
Abstract
Introduction:
Postoperative lymphatic drainage and lymphocele formation is a common seen complication after extended pelvic lymph node dissection (ePLND) in robot-assisted radical prostatectomy (RARP) operation. The aim of this study was to evaluate autologous fibrin glue as an additional treatment option to reduce the volume of lymphatic drainage and prevent lymphocele development.
Materials and Methods:
A total of 75 patients undergoing transperitoneal RARP with ePLND between January and July 2018 were enrolled in this study. Thirty-five patients who received autologous fibrin glue enrolled to study group, another 40 patients who did not receive to control group. Autologous fibrin glue was applied over the PLND areas. Age, body mass index (BMI), pathologic stages, and number of removed lymph nodes (LNs) were compared. The main endpoint was to compare postoperative lymphatic drainage volume and lymphocele formation rate between groups.
Results:
There was not statistically significant difference between the groups with respect to age, BMI, Gleason score, T-stage, and number of removed LNs. Autologous fibrin glue resulted in 50% (110 mL vs 210 mL; p = 0.037) and 75% reduction of postoperative drainage volume (70 mL vs 270 mL; p = < 0.0001) in study group than control group at postoperative 2nd and 3rd days, respectively. The total drainage volume was also 50% reduced in study group (277 mL vs 577 mL; p = 0.004). The incidence of asymptomatic lymphocele was 20% (n = 7) and 37.5% (n = 15) in study and control groups, respectively (p = 0.112). One patient in control group developed symptomatic lymphocele. There were no immediate or late adverse effects in study group.
Conclusion:
Autologous fibrin glue application reduced postoperative lymphatic drainage, and also lymphocele formation rate after extended PLND in RARP operation.
Introduction
Pelvic lymph node dissection (PLND) is considered to be the most accurate staging method during robot-assisted radical prostatectomy (RARP) for localized prostate cancer. 1 The clinical usefulness of performing PLND is based on better detection of regional lymph node (LN) metastasis and initiation of adjuvant treatment. Despite its potential benefits PLND can lead to several complications frequently associated with lymphocele development, prolonged postoperative lymphatic drainage, and hospital stay. 2,3 Although most of the lymphoceles may be clinically indolent, infection risk, thromboembolic events, compression to iliac vessels, or urethrovesical anastomosis may be detected in some cases. 4 Moreover, complicated lymphoceles may require hospitalization and surgical intervention. Recently published reports have documented 2–8% of symptomatic lymphocele formation after RARP. 2,5,6
Various conventional methods, such as transperitoneal approach, clipping, or bipolar coagulation of lymphatic channels, are used to reduce lymphatic drainage and lymphocele formation. However, these techniques may not sufficiently prevent postoperative drainage and lymphocele formation in majority of cases. Several studies evaluated the efficacy of the fibrin sealants adjunct to conventional methods for reducing lymphatic drainage and lymphocele formation in variety of surgical fields, including urologic, gynecologic, and other surgeries. 3,7 –10 In this study, we aimed to evaluate autologous fibrin glue as an additional treatment option to reduce the volume of lymphatic drainage and prevent lymphocele development.
Materials and Methods
This study was designed at a single center in which patients underwent extended PLND during RARP between January and July 2018. A total of 75 patients were enrolled into two groups; study group (ePLND+ plus fibrin glue; n = 35) or to control group (ePLND alone; n = 40). Hem-o-lok clips and bipolar cautery were used as standard lymphatic control during the extended PLND.
The study originally was designed to prospectively randomize patients into two groups receiving ePLND (control group) and ePLND plus autologous fibrin glue (study group). However, after monitoring the significant decrease in lymphatic drainage amount in study group patients, it was planned to continue application of fibrin glue in consecutive patients and compared with previously operated patients. All procedures were performed by the same surgical team.
Surgical technique
The RARP was performed by the standard transperitoneal approach as previously described. 11 The absolute indication for ePLND was Gleason >7 score or PSA >10 ng/mL or T3 disease. The risk of LN involvement was also calculated in all patients according to nomograms. 12,13 Extended PLND was performed in all patients enrolled in this study as previously described. 2 Lymphatic tissue was ligated with medium or large Hem-o-lok® clips (Teleflex Medical, Research Triangle Park, NC) and bipolar cautery was also used for coagulation of small vessels in all patients. In study group, 4–5 cc of autologous fibrin glue—Vivostat™ (Vivostat A/S, Alleroed, Denmark) was spread on bilateral dissection areas in addition to surgical clips and bipolar cautery for lymphatic control. Vivostat is an automated system for preparation of human blood-derived purified fibrin. The preparation unit isolates 6–6.5 mL fibrin solution from 120 mL blood sample. Fibrin glue polymerases immediately after contacting with the tissues within seconds (Fig. 1).
