
Abstract
Aim:
To evaluate and study the efficacy of intraoperative renal stone culture (IOSC) in predicting postpercutaneous nephrolithotomy (PCNL) urosepsis (PPS) and systemic inflammatory response syndrome (SIRS). PPS is known to occur in patients despite negative preoperative midstream urine culture (MSUC).
Methods:
After obtaining institutional ethics committee approval and informed consent, 78 selected patients undergoing PCNL were evaluated as per protocol for risk factors for SIRS criteria with MSUC, intraoperative renal pelvic urine culture (RPUC), and IOSC.
Results:
MSUC was positive in six (7.7%) patients. The sensitivity, specificity, PPV, negative predictive value (NPV) and respiratory rate of MSUC for detecting SIRS were 20%, 93.15, 16.67%, 94.44%, and threefold, respectively. RPUC was positive in five (6.9%) patients with a specificity and NPV of 92.64% and 94.02%, respectively. IOSC positivity was seen in four (5.1%) patients with specificity and NPV of 94.5% and 3.2%, respectively. SIRS developed in five (6.4%) patients. MSUC, RPUC, and IOSC could not demonstrate any significant association with the occurrence of SIRS. Postoperative urine culture (POUC) was positive in 1/5 SIRS patients and no significant association (p < 0.182) could be demonstrated between the risk factors and PPS. Most complications were minor, while the mean hospital stay was significantly higher in SIRS patients.
Conclusions:
While MSUC, RPUC, and IOSC were less sensitive in predicting the occurrence of SIRS/urosepsis in patients undergoing PCNL, nevertheless, we recommend routine IOSC for stone colonizing bacteria in at-risk select patients to predict potential PPS/SIRS. POUCs could be used in symptomatic SIRS to guide antimicrobial therapy in post-PCNL patients. Positive peri/intraoperative urine cultures may assist the urologist in directing appropriate antibiotics to prevent potential urosepsis in post-PCNL patients. Those with a higher blood transfusion rate and Clavien complications were at increased risk of PPS/SIRS. Escherichia coli was the most frequently isolated microbe followed by Klebsiella and Proteus, which were mostly sensitive to nitrofurantoin.
Introduction
Percutaneous nephrolithotomy (PCNL) is a standard operative procedure currently indicated for the vast majority of renal calculi. Urosepsis is an uncommon (0.9%–4.7%) 1 event and the most common cause of mortality rate in patients undergoing PCNL, 2 which may occur despite ensuring asepsis, a sterile midstream urine culture (MSUC), and administering prophylactic antibiotics. 3 The probable reason postulated by workers is release of bacteria from the fragmented calculi or introduction of bacteria via the PCNL tract. Post-PCNL urosepsis (PPS) may manifest itself as a systemic inflammatory response syndrome (SIRS) in up to 66%–80%. 4
According to Draga and colleagues, 5 SIRS criteria may be considered in patients with more than one of the following clinical features: (i) body temperature higher than 38°C or lower than 36°C, (ii) heart rate (HR) >90/minute, (iii) respiratory rate >20/minute or PaCO2 <32 mmHg, and (iv) total leukocyte count (TLC) >12,000/mm 3 or <4000/mm 3 . The primary outcome measures used for detecting PPS/urinary tract infection (UTI) in our cohort of patients were intraoperative stone culture (IOSC), intraoperative renal pelvic urine culture (RPUC), postoperative urine culture (POUC), in which positive cultures were correlated with features of SIRS. Hemogram, TLC, renal function test, serum electrolytes, blood culture, and ultrasonography (USG) abdomen were evaluated at 48 hours post-PCNL. The secondary outcome measures used were the association of risk factors with post-PCNL urosepsis/SIRS, mean modified Clavien grade of complications, antibiogram, and mean hospital stay (HS).
Materials and Methods
After obtaining written informed consent and institutional ethics committee (IEC) approval, a prospective randomized observational analytical study was performed on 78 eligible patients from November 2016 to April 2018. The protocol of this study was registered with the Clinical Trials Registry of India (CTRI) as CTRI/2018/03/012765. The primary intent to diagnose and treat patients with whatever necessary as consistent with good clinical practices was followed as far as feasible, subject to our protocol and IEC limitations.
