
Abstract
Introduction and Objectives:
Standard of care in upper tract urothelial cancer is nephroureterectomy with bladder cuff excision (BCE). However, alternative techniques such as transurethral incision/resection have been used to simplify distal ureterectomy. The optimum strategy is unclear, and current guidelines do not specify a gold standard technique. The objective of this study was to perform a systematic review of the literature, to compare BCE and transurethral distal ureter methods.
Materials and Methods:
A Cochrane and PRISMA-guided systematic literature search was conducted on English language articles from January 2000 to present, reporting on centers’ experience with either BCE or transurethral distal ureterectomy. A cumulative meta-analysis comparison between the two procedures was performed. Primary outcome was intravesical recurrence. Secondary outcomes were local/distant recurrence, surgical margins, and disease-specific mortality (DSM). Groups were compared using chi-square analysis.
Results:
In total, 66 studies were included after excluding 1795. BCE and transurethral groups contained 6130 and 1183 patients, respectively. Mean/median age ranged from 57.5 to 75.2 years, and follow-up from 6.1 to 78 months. Level of evidence was low, with high risk of bias and small sample size (<100 patients) in 41 (62%) and 52 (79%) studies, respectively. Baseline cancer demographic analysis identified significantly higher rates of high grade, advanced stage, node-positive and carcinoma in situ disease in the BCE group. However, intravesical recurrence (23.6% vs 28.7%, p = 0.0002) and local/distant recurrence (17.9% vs 21.6%, p = 0.02) were significantly lower than the transurethral group. No difference was seen regarding surgical margins (3.1% vs 2.4%, p = 0.27) or DSM (16.8% vs 14.3%, p = 0.06).
Conclusions:
No prospective, randomized comparisons exist for distal ureterectomy at nephroureterectomy. In this analysis, patients undergoing BCE had more advanced disease burden compared with the transurethral group. Despite this, the BCE group had statistically lower intravesical and local/distant recurrence. Further prospective research should be encouraged to identify gold standard ureter management.
Introduction
Upper urinary tract urothelial cancer (UTUC) is a rare disease that accounts for less than 5% of urothelial tumors, with an annual incidence ranging from 0.8 to 1.7 cases per 100,000 people. 1 The disease remains lethal in modern times with 48% 5-year survival. 1 UTUC can arise anywhere from the renal calyces to the distal ureter, and given this, bladder urothelial carcinoma recurrence is common, occurring in 15% to 50% of patients after treatment. 2
Management of UTUC remains challenging, with the current standard of care nephroureterectomy with bladder cuff excision (BCE) for patients with a normal contralateral kidney. 3 Complete excision of the ureter to the level of the bladder is thought to be important, as a retained ureteral segment after incomplete nephroureterectomy may act as a possible site for local recurrence and may contribute to bladder recurrences or metastases. 3
A number of alternative techniques for the management of the distal ureter have been used to simplify distal ureter management, and their use varies from center to center. 4 This includes transurethral, endoscopic distal ureter management, in the form of intramural ureteral resection, that is, the Pluck method, or circumferential excision of the ureteral orifice. The optimal method of distal ureter management is unclear, and no specific method is recommended in current guidelines from the EAU. 3
No randomized, prospective clinical trial has been performed, comparing BCE and transurethral distal ureter techniques, with oncologic outcomes varying in retrospective series. 5 Given the variability in the use of BCE among centers and the uncertainty of the optimum distal ureteral technique, we performed a systematic review of the contemporary literature and cumulative analysis, to assess oncologic outcomes for patients undergoing BCE vs transurethral distal ureter management.
Materials and Methods
Search strategy and study selection
A PRISMA-guided systematic literature search was conducted for contemporary English language articles from January 2000 to September 2017, using the Medline, PubMed, and Cochrane Library. The MeSH term “nephroureterectomy” and variations thereof, including “nephro-ureterectomy” “ureteronephrectomy,” and “uretero-nephrectomy,” with Boolean operators, were used to refine the search.
Studies report on outcomes following nephroureterectomy in adult patients with nonmetastatic UTUC. Studies had to comply with the following inclusion criteria: report on the primary outcome, that is, bladder recurrence, utilize either BCE or transurethral distal ureter management, and a minimum of 10 participants.