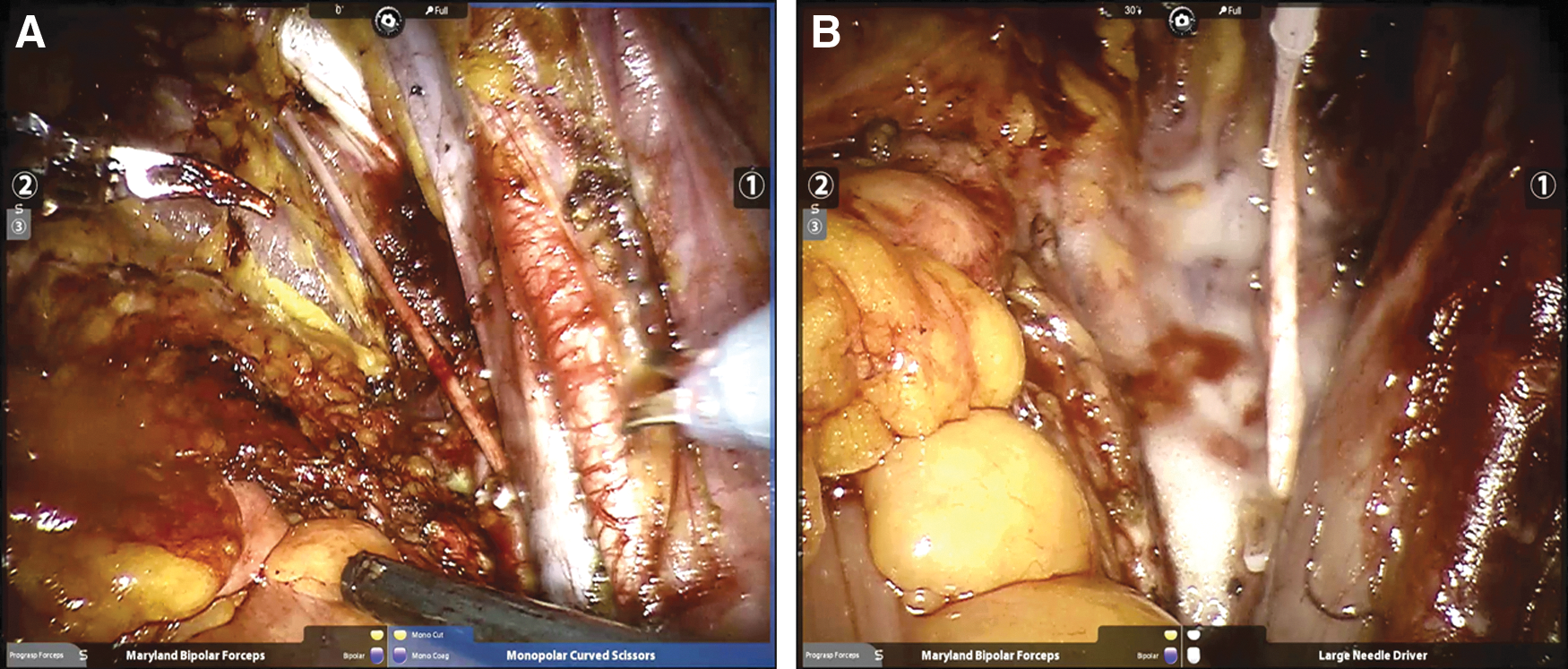
Fibrin glue (Vivostat) sprayed over the extended pelvic lymph node dissection area
Postoperative follow-up
The Jackson–Pratt (J–P) suction drain placed through the left 8 mm robotic port. Drainage volume was recorded every 4–6-hour interval. Drain catheter was removed when 8-hour shift volume was <50 mL. Foley catheter removed on postoperative 7th day. Lymphocele formation and lymphocele characteristics were checked by ultrasonography after urethral catheter removal and at first month of follow-up or when symptomatic lymphocele formation was suspected.
Statistical analysis
Patients' age, body mass index (BMI), Gleason score, drain and Foley catheter removal, and number of removed LNs were used for analysis. For continuous variables Mann–Whitney U test or Wilcoxon-sample tests were used with median (interquartile range) or mean (standard deviation) parameters. Chi-square test or Fisher's exact test were used for categorical comparisons. Statistical analysis was done with SPSS (Software Package for Social Sciences, NY). p < 0.05 considered as statistically significant.
