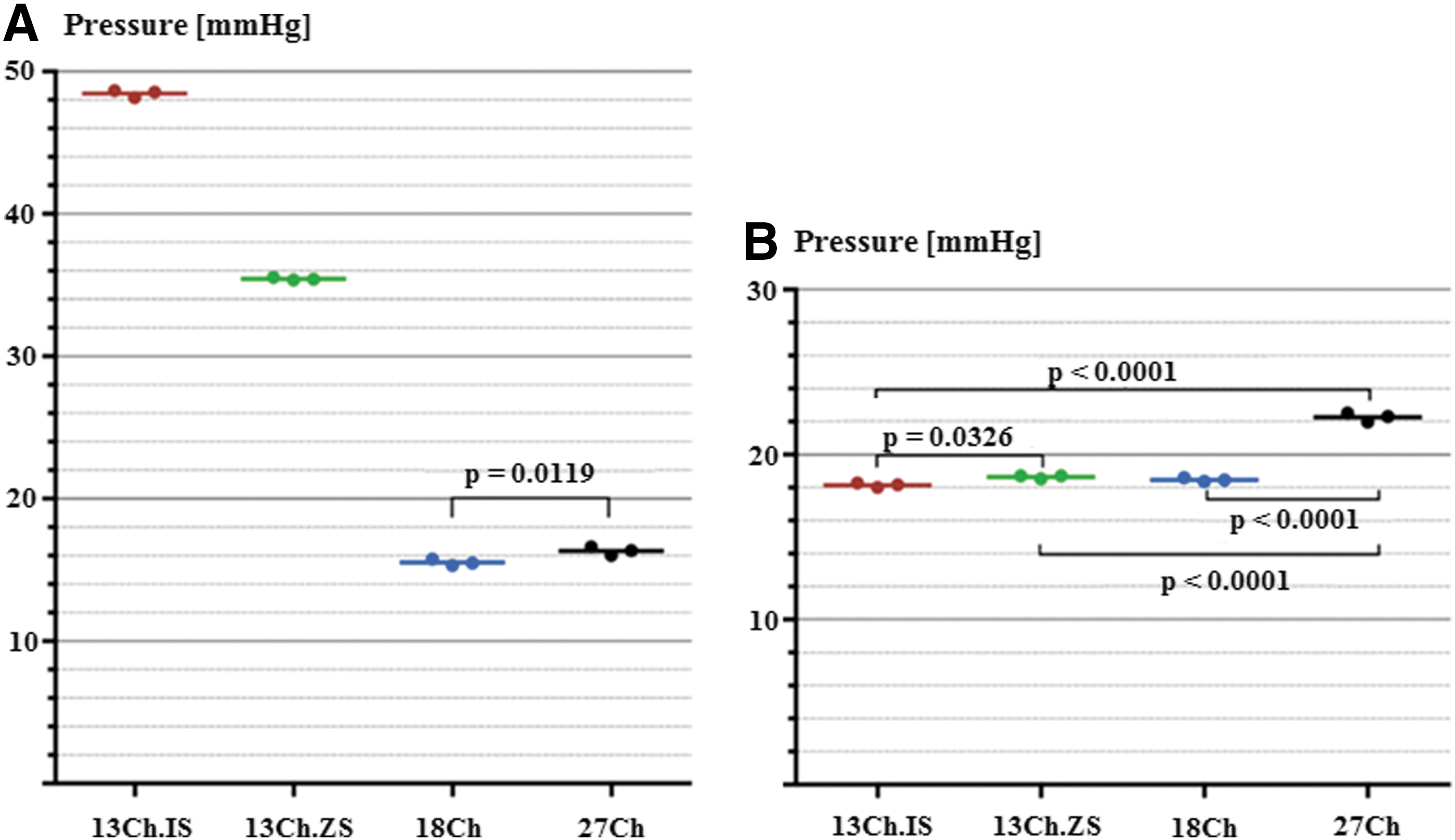
Pressure on the vessel wall.
The wall pressure obtained in the pulled-back position dropped below 20 mmHg in the UMP independent of irrigation (Fig. 4B). This value was comparable with the maximum wall pressure of the MPCNL (18.47 mmHg).
Position of the nephroscope in the access sheath
UMP with irrigation through the nephroscope showed a pressure difference of 25.8 ± 0.46 mmHg (p < 0.0001) between the advanced and the 1 cm pulled-back position. The maximum pressures in the two retracted positions (0.5 and 1 cm) did not differ from each other (p = 0.9888).
For MPCNL, we found a maximum pressure of 15.6 mmHg in the advanced position and 17.0 mmHg (p = 0.0002) in the pulled-back position. For SPCNL, the mean maximum pressure in the retracted position was 5.0 mmHg higher than in the advanced position (15.5 mmHg vs 20.5 mmHg).
Ex vivo kidney model
Diameter of PCNL systems
All recorded pressures were below 20 mmHg. With the nephroscope in the advanced position, significantly higher mean pressures were found for UMP compared with MPCNL and SPCNL. The highest pressures were generated with the UMP flushed through the nephroscope. The pressures generated with the UMP were on average 7.9 mmHg higher than with MPCNL, which had the lowest mean pressure (5.1 mmHg, p = 0.0024). The mean pressure for the SPCNL did not differ significantly from that of the MPCNL (Δpressure = 3.6 mmHg, p = 0.2317) nor from that of the UMP for both irrigation methods (internal channel: Δpressure = 4.3 mmHg; p = 0.1197; access sheath: Δpressure = 2.6 mmHg; p = 0.4826) (Fig. 5A).
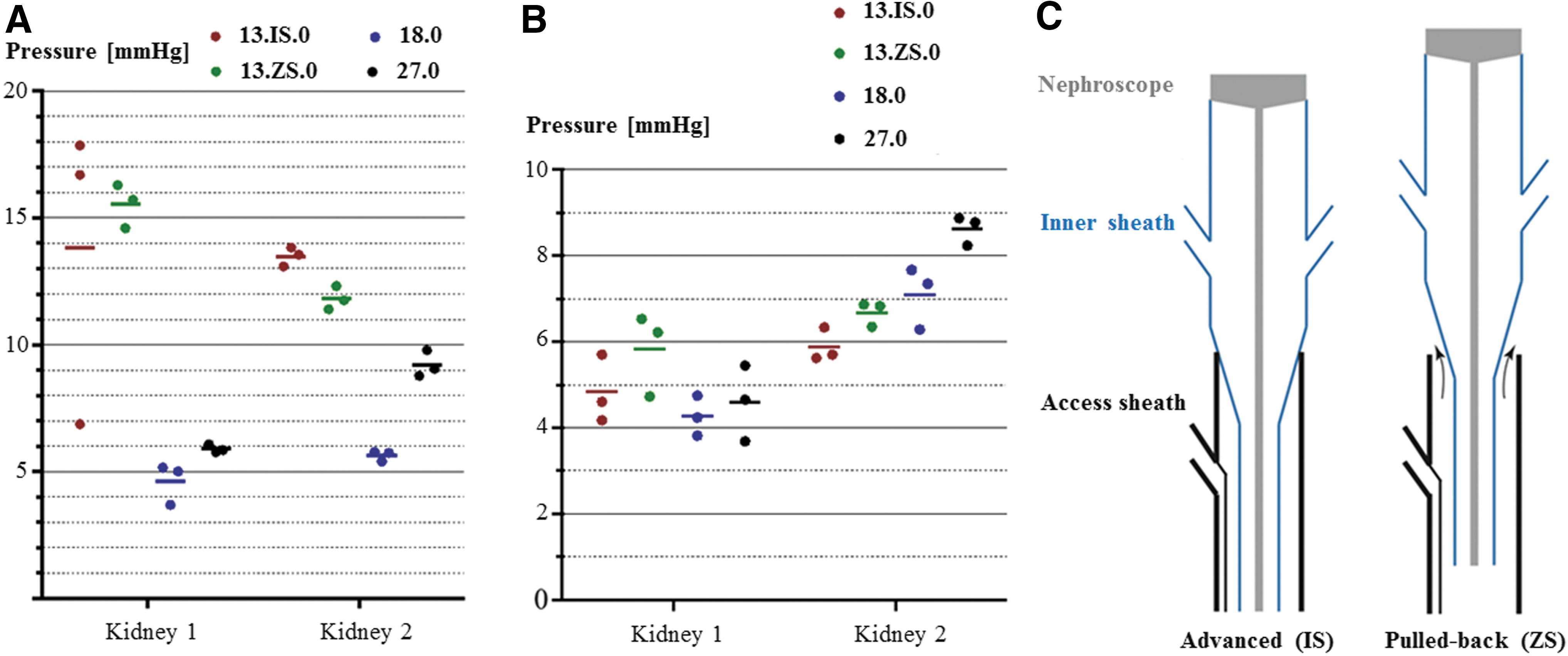
Wall pressures in the porcine model.
Position of the nephroscope in the access sheath
In both kidneys, UMP pressure values were higher in the advanced position than in the pulled-back position with both irrigation methods. When flushed via the nephroscope, the mean difference between the two positions in the first kidney was 9.0 mmHg (p = 0.0024). When flushed over the access sheath, this difference increased to 10.5 mmHg (p < 0.0001). The pressures in the two pulled-back positions did not differ significantly from each other (Fig. 5B).
MPCNL pressures did not differ in the advanced and retracted positions in the first kidney. In the second kidney, a 1.5 mmHg higher mean pressure was observed in the retracted position.
The SPCNL generated significantly higher pressures in the advanced than in the pulled-back position (Δpressure = 1.3 mmHg, p = 0.89) in the first kidney, but no difference was observed in the second kidney.
Discussion
Recent modifications in PCNL instrumentation and technique call for a critical evaluation in efficacy and also in safety and adverse effects. Studies on renal physiology have shown pathologic changes in renal tubule histology if intrarenal pressures exceed 30 mmHg. 14 Systemic absorption of irrigant, debris, and bacteria can enter the blood stream through pyelovenous lymphatic or renotubular backflow and elicit a systemic inflammatory response. Although high RPP have been linked to postoperative fever and perioperative sepsis, scarce data have been published regarding RPP measurements in experimental PCNL systems so far. 11
This study focused on the flow-related pressure conditions in the different PCNL systems, UMP (13F), MPCNL (18F), and SPCNL (27F), by using self-constructed physical models and an ex vivo porcine kidney model. The main finding of our study is that all tested PCNL systems generated maximal pressures below the critical threshold value of 30 mmHg. However, high pressures were caused by the UMP system if the nephroscope was pushed to the end position inside the access sheath. A reasonable explanation is that the conical shape of the nephroscope can close the space between the nephroscope and outer shaft almost completely, which leads to outflow obstruction.
Overall, no uniform correlation was observed between the diameter of the access sheath of a PCNL system and the irrigation-induced RPP.
Loftus and colleagues studied the effect of sheath and endoscope size on RPP in a porcine model and associated MPCNL with higher RPP and higher risk of end-organ bacterial seeding than with SPCNL. 15 Zhong and coworkers found that prolonged RPP of 30 mmHg or greater were significantly associated with postoperative fever after MPCNL. 9 The authors concluded that any factor that results in poor drainage during PCNL contributes to elevated RPP. 4,9 In MPCNL, there is less space between the access sheath and the endoscope for irrigant to escape, resulting in higher system pressures than with SPCNL. 1
Alsmadi and colleagues measured RPP in 74 patients using super-MPCNL (14F) and found average RPP of 19.5 mmHg when irrigation flow was kept below 320 mL/minute. Their results are comparable with those observed in the present study in all PCNL systems and confirm that RPP are intricately related to irrigation flow, compliance, and drainage. 12
For the UMP system, we found that drainage capacity depends on the position of the nephroscope within the access sheath. If the nephroscope is pulled back, the observed pressures were below the critical threshold of 30 mmHg, while in the advanced position we observed higher pressures. A possible explanation for this is the conical shape of the nephroscope, obstructing irrigant outflow in the advanced position (Fig. 5C). It is unclear how frequent this completely advanced position occurs during PCNL in the clinical setting.
There are numerous conditions in which high RPP can occur as a result of endoscope positioning, such as scavenging a stone from the margin of a calix or torquing a rigid endoscope against the pyelocaliceal system to reach an inaccessible calix. 9,13 In our study, we observed positional high irrigation pressures only for UMP when flushed through the additional irrigation channel in the access sheath. This flushing model is only used during a limited time to flush out small stone particles and sand.
Although high pressures may have deleterious effects on surgical outcomes, a certain amount of RPP is required to gently expand the collecting system for sufficient visualization of caliceal infundibula and stones. 16,17 Future studies are therefore necessary to identify the ideal pressure parameters that allow optimal visualization while maintaining low RPP.
The study is limited by its experimental nature. The vessel in the open model had a large diameter of 19.5 cm and a rigid wall, differing from the conditions in the clinical situation. However, this was accepted: the size of the vessel was required to exclude potential interactions of the fluid stream with vessel wall. The open vessel top allowed precise measurements on fine grid points (0.5 mm pitch), which were essential for detailed representation of the three-dimensional pressure profiles. This experiment served to identify the flux-related pressure profiles at the nephroscope tips. Notably, the described pressure values present only the dynamic part of the total pressure, which may add to a potentially present static pressure, not captured in this part of our study.
In the closed model, we tried to simulate the conditions in the renal pelvis as a pneumatically sealed hollow organ. To simulate a ureter with an occlusion catheter, a clamped silicone tube was used. 18 It cannot be ruled out whether there was any residual drainage around the catheter. Accordingly, the high pressures reached under the restricted drainage conditions may not be fully representative of those reached in the clinical application, especially of the small-sized UMP system.
Other clinical parameters, such as shape and compactness of the collecting system, stone burden and its complexity, and extent of bleeding (apart from the flow dynamics), may also affect the RPP and cannot be accounted for by this experimental design.
Conclusion
Static and dynamic pressures generated by standard, mini, and ultramini PCNL systems are generally below the critical threshold value of 30 mmHg. However, higher pressures may occur with the UMP system if the nephroscope is pushed to the end position inside the access sheath, thereby obstructing the outflow. This finding should be taken into consideration in the daily clinical work when using UMP systems. More studies, especially comprising the clinical situation, are required to determine the impact of endoscope position and caliber in RPP during PCNL.
Footnotes
Acknowledgment
We thank Mr. Matthias Schneider for his continuous support with the construction of the experimental models.
Authors' Contribution
K.W.: project development, experiments, supervision, and article writing; P.F.M.: article and figure writing/editing and data analysis; J.S.-A.: performing experiments and data analysis; J.S.: project development; R.S.-I.: figures and article writing; A.M.: supervision; S.S.: project development, supervision of experiments, data analysis, and article writing.
Author Disclosure Statement
The MPCNL and SPCNL systems were provided by Richard Wolf GmbH (Knittlingen, Germany). The UMP system was provided by LUT (Denzlingen, Germany). However, there was no influence of the two companies on the experiments, results, or interpretation of the data.