Randomized clinical trials as well as prospective or retrospective nonrandomized comparative studies and noncomparative series reporting on outcomes in ≥10 patients were included in this systematic review. If two or more studies reported outcomes of overlapping series (i.e., by the same surgical team), the one with the greater sample size was selected.
The primary outcome was intravesical recurrence. Secondary outcomes were other recurrence (local [nonintravesical], lymph nodes or distant metastases), positive margins, and disease-specific mortality (DSM).
Data extraction and analysis
Data from all selected studies were independently extracted by two authors (S.M.L. and A.M.) and subsequently cross-checked by the senior author to ensure accuracy. A standardized data extraction form was created and used to collect the following variables extracted from each study: tumor location, tumor stage, tumor grade, presence of carcinoma in situ (CIS), nodal status, positive surgical margins, intravesical (bladder) recurrence, other recurrence (local, lymph nodes, or metastases), and DSM. Where DSM was not directly reported, DSM was back subtracted from living patients based on reported follow-up.
Articles included in the study were assessed for risk of bias (RoB) using two domains of the Quality in Prognosis Studies (QUIPs) tool, relevant to observational studies: study participation and outcome measurement. The risk was graded as low, medium, or high independently by two authors. In case of discrepancies, the senior author was involved in the decision process. If an item of the domain was not fulfilled, the risk was ranked as moderate; if two or more items were not fulfilled, the risk was deemed as high. If the risk ranks of the two domains were discordant, the worst rank was used to summarize RoB for the series.
Data were collected using Excel 2013 (Microsoft Corporation, Redmond, WA) and analyzed using SPSS (version 20; IBM, Armonk, NY). Continuous variables were described using mean and standard deviation, or alternatively, median and interquartile range. Chi-square test was used to compare variables. Statistical significance was defined as p < 0.05.
Results
Literature search
After removal of duplicates, two authors independently screened the titles and abstracts of the records for eligibility. Full texts of 163 eligible studies were retrieved and screened independently by two authors. Any disagreement was resolved by consulting the senior author (O.A.). According to the above mentioned criteria, 66 studies were deemed relevant for this systematic review. A PRISMA flowchart describing the study selection process is presented in Figure 1.
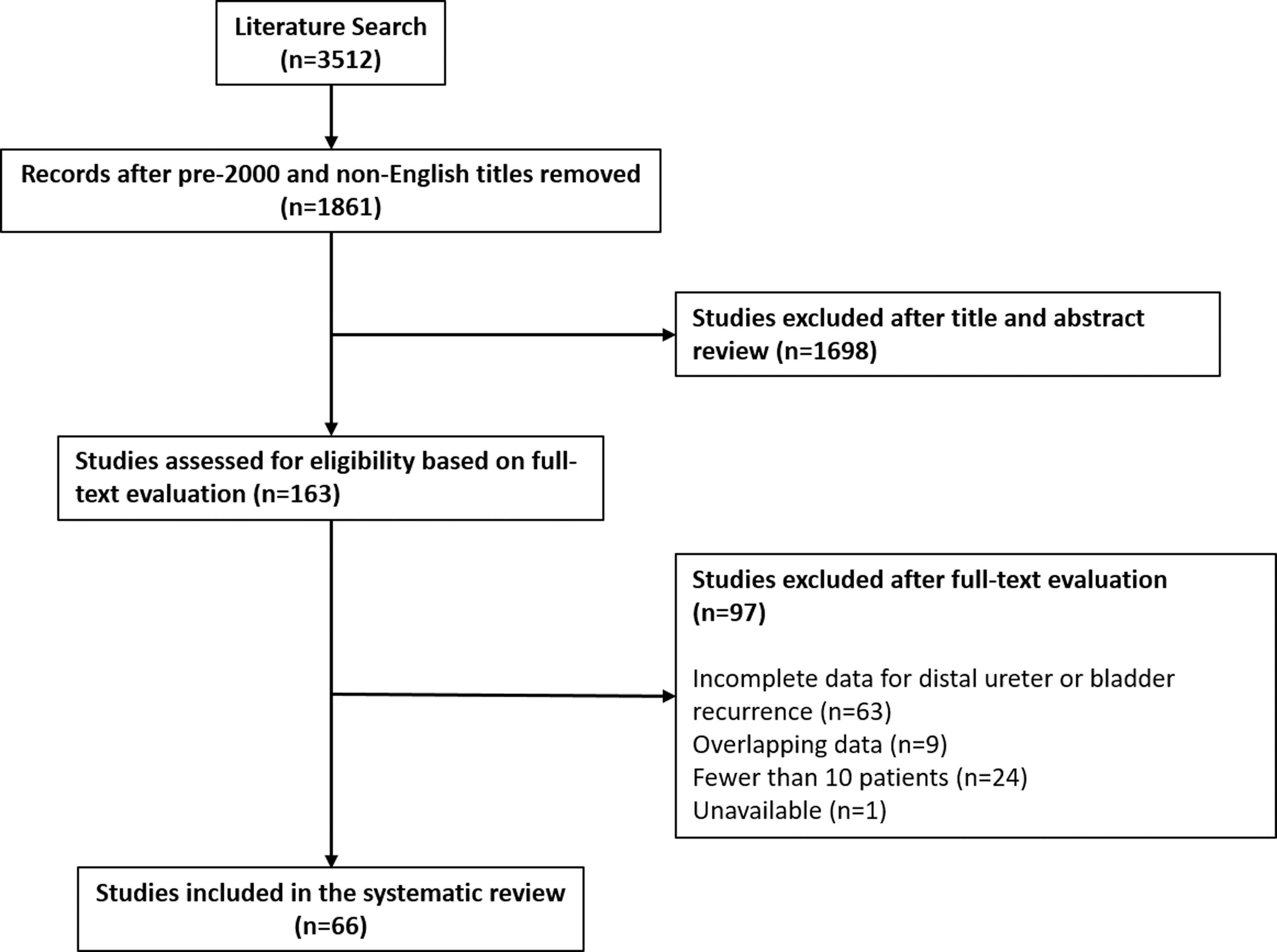
Flowchart of article selection process for review.
Characteristics of included studies
Overall, the 66 studies enrolled 7313 patients: 6130 with a mean age of 69.8 years in the BCE and 1183 with a mean age of 70 years in the transurethral groups. 6 –71 The BCE group consisted of 51 studies, while the transurethral group had 25 studies. Only 10 studies directly compared BCE and transurethral distal ureter techniques. The majority of reports had small sample sizes, with only 14 studies having greater than 100 patients included. Mean/median follow-up varied greatly between studies. Mean/median follow-up ranged from 6.1 to 78 months, across all studies. For each group, follow-up ranged from 6.1 to 78 months in the BCE group and 8 to >60 months in the transurethral group.
Patient characteristics for the studies comprising the BCE and transurethral groups are summarized in Tables 1 and 2, respectively. Within both groups, variables, including nephroureterectomy technique (open or minimally invasive), tumor grade, tumor stage, and tumor location, were well reported in 73% to 100% of studies. However, possible confounders, including previous bladder cancer, CIS, and nodal status, were poorly reported, with only 45%, 22%, and 49% of studies in the BCE group and 36%, 16%, and 52% of studies in the transurethral group reporting on these variables, respectively.
Patient Characteristics of Studies Included in Bladder Cuff Excision Group
CIS = carcinoma in situ; DSM = disease-specific mortality.
Patient Characteristics of Studies Included in the Transurethral Group
TCIUO = transurethral circumferential incision of the ureteral orifice.
No prospective studies on distal ureter management at time of nephroureterectomy are available, with only retrospective comparative studies and retrospective case series. As all studies were retrospective in nature, level of evidence was low. Overall, RoB was considered low in 12 studies, moderate in 13 studies, and high in the remaining 41 studies.
Comparison of baseline cancer demographics found significantly higher rates of G3/high grade and ≥T2 disease, node-positive disease, and CIS disease in the BCE group (Table 3). In addition, a significantly higher proportion of patients in the BCE group had previous bladder cancer (Table 3). Patients in the transurethral management group were more likely to have disease confined to the kidney and renal pelvis (Table 3). The data did not include information on prior endoscopic intervention for biopsy or a tubal prosthesis, that is, stent, before definitive nephroureterectomy.
Distal Ureteral Techniques Used Within the Bladder Cuff Excision and Transurethral Groups
Distal ureteral management
Table 3 summarizes the primary techniques and variations utilized in each group. Distal ureter management in the BCE group studies was variable, using techniques ranging from traditional open intravesical, to completely minimally invasive, or extravesical tenting approaches. Within the BCE group, 4437 patients had a traditional open BCE, using either an intravesical (cystotomy) or extravesical approach. The remaining 1693 patients had a completely minimally invasive approach, with either robotic or laparoscopic BCE or extravesical tenting.