Patients were selected as per inclusion criteria (adults >18 and <80 years, indications for PCNL, anesthetically fit for surgery, and a sterile MSUC). Patients with preoperative stents/percutaneous nephrosomy (PCN) in situ/indwelling catheter, positive MSUC/UTI/pyonephrosis, concomitant/contralateral ureteral/bladder stone, concomitant antibiotics and nonconsenters, those unable to comply with protocol requirements, and those with contraindications to PCNL (uncorrected coagulopathy, pregnancy, unsafe access, pulmonary and cardiac disease, morbid obesity) were excluded from this study.
MSUC was done at least 7 days before surgery and those positive were treated with antibiotics to ensure a sterile MSUC before PCNL. Preoperative antibiotics were given in MSUC-negative patients as per AUA best practice guidelines. 6 Screening kidney, ureter, and bladder radiograph (KUB), ultrasound abdomen, chest X-ray, renal function test, intravenous pyelography renal scan (if indicated), and preanesthetic evaluations were done in all patients. Cultures with greater than 1000 colony forming units (CFU)/mL of one type of bacteria usually indicated infection after 48 hours of incubation.
While puncturing the renal system for PCNL, an RPUC sample or urine sample via a ureteral catheter was considered RPUC. After establishing the PCN tract, PCNL was performed in the usual manner. The first stone fragmented was retrieved and sent for stone culture after processing. The stone fragment was processed by washing it four times and crushing it in sterile saline using the technique described by Nemoy and Stamey 7 and was sent for IOSC. A semiquantitative culture using the calibrated loop technique was done on CLED medium, and the Kirby–Bauer disc diffusion method was used for antibiotic sensitivity testing; results were interpreted using CLSI (Clinical and Laboratory Standards Institute) guidelines. 8
Patients were followed up for Clavien score of complications and post-PCNL urosepsis/SIRS using the following parameters as per protocol: IOSC and POUC at 48 hours along with hemogram, blood urea, serum electrolytes, and blood culture. Cultures showing varying pathogens isolated in urine samples (MSUC, RPUC, IOSC, POUC) were considered discordant criteria for this study. Postoperative HS, body temperature, HR, and RR were recorded, while hematocrit, blood urea, serum electrolytes, urine culture, and KUB at 48 hours; blood culture and USG abdomen were repeated if signs of SIRS were present beyond 48 hours.
Other risk factors for PPS/SIRS such as age/sex/body mass index (BMI)/presence of hydronephrosis (HDN)/type 2 diabetes/chronic renal failure/operating time/multiple PCNL tracts/stone burden/prior ipsilateral (IP) renal surgery/blood transfusion (BT)/residual stones were also evaluated for correlation, if any, with PPS. The typical flow pattern of the present study is depicted in Figure 1.