Results
A total of 75 patients were included in the study; 40 of them underwent RARP with extended PLND (control group), whereas 35 received autologous fibrin glue plus to extended PLND (study group). We prospectively collected demographic, peri-, and postoperative data of patients enrolled in study group. The demographic data for both groups is shown in Table 1. There was not statistically significant difference between the groups regarding age, pT-stage, PSA levels, and BMI. The number of removed LNs was 30 (range 13–49) and 31 (12–55) in study and control groups (p = 0.941). Positive LNs were reported in two patients, one in each group.
Baseline Patient Characteristics
Postoperative drainage characteristics are shown in Table 2. The daily (24 hours) output volume was statistically significantly lower in study group than the control group at postoperative day 2 (median 110 mL vs 210 mL; p = 0.037) and day 3 (70 mL vs 270 mL; p < 0.0001). The total drainage volume was also 50% reduced in study group (310 mL vs 577 mL; p = 0.004) (Fig. 2). Median duration of drain catheter removal was similar in both groups (p = 0.717).
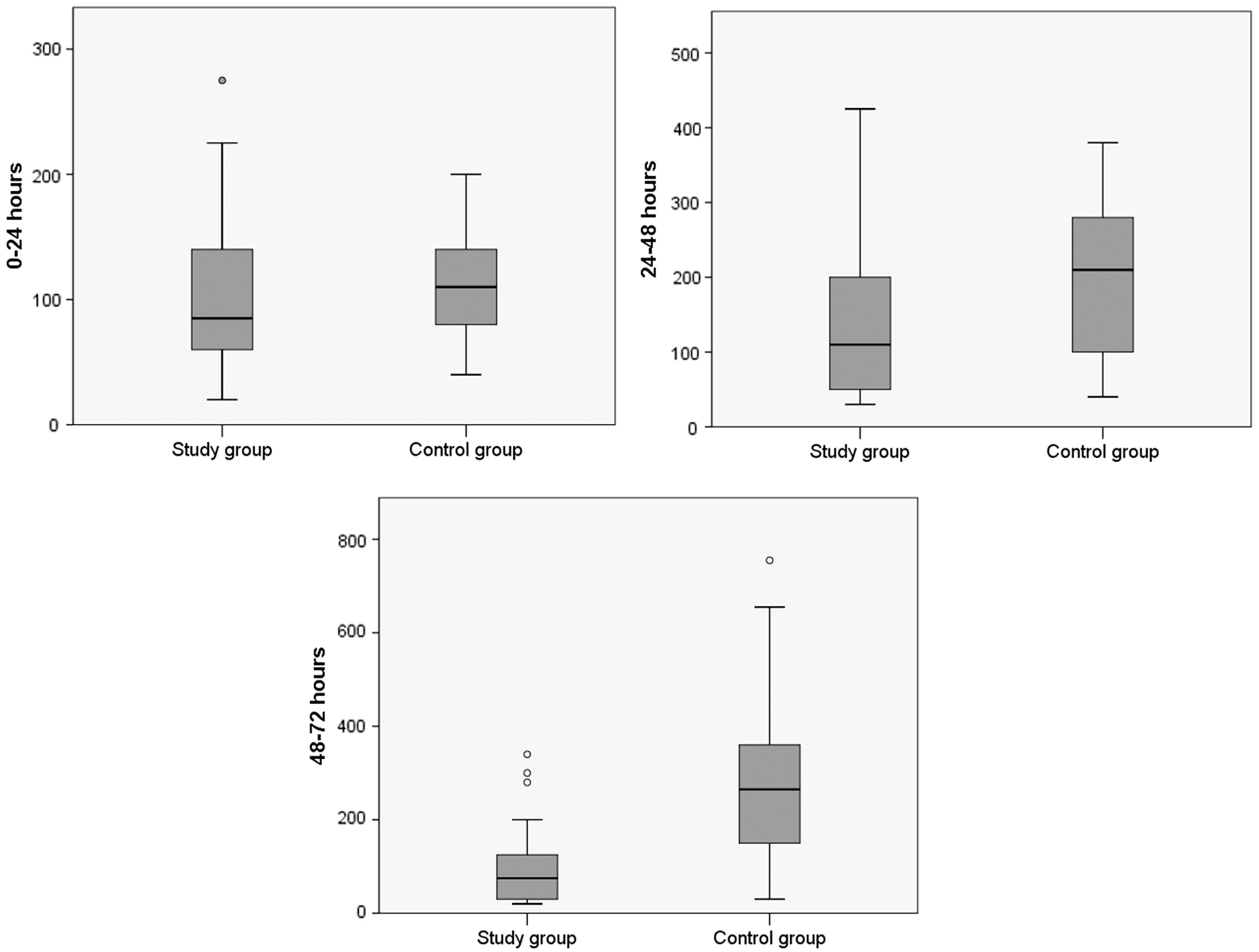
Comparison of postoperative drainage volumