
Abstract
Introduction:
The objectives of this study were to introduce a newly developed approach for holmium laser enucleation of the prostate (HoLEP) called the “complete en-bloc technique,” and to compare the clinical outcomes of this approach with those of previously performed procedures.
Methods:
This study retrospectively assessed the perioperative findings from 548 patients with benign prostatic hyperplasia (BPH) undergoing HoLEP who were divided into the following groups according to the consecutive changes in surgical techniques: group A (n = 236), the three-lobe technique; group B (n = 137), the conventional en-bloc technique; and group C (n = 175), the complete en-bloc technique with direct bladder neck incision.
Results:
There were no significant differences in major clinical characteristics or urinary symptoms among groups A, B, and C. Although there was no significant difference in the resected prostate weight among the three groups, the enucleation time was significantly shorter and total laser energy was significantly lower in group C than in groups A and B. Therefore, the enucleation efficiency, calculated by dividing the resected prostate weight by the enucleation time, was significantly greater in group C than in groups A and B. Furthermore, no significant differences in the postoperative urinary symptoms, including the International Prostate Symptom Score (IPSS), quality of life, maximum flow rate, postvoid residual, and persistent stress urinary incontinence rate, were noted among the three groups, and there were no significant differences in the incidences of major perioperative complications, including the blood transfusion, bladder injury, urethral stricture, and bladder neck sclerosis among the three groups.
Conclusions:
These findings suggest that our complete en-bloc technique can improve the clinical outcomes of HoLEP in BPH patients, even in difficult cases, considering its markedly improved enucleation efficiency.
Introduction
Minimum invasive surgeries using several types of lasers, including holmium laser, potassium titanyl phosphate laser and thulium laser, have been increasingly applied to treatm benign prostatic hyperplasia (BPH). 1 –3 Of these, holmium laser enucleation of the prostate (HoLEP), originally reported by Gilling et al. in 1998, 4 has become one of the potential alternative therapies to the classic transurethral resection of the prostate and open prostatectomy for patients with BPH. 5 –10 To date, a number of single-center and multicenter studies have demonstrated that HoLEP could be a more efficient and safe procedure than other surgical treatments, irrespective of prostate size. 11 –16 However, even with its marked advantages, HoLEP has not widely spread because of several reasons, including the difficulty to learn and teach its procedure. 17 –19 Accordingly, several alterations in the surgical technique associated with HoLEP have been introduced to minimize the learning curve. For example, anteroposterior dissection HoLEP optimized the visibility of separation between the adenoma and surgical capsule, and safely enabled preservation of the sphincter, significantly improving the morbidity and learning curve of HoLEP. 14 More recently, instead of the conventional technique of dividing the adenomas into some lobes, 4,20 –25 the en-bloc enucleation technique was developed to further improve the perioperative outcomes of HoLEP. 26,27
At our institution, HoLEP was first performed in 2011 using the three-lobe technique as previously reported by Endo and colleagues. 20 As we gained experience, we gradually shifted to the conventional en-bloc enucleation technique with modification of the original procedures. However, as these approaches required incision of the adenoma for enucleation, this approach often induced hemorrhage and disorientation, resulting in a prolonged operative time. As such, to make the HoLEP procedure less challenging, we developed a new approach for HoLEP called the “complete en-bloc technique with direct bladder neck incision,” which enables enucleation of the adenoma without an incision. In this report, we describe the detailed surgical procedure of the complete en-bloc technique and retrospectively compared the clinical outcomes of this novel technique with those of our previous procedures.
Patients and Methods
Patients
The research ethics committee of our institution approved the design of this study, and the need to obtain informed consent for involvement in this study from all of the included patients was waived because of its retrospective design. At our institution, 667 consecutive patients with BPH underwent HoLEP between September 2011 and December 2016. After excluding 119 in whom a complete data set was not available, a total of 548 were included in this study. In this series, HoLEP was performed by five surgeons with previous experience of >30 HoLEP procedures before the involvement as an operator at our institution. The 548 patients were classified into the following three groups according to the enucleation techniques: group A, the three-lobe technique reported by Endo et al. 20 ; group B, the conventional en-bloc enucleation technique with adenoma incision 26,27 ; and group C, the newly developed complete en-bloc technique with direct bladder neck incision described in detail hereunder. As a rule, each technique was consecutively introduced and performed during the following period: three-lobe technique, between September 2011 and October 2013; conventional en-bloc enucleation technique, between October 2013 and July 2014; and complete en-bloc technique, between July 2014 and December 2016.
Equipment
A continuous flow 26F resectoscope (Karl Storz, Tuttlingen, Germany) equipped with a dedicated laser fiber stabilizing bridge, a 550-μm laser (SlimLine™ 550), a 12° optics, and an endoscopic camera were employed. The 75-W holmium laser (VersaPulse® Select™ 80 W; Lumenis, Yokneam, Israel) was used in all cases (2.5 J/30 Hz setting). Transurethral morcellation was performed using a 26F rigid Storz nephroscope and the Versacut Morcellator System (Lumenis). After enucleation, the Storz bipolar electrode was used for hemostasis of the surgical capsule.
Parameters
We evaluated the weight of the resected prostate specimens, enucleation time, and total laser energy required during the enucleation, and the enucleation efficiency was calculated by dividing the resected prostate weight by the enucleation time. In addition, International Prostate Symptom Score (IPSS), quality of life (QoL), maximum flow rate (Qmax), postvoid residual (PVR), and persistent stress urinary incontinence (SUI) rate were used to assess the urinary symptoms as early postoperative outcomes for each patient. In this series, indwelling urinary catheter was generally removed 2 days after surgery, and the achievement of urinary continence was defined as the use of no pad at 3 months after surgery.
Surgical procedure for the complete en-bloc technique
Supplementary Video S1 demonstrates the complete en-bloc technique described below.
The mucosa is incised from the side of the verumontanum to expose the surgical capsule. In this procedure, it is particularly important to find the exact plane first. Once the initial plane is identified under the right lobe, the operator turns the endoscope by 180° and frees the right lobe from the surgical capsule (Figs. 1A and 2A, B).
The space between the adenoma and the surgical capsule is retrogradely separated toward the bladder neck with intermittent incision of the distal sphincter muscle to prevent excessive tension on the sphincter. The bladder lumen is then exposed by incising the anterior fibromuscular stroma at 10 o'clock position (Figs. 1B, and 2C–E). After reaching the bladder lumen, it becomes possible to improve perfusion efficiency and view the lumen of the bladder.
After reaching the bladder lumen, the bladder neck is dissected annularly, and passive detachment using the shaft of the resectoscope is performed antegradely toward the bottom of the lateral and middle lobes (Figs. 1C, and 2F, G). Furthermore, by lifting the right lobe with the resectoscope shaft, continuous peeling to the middle lobe is possible without separation from the right lobe (Fig. 2H).
By pulling down the entire adenoma on the shaft of the resectoscope, a sharp incision is made in the anterior fibromuscular stroma at the bladder neck to mobilize the adenoma. As with the right lobe, the annular incision of the bladder neck and passive detachment of the left lobe are subsequently performed antegradely (Figs. 1D, and 2I, J).
When the adenomas are almost completely peeled, a mucosal band of the sphincter is naturally formed at the apical urethra (Figs. 1E, and 2K, L). When incising the mucosa, it is important to maintain a tension-free state by pulling the endoscope distally. At this point, the completely enucleated adenoma can be pushed inside the bladder lumen (Figs. 1F, and 2M–O).
The intact ring where the sphincter forms is clearly observed after the entire adenoma is removed. We occasionally use the bipolar electrode for hemostasis of surgical capsules after enucleation, particularly for patients with hemorrhagic diathesis, such as those under antiplatelet or anticoagulation therapy. The enucleated adenoma is then removed from the bladder lumen using a morcellator.
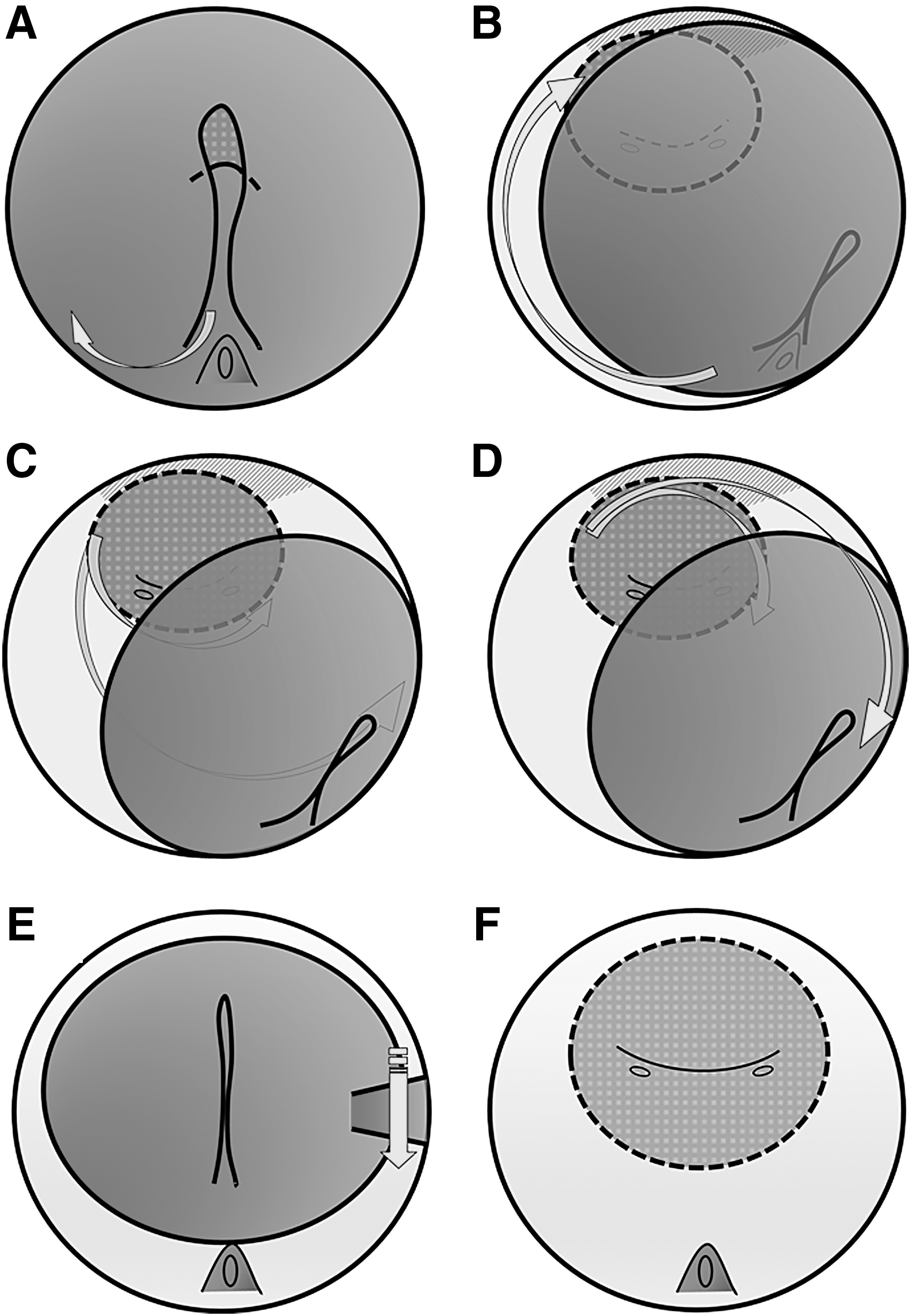
Schematic presentation of the complete en-bloc technique for HoLEP.
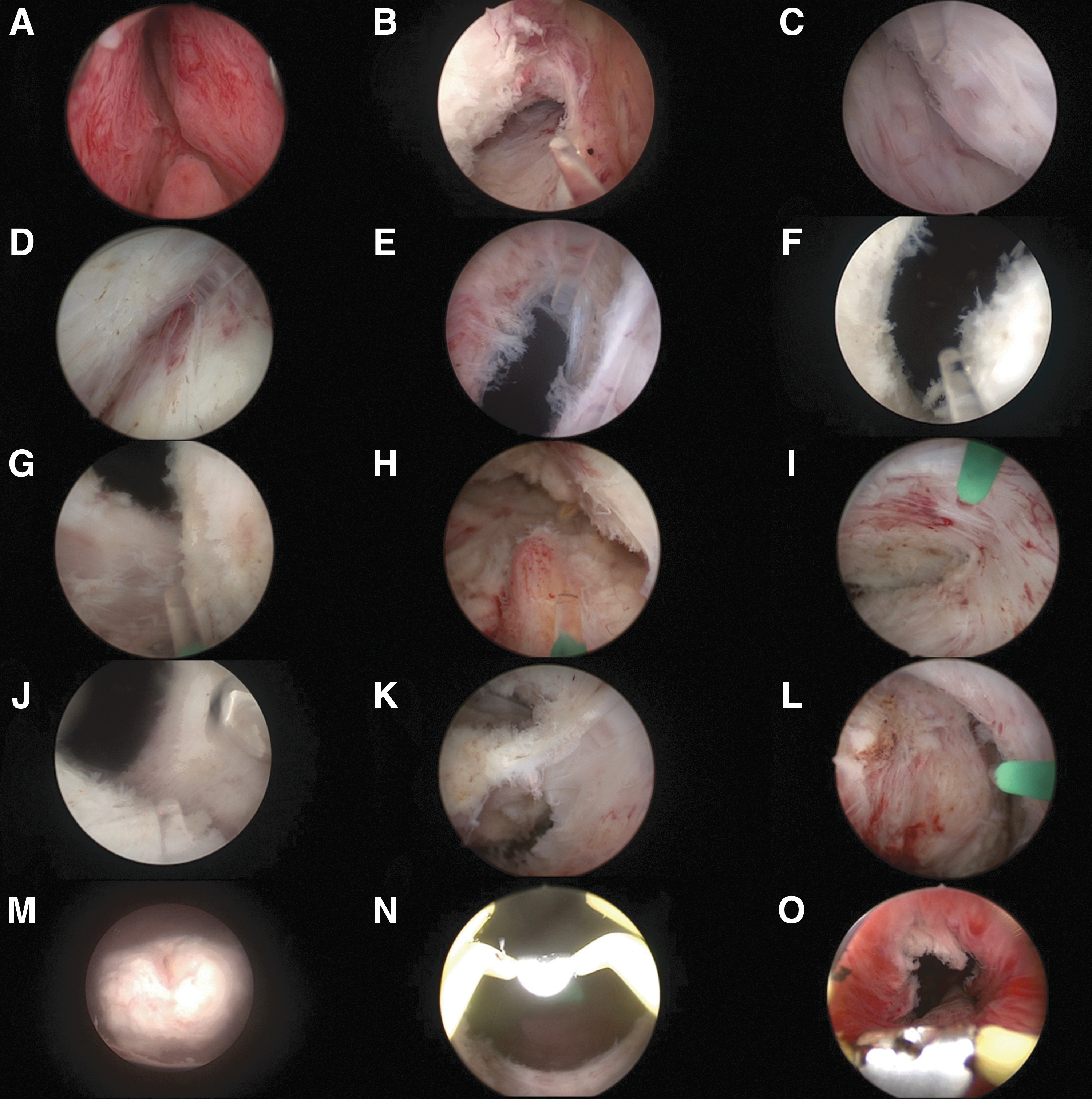
Endoscopic view of the complete en-bloc technique shown in Figure 1.
Statistical analysis
All statistical analyses were carried out using MedCalc® (version 13.0.2.0), and p-values <0.05 were considered significant. Differences in several parameters among the three groups were compared using ANOVA for continuous variables, and all statistical tests were two sided.
Results
The characteristics of the included patients according to the surgical techniques for enucleation are given in Table 1. There were no significant differences in the major clinical parameters, including age, total prostate volume, prostate-specific antigen level, IPSS, QoL, Qmax, and PVR, among the three groups.
Baseline Characteristics of the Patients (n = 548) Who Underwent Holmium Laser Enucleation of the Prostate
Data are expressed as the mean ± standard deviation.
HoLEP = holmium laser enucleation of the prostate; IPSS = International Prostate Symptom Score; PSA = prostate-specific antigen; PVR = postvoid residual; QoL = quality of life; Qmax = maximum flow rate; TPV = total prostate volume.
Comparison of the perioperative outcomes among the three groups is given in Table 2. Although no significant difference in the weight of the resected prostate was noted among the three groups, the enucleation time was significantly shorter and the total laser energy was significantly lower in group C than in groups A and B. Therefore, the enucleation efficiency in group C was significantly superior to those in groups A and B. Three months after surgery, there were no significant differences in the urinary symptoms, including the IPSS, QoL, Qmax, PVR, and persistent SUI rate, among the three groups. Furthermore, no significant difference in the frequency of major perioperative complications, including blood transfusion, bladder injury, urethral stricture, and bladder neck sclerosis, was noted among the three groups. As for postoperative urethral stricture occurring in eight patients, its anatomical distribution was as follows: the bulbar urethra in seven patients and the anterior urethra in one patient.
Perioperative Surgical Parameters and Early Follow-Up Data: 3 Months After Surgery
Data are expressed as the mean ± standard deviation.
SUI = stress urinary incontinence.
Discussion
Since its initial description by Gilling and colleagues, 4 HoLEP is currently regarded as a suitable surgical technique for patients with BPH because of several confirmed advantages such as minimal invasiveness, low morbidity, and long-term durability. 5 –16 Furthermore, several studies have reported the utility of modified surgical approaches for HoLEP, including en-bloc techniques 20 –25 ; however, all approaches require one or more incisions in the adenoma to complete the enucleation. Since BPH is a multinodular tissue originating from the transition zone and periurethral glands, 28 it is sometimes difficult to exactly identify the anatomical boundary between the lateral and middle lobes; thus, an active incision to separate the adenoma is necessary, which usually results in unnecessary blood loss and loss of anatomical orientation during surgery. Considering these factors, we devised a new technique called the “complete en-bloc technique with direct bladder neck incision,” which enables enucleation of the adenoma without any incision.
In this study, we comparatively assessed the clinical outcomes of three different surgical approaches for HoLEP consequently introduced at our institution: the three-lobe technique, 20 conventional en-bloc technique with adenoma incision, 26,27 and the newly developed complete en-bloc technique. Initially, the absence of significant differences in major clinical characteristics among the three groups was confirmed; however, the complete en-bloc technique significantly shortened the operation time and provided superior enucleation efficiency compared with the remaining two approaches. Although this was because, at least in part, of the accumulated experience in HoLEP by the individual surgeons until the introduction of this new approach, the positive results with the complete en-bloc technique can be explained by refinement of the surgical procedure itself rather than the surgeon's experience, considering the markedly different operative outcomes from the two other approaches. In addition, according to our experience of the complete en-bloc technique for extremely large prostates, including those >200 mL, this approach could be safely performed regardless of the size of the prostate.
The safety of the complete en-bloc technique remains to be evaluated. Indeed, there were no significant differences in major postoperative urinary symptoms and perioperative complications assessed at 3 months after surgery, and as for the persistent SUI rate, no significant difference was noted even 6 months after surgery (data not shown) among the three groups. In particular, despite the lack of significant difference in the incidence of persistent SUI among the three groups, it should be required to further refine our surgical technique and to assess long-term postoperative outcomes regarding urinary symptoms considering the increased incidence of persistent SUI after introducing the en-bloc technique. However, we believe that there may be several benefits associated with the safety of the complete en-bloc technique, which cannot be clearly demonstrated by statistical analyses. For surgeons without sufficient experience, incision and segmentation of adenomas may cause a loss of anatomical orientation and result in severe complications, such as bladder or ureteral injury; therefore, it is important to avoid such complications by initially recognizing the correct position of the bladder neck. By using our developed approach, it is possible to visualize the bladder trigone and ureteral orifice at any time during the operation by approaching the bladder lumen at an early stage in enucleation; thus, the procedure could be completed regardless of the presence of the middle lobe hypertrophy.
There are several limitations to this study. First, the data assessed in this study were retrospectively obtained from patients undergoing HoLEP in routine clinical practice; therefore, a prospective study under strict conditions is needed to prove the utility of the complete en-bloc technique achieved in this pilot study. Second, this study involved comparatively well-experienced surgeons. Considering the favorable postoperative outcomes, including the adverse event profile, this technique may make HoLEP easier to perform; however, it is still necessary to evaluate the learning curve of this technique for inexperienced surgeons. Lastly, patients with BPH who are most likely to benefit from this approach should be identified.
Conclusions
We developed a new surgical technique for enucleation of adenomas during HoLEP called the “complete en-bloc technique with direct bladder neck incision.” This new technique markedly improved the enucleation efficiency without compromising the safety compared with our previously performed procedures. Although a prospective study is required to clarify the significance of this technique, our results suggest that this technique can further improve the clinical outcomes of HoLEP in BPH patients, even in difficult cases.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Video S1