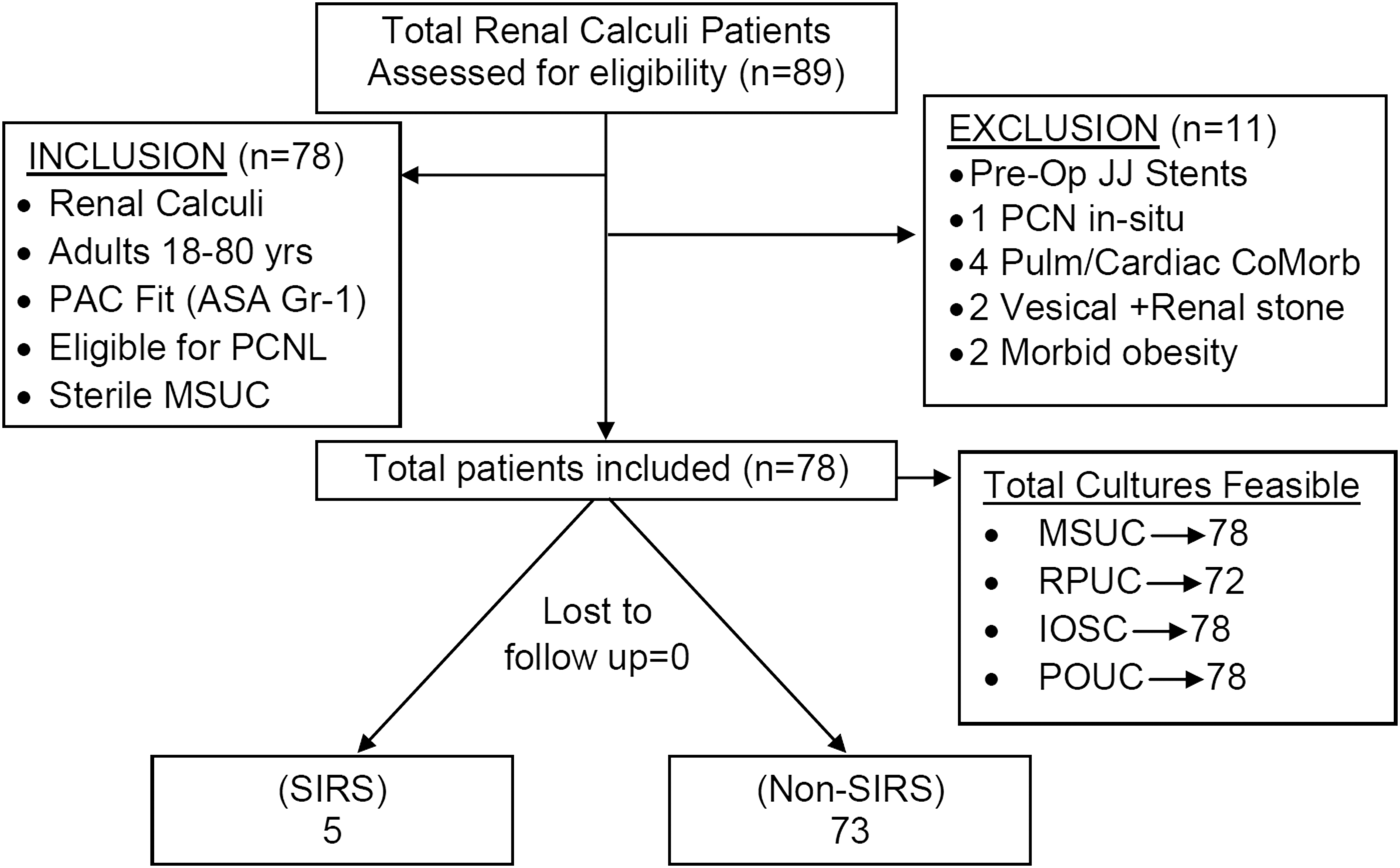
Depicting the flow chart pattern of this study.
Sample size was computed by considering 1:3 ratio (based on a 25% stone culture-positive rate in prior studies), 9 80% power, and 5% level of significance, for which an estimated 72 POUC-negative cases were required. Chi-square and Fisher's exact test were used to compare other risk factors.
Results
MSUC was positive in 6/78 (7.7%) patients, while IOSC was positive in 4/78 (5.1%) patients, as depicted in Figure 2a. In the four patients with a positive IOSC, Escherichia coli, mixed growth, and proteus vulgaris were cultured in two, one, and one patient, respectively. Three of four patients with positive IOSC were also positive for MSUC (E. coli in two and mixed growth in one patient), suggesting 100% concordance between MSUC and IOSC. RPUC was collected in 72 patients and was positive in 5/72 (6.9%) patients, in which E. coli was the commonest pathogen isolated (100% sensitive to nitrofurantoin [NFT]) in one followed by mixed growth in four as depicted in Figure 2b. In nine patients with positive intraoperative cultures (five and four patents with positive RPUC and IOSC, respectively), NFT was administered as per sensitivity report to prevent urosepsis.

Depicting the flow diagram of various culture-positive prevalences
The antibiogram of various cultures is depicted in Figure 2c. Positive IOSC and RPUC in the presence of sterile MSUC were identified in one (25%) and two (40%) patients, respectively. However, there were three (4.16%) cases with positive MSUC and RPUC, in which the same organism was cultured in two, thereby suggesting a concordance rate of 66.7% between MSUC and RPUC. In the present study, MSUC correctly predicted in IOSC with 75% sensitivity, 95.9% specificity, and a positive predictive value of 50% (Table 1). MSUC predicted correct organism in RPUC patients with 75%, 95.58%, and 50% sensitivity, specificity, and positive predictive value, respectively (Table 2). RPUC predicted the correct organism in IOSC with 75%, 97.05%, and 60% sensitivity, specificity, and positive predictive value, respectively (Table 3).
Comparison of Midstream Urine Culture with Intraoperative Renal Stone Culture
IOSC = intraoperative renal stone culture; MSUC = midstream urine cultures.
Comparison of Renal Pelvic Urine Culture with Midstream Urine Culture
RPUC = renal pelvic urine culture.
Comparison of Intraoperative Renal Stone Culture with Renal Pelvic Urine Culture
RPUC could not be collected in six patients.
Fever was detected in all five patients with SIRS post-PCNL (Table 4). SIRS developed in five (6.41%) patients in whom IOSC and RPUC were negative; in all patients with SIRS, mixed growth was seen in one patient with a positive MSUC. Blood cultures were negative in all patients with SIRS. Female patients were predominant in SIRS patients. POUC was positive in one SIRS patient for E. coli, which resulted in a change of the antimicrobial treatment. Thus, in the present study, IOSC and RPUC appeared to guide targeted antimicrobial therapy in at least four and five (total nine) of our patients, respectively.
Systemic Inflammatory Response Syndrome Diagnostic Parameters in Postpercutaneous Nephrolithotomy Five Patients with Systemic Inflammatory Response Syndrome
HR >90, RR >20/min, TLC >12,000, temperature >98.4°F were the deemed criteria used in this study to establish SIRS.
HR = heart rate; RR = respiratory rate; SIRS = systemic inflammatory response syndrome; TLC = total leukocyte count.
Intergroup comparison of mean stone burden was 2.23 ± 0.97 cm (vs 1.96 ± 0.58 cm in SIRS patients), which was similar. All patients received a PCN tube at the termination of the procedure, while additional Double-J stenting was done in 68/78 patients (4/5 patients with SIRS had concomitant Double-J stenting); however, Double-J stenting was not associated with a higher risk of SIRS (p = 1.000) in this study. As a departmental unit preference, we attempted to place Double-J ureteral stents where ever feasible in most patients alongside the PCN tube to facilitate an earlier PCN tube removal and rapid convalescence.
Clavien (G1, G2-minor) complications were observed in two (2.6%) and eight (10.3%), respectively, while Clavien (G3-major) complication was observed in three (3.84%) patients. These patients had a significantly higher risk of SIRS (p = 0.000). SIRS was significantly higher in patients with BT (p = 0.031). Comorbidities and known risk factors evaluated were not associated with any increased risk of SIRS (Table 5), and the HS was significantly higher among patients with SIRS in this study (p = 0.021).
Depicting Comparison of Demographic/Risk Factors in Patients With/Without Systemic Inflammatory Response Syndrome
Indicates p value was highly significant.
Indicates p value was significant.
BT = blood transfusion; CRF = chronic renal failure; DM = diabetes mellitus; HDN = hydronephrosis; HS = hospital stay; I/L = ipsilateral; PCN = percutaneous nephrostomy; ORT = operation room time; SD = standard deviation.
Discussion
In the present study, SIRS was encountered in five (6.41%) post-PCNL patients despite appropriate antimicrobial prophylaxis, which suggested that MSUC was an unreliable predictor of SIRS, in conformity with that reported by other researchers. 9 –12 Positive IOSC was observed in 4/78 (5.1%) patients despite negative MSUC, and RPUC was positive in 5/72 (6.9%) patients, which appeared to suggest that these patients were more prone to PPS/SIRS.
Among the patients with SIRS, one patient had mixed growth in MSUC (subjected to 7 days of ciprofloxacin therapy despite which the patient developed SIRS). IOSC and RPUC were negative in our patients with SIRS, however, it appeared that a negative IOSC was observed to be more specific than MSUC/RPUC in correctly predicting a negative SIRS in post-PCNL patients. Patients with positive IOSC and RPUC did not develop SIRS, possibly due to patients being subjected to immediate antibiotic therapy as per the culture reports.
In the present study, the concordance rate between MSUC and RPUC was 2/3 (66.67%). The concordance rate for IOSC/MSUC was 100%, which suggested that IOSC was a better reflection of the internal milieu of the urinary system as it tends to form in infected urinary tract. The concordance rate of IOSC/RPUC was 2/3 (66.67%) patients in our study, and POUC at the time of SIRS could be used to guide appropriate antibiotics in some patients. Gram-negative organisms were predominant cultures in this study and the same has been documented by other researchers. 9 The most common organism isolated from IOSC was E. coli in 2/4 (50%) patients followed by proteus vulgaris and mixed growth; E. coli was also the most common organism in RPUC and further was sensitive to NFT (sensitivity 100%) and resistant to ciprofloxacin.
In our study, in nine patients (non-SIRS) undergoing PCNL, the intraoperative cultures were beneficial in directing targeted antimicrobial therapy, while POUC was beneficial in only one patient (non-SIRS) for the same. Thus, a total of 10 (12.8%) patients seemed to have benefited from various pre/intra/peri/postoperative cultures and the same was useful in directing a targeted change in appropriate antibiotics and was probably beneficial in preventing potential PPS. It is with this caveat that we feel perioperative cultures may have a vital role to play in select patients.
According to published studies, the prevalence of SIRS in post-PCNL patients has been reported to be as high as 15%–30%, 5,13 with the reported incidence of clinically overt PPS varying from 0.9% to 4.7%. 1,14 In the present study, SIRS occurred in five (6.4%) patients that was comparable with other studies. 10,15 –21 We have reviewed and tabulated the salient findings from various articles in the published English literature and PubMed(TM), depicted in Table 6.
Depicts Comparison of Systemic Inflammatory Response Syndrome Rate, Positive Midstream Urine Culture and Sensitivity, Stone Culture and Sensitivity, Pelvic Urine Culture and Sensitivity and Their Concordance Rates as Reported in Various Studies
p value not defined.
BP = better predictor of sepsis/SIRS; N = no. of patients; PNR = prospective nonrandomized study; PP = poor predictor of sepsis/SIRS; RCT = randomized control trial; RS = retrospective study; RSF = residual stone fragments.
Chew and coworkers 21 conducted a multi-institutional, randomized controlled trial in 86 patients undergoing PCNL to define the risk factors for SIRS; these authors demonstrated that the intraoperative PCN tube placement was the sole predictor of PPS, while RPUC, IOSC, and MSUC failed to predict the risk of post-PCNL SIRS, although the authors admitted in their limitations that they had included patients presumed to be at low risk for sepsis.
Degirmenci and colleagues 20 in a prospective study assessed 729 PCNL patients (SIRS in 35), with residual stone fragment (RSF)-related infectious complications. These authors demonstrated that while patients with post-PCNL RSF were associated with PPS, however, the IOSC and RPUC positivity did not appear to pose any additionally significant risk for PPS/infectious complications.
Elshal and coworkers 22 also attempted to define the role of IOSC in 84 patients undergoing PCNL who demonstrated positive IOSC in 23/84 (27.4%) and concluded that routine IOSC was of limited utility and only positive MSUC (p = 0.02) and leukocytosis (p = 0.01) could reliably predict the occurrence of SIRS. Osman and colleagues 23 too in a study on 79 patients undergoing PCNL encountered SIRS in 12/79 (15.2%) of their patients and demonstrated that routine IOSC did not affect antimicrobial therapy and only leukocytosis was a reliable predictor of SIRS, while neither culture was useful in predicting the occurrence of SIRS.
Gonen and coworkers 19 in a prospective study on 61 patients undergoing PCNL analyzed the factors responsible for post-PCNL fever and demonstrated a significantly positive IOSC for patients in the fever group vs no fever group (5/10 vs 9/51, p < 0.05) and concluded that routine IOSC was important in guiding antibiotic therapy in post-PCNL fever, although the authors failed to conclude its efficacy in detecting post-PCNL SIRS.
Mariappan and colleagues 9 in another prospective study on 54 PCNL patients demonstrated that the stone entrapped bacteria were responsible for PPS and concluded that RPUC was better than bladder urine culture in predicting infected stones and those with infected stones or pelvic urine had four times higher risk for developing urosepsis (p = 0.0009). However, these authors admitted using only the HR as their sole criteria for defining post-PCNL SIRS (contrary to definition of SIRS by Consensus Committee report). 9
Paonessa and coworkers 11 in a study examined the relationship between MSUC and IOSC (after omitting RPUC) in a large cohort of 776 PCNL patients and compared their findings in infectious vs metabolic calculi and demonstrated a 25% discordance in IOSC in their cases with a prominent shift toward gram-positive organisms in cultures.
Roushani and colleagues 12 in a correlation between MSUC and IOSC in 51 PCNL patients with UTI or post-PCNL SIRS demonstrated a 10-fold increased risk of SIRS in patients with positive IOSC (p = 0.002) and concluded that positive IOSC was a significant predictor of post-PCNL-SIRS regardless of other factors.
Margel and coworkers 13 in a prospective study on 75 PCNL patients studied the correlation between MSUC and IOSC and concluded that MSUC often failed to localize stone-colonizing bacteria and that routine use of IOSC was essential to direct appropriate antibiotics. Devraj and colleagues 13 in an analytical study on 83 consecutive patients undergoing PCNL studied the utility of MSUC, RPUC, and IOSC in predicting PPS and demonstrated the occurrence of SIRS in 20/83 (25%) of their patients and concluded that IOSC was a better predictor of potential urosepsis than RPUC/MSUC and these authors recommended that use of routine IOSC was essential for the diagnosis and management of PPS.
Risk factors for PPS/SIRS: Age and BMI did not appear to increase the incidence of SIRS in our study. However, SIRS may tend to have a female predominance as documented by other researchers, 5,9,16,21,23,24 with the female gender being more prone to recurrent genitourinary infections/UTI due to a short urethra, urethral proximity to anus, intercourse-related trauma, and pregnancy/menopause-induced hormonal changes.
The mean stone burden in the present study was 2.23 ± 0.97 cm (vs 1.96 ± 0.58 cm in SIRS patients), which was partially responsible for the lower incidence of SIRS observed in this study as bacteriuria tends to be more prevalent in stones greater than ≥10 cm 2 . 15 However, in our study, the stone burden was not too high, and hence, stone size was not a significant risk factor toward SIRS/PPS. Double-J stent insertion too was not associated with SIRS as PCN insertion provided unimpeded drainage of infection pockets in the nondependent calices/urinary tract. RSF were present in 1/5 SIRS patients, which too did not appear to increase the risk of SIRS as demonstrated by other researchers in similar studies. 16,24
RPUC and IOSC were negative in all five SIRS patients. Patients with Clavien grade 1/2/3 complications had a significantly higher risk of SIRS, but there was no mortality rate in any patient. There was a significant increase in the need for BT among SIRS patients (p = 0.031), which has been demonstrated by other workers in similar studies. 17,24 It is postulated that patients with narrow calyces/caliectasis could be more prone to more injuries in upper urinary tract, facilitating bacterial inoculation in the disrupted renal parenchyma and the translocation into systemic circulation with subsequent sepsis.
Factors such as BT, number of access tracts, RPUC, IOSC, stone size, age, and operative time have also been shown to be significant copredictors of SIRS in PCNL by other workers. 24 Patients with certain comorbidities and risk factors such as hypertension, type 2 diabetes, prior IP surgery, chronic renal failure, Australian antigen positive, hepatitis C positive, hypothyroidism, multiple access tracts, and HDN 21,23,25 in this study were, however, not associated with increased risk of SIRS.
It is postulated that certain patients could be exposed to a higher risk of SIRS/PPS, such as patients with (1) female gender, (2) high stone burden, (3) higher operation room time, (4) higher PCN indwelling time, (5) concomitant Double-J stents and PCN tube, (6) residual stones, and (7) comorbidities such as HT, type 2 diabetes, prior IP surgery, chronic renal failure Australian antigen positive, HDN, and multiple access PCN tracts(>1). However, a larger number of patients with these entities need to be selectively evaluated to better define such patient subgroups, presumed to be exposed to an apparently higher risk of developing PPS/SIRS.
Patients with higher BT rates and Clavien complications may increase the relative risk of developing PPS/SIRS, in which E. coli may be the most frequent culprit followed by Klebsiella and Proteus, which may be mostly sensitive to NFT and resistant to fluoroquinolones. There was a significant increase in the postoperative HS among SIRS patients in this study.
However, MSUC was able to predict IOSC and RPUC with good accuracy. IOSC and RPUC are better reflectors of internal milieu of the upper urinary tract, relatively economical/cost-effective (vs the cost of managing a single episode of PPS), and can be easily collected during PCNL to assist the urologist in guiding necessary antimicrobial prophylaxis in postoperative patients to prevent SIRS and minimize sepsis.
Some reasons have been postulated by us for a low RPUC/IOSC positivity in this study, namely: (1) the majority (78%) of renal stones well documented by us elsewhere 29 tend to be calcium-containing stones of oxalate/hydroxyapatite with only about 7% being primarily infection/struvite-based stones. According to a study published by Kajander and Ciftçioglu 30 on the origin of calcium phosphate stones involving nanobacteria, the authors documented that no genomic material was identified till date, indicating thereby that a majority of renal stones could be sterile from within; (2) there may have been an inadvertent possible delay in transportation/inoculation of the intraoperative stone/urine samples; and (3) furthermore, our patients were referred from the periphery in which they may already have received a prolonged course of antibiotic, not only ensuring a sterile MSUC but possibly also sterilized renal stones, all of which could have contributed toward a lower RPUC/IOSC positivity in the present study, and (4) finally, our patient population undergoing PCNL appeared to have primarily noninfection small burden stones.
Larger carefully designed randomized controlled studies would be better to select independent predictors and risk factors for PPS/SIRS and to detect the precise utility of routine intraoperative stone/urine cultures in patients of urolithiasis undergoing PCNL.
Conclusions
POUC in symptomatic patients with PPS/SIRS could be used to guide antimicrobial therapy in post-PCNL patients. RPUC and IOSC were reliable and better predictors for post-PCNL urosepsis in select high-risk patients. Since cultures are relatively easy and cost-effective to obtain in PCNL, we do recommend RPUC and IOSC in such patients to better predict and manage SIRS/PPS.
Although our outcome in terms of positive intraoperative cultures was not as robust as we had anticipated, nevertheless, we were able to document the utility of the same in guiding and directing appropriate antibiotic therapy in a sizable number of post-PCNL patients. We feel that this study could serve as a useful adjunct clinical guide to improve patient outcomes particularly in terms of lessening SIRS, preventing PPS, and lowering the morbidity of PCNL. Targeted antibiotics may also aid in lowering antibiotic resistance. Our conclusions should thus be read in the light of these observations.
Footnotes
Acknowledgment
The authors certify that the above study was conducted entirely from within regular running expenditure available to the Government Institution and no extra institutional financial grant or funding was availed in any manner whatsoever.
Ethical Statement
The authors declare that the above article is in compliance with the ethical standards for research in human participants and that they have no potential sources of conflict of interest associated with its publication.
Informed Consent Statement
The authors also certify that informed consent was obtained from all the human participants in this study.
Author Disclosure Statement
No competing financial interests exist.