The transurethral detachment techniques were all variations on two main approaches: transurethral resection of the ureteral orifice, that is, the “Pluck” technique or transurethral circumferential incision of the ureteral orifice (TCIUO). The Pluck technique was performed through transurethral resection or bipolar vaporization of the UO, and in some studies, synchronous ligation, clipping, or stapling of the ureter were performed before transurethral management of the UO. TCIUO was performed using a Collins knife in all studies, with or without ureteral ligation or stapling.
Outcomes of distal ureteral management
For the primary and secondary outcome measurements, most available information concerned the number of patients with an event at time of follow-up. There was little time-to-event data, including hazard ratios, p-values, and multivariate adjustment. Therefore, the main analysis is based on a comparison of the overall percentage of patients with an event during follow-up. Data from each study were combined to obtain an overall estimate and compared using a Pearson chi-square test. Cumulative patient characteristics are shown in Table 4.
Cumulative Analysis of Distal Ureter Technique Patient Characteristics and Outcomes
Significant p < 0.05.
Primary outcome measure
Intravesical recurrence was reported by all included studies in both groups. During follow-up, intravesical recurrence was significantly lower in the BCE group patients, 23.6%, vs the transurethral management group, 28.7% (p = 0.0002*, OR 0.77, 95% CI 0.67, 0.88).
Secondary outcome measures
In the BCE group, other recurrence (local or systemic) and DSM was reported in 98% and 90% of included studies, respectively, while in the transurethral group, these variables were published in 76% and 72%, respectively. Other recurrence was significantly lower in the BCE vs the transurethral group, 17.9% vs 21.6%, respectively (p = 0.02*, OR 0.79, 95% CI 0.66, 0.96). No difference between the two groups was seen for DSM (BCE 16.8% vs transurethral 14.3%, p = 0.06, OR 1.21, 95% CI 0.99, 1.48).
Positive surgical margins were reported in 92% and 92% of studies in the BCE and transurethral groups, respectively. There was no significant difference in positive margins between the BCE and transurethral groups: 3.1% vs 2.4% (p = 0.27, OR 1.30, 95% CI 0.82, 2.08).
Discussion
Summary of results
While the standard of care for UTUC is radical nephroureterectomy, current guidelines do not specify the ideal technique for management of the distal ureter. 3 We performed a systematic review and cumulative analysis of the literature to assess contemporary (2000–2017) oncologic outcomes for UTUC patients undergoing nephroureterectomy with either BCE or transurethral distal ureter management.
We found that patients who underwent BCE had significantly higher rates of high grade (69.7% vs 59.8%; p < 0.0001) and staged (53.3% vs 47.3%; p = 0.0004) disease compared to the transurethral group, including higher rates of CIS (24% vs 15.4%; p = 0.0005). Despite having more advanced disease, results have shown significantly lower bladder recurrence rate (23.6% vs 28.7%; p = 0.0002) and distant recurrences (17.9% vs 21.6%, p = 0.02). There was no difference between the two groups regarding positive surgical margins (3.1% vs 2.4%; p = 0.27) or DSM (16.8% vs 14.3%, p = 0.06).
Comparison to the literature
The two largest studies within this systematic review came from two multicenter collaborations, by Kapoor and colleagues 33 and Xylinas and colleagues. 68 Both studies subdivided distal ureter techniques into intravesical BCE, extravesical tenting of the ureter without opening the bladder at another location, and transurethral techniques. The transurethral groups in both studies were comparatively small, representing only 12.0% (98/820) and 3.2% (85/2681) of patients, respectively. The Kapoor study found inferior recurrence-free survival for patients undergoing transurethral distal ureter management vs intravesical BCE (HR 1.488, p = 0.0424). 33 Similarly, Xylinas and colleagues reported higher intravesical recurrence rates in patients undergoing transurethral management (HR 1.74, p = 0.01). The results from both these reports are reflected in the higher intravesical recurrence rate seen in the transurethral group within this study.
Mortality
The population-based study by Lughezzani et al. 5 analyzed the U.S. National Cancer Institute's Surveillance, Epidemiology, and End Results (SEER) database, comparing patients who underwent nephroureterectomy with or without BCE for DSM. The authors found 1.25- to 1.45-fold greater DSM when BCE was not performed in patient with pT3–4 N0/x or pT(any) N1–3 disease.
This increase in DSM was not seen in this review, and may be due, in part, to the wide variations in follow-up between the various included studies. However, taking this into consideration, the mortality rates of those studies with longer follow-ups for BCE vs transurethral treatment were compared: >36 months: 20.47% vs 19.45%; p = 0.06, OR 1.07, 95% CI 0.84, 1.35, >48 months follow-up: 22.5% vs 22.4%; p = 0.98, OR 0.1, 95% CI 0.76, 1.33, and for those with >60 months follow-up: 21.7% vs 25.3%; p = 0.62, OR 0.82, 95% CI 0.38, 1.78. With longer follow-up, it appears that DSM rates favor the BCE group.
In the short-term, the DSM rates are higher in the BCE group and may arise for a number of reasons. These results are interesting, particularly as local and systemic recurrences were lower in this same cohort. As previously discussed, the BCE group had higher disease burden vs the transurethral group. Furthermore, all included studies were retrospective, and the timing of patient mortality was not included in the studies. It is also unclear about the proportion of patients who underwent adjuvant or neoadjuvant chemotherapy before surgery. It is possible that those with the highest disease burden included in the BCE group died early in the follow-up, which would explain the higher early mortality, with similar mortality displayed on long-term follow-up. Some of these patients may have been unfit, denying the use of adjuvant chemotherapy following surgery.
Strengths and limitations of review
This systematic review comprehensively investigates the currently available contemporary (all articles published after 2000) literature and gives the best evidence regarding distal ureter management at time of nephroureterectomy to date. However, despite this, the quality of the evidence obtained was low. Studies were retrospective with no well-designed prospective studies with low RoB. Heterogeneity in study design, populations, and incomplete reporting of patient characteristics and outcome data limited the analyses that could be performed. Follow-up also varied from study to study, ranging from less than 1 year to greater than 5 years.
Finally, there was technique discrepancy in method of BCE within the group. A combination of open intra- and extravesical BCE was used along with minimally invasive techniques, including extravesical tenting and ligation. There is debate as to whether this extravesical tenting of the bladder followed by stapling, Ligasure or similar ligation of the UO and bladder cuff are equivalent to formal BCE. Indeed, larger cohort studies, including Kapoor and colleagues 33 and Xylinas and colleagues, 68 included these as a separate group. While Kapoor found significantly higher intravesical recurrence rates in the extravesical tenting group, no difference was seen in the Xylinas and colleagues cohort.
Nonetheless, this represents the existing evidence, based on a thorough, high-standard protocol-driven systematic review and analysis of the results.
Implications for practice and research
Although renal pelvic cancer is more common than distal ureteral disease, this study has found significantly more centers performing BCE as opposed to transurethral distal ureteral procedures. This emphasizes that although the evidence is not yet established, clinical intuition or practice has led to more surgeons moving away from transurethral management of the distal end at nephroureterectomy. Nonetheless, generally, this review found that BCE has better oncologic outcomes despite having more advanced disease. However, no difference in DSM was noted.
BCE had more advanced disease but better oncologic outcomes compared to transurethral management. We postulate that in patients with matching disease status, BCE will have better oncologic outcomes and potentially lower mortality.
Although this review is composed of low-grade evidence studies, it does highlight the current uncertainty and lack of high-level evidence in current guidelines regarding the optimum distal ureter technique at nephroureterectomy. There is a pressing need for further prospective, randomized studies to investigate the optimum distal ureter technique. Anecdotally, the increasing need for transurethral confirmation of urothelial carcinoma and the potential effects of manipulation and seeding from the upper tracts remains unquantified and must be documented as part of any future study.
Until such a trial is conducted, based on the evidence provided, we recommend that at time of nephroureterectomy, preference is given to BCE management of the distal ureter.
Conclusions
In this cumulative analysis, patients with BCE distal ureter management had more advanced disease burden compared to the transurethral group. Despite this, there was statistically lower bladder recurrences and local or distant recurrences. Further prospective research in this area should be encouraged to identify gold standard distal ureter management. Until then, we recommend BCE be considered the default technique with nephroureterectomy procedures.
Footnotes
Acknowledgment
The authors thank Dr. Isra Ashi for her support.
Author Disclosure Statement
No competing financial interests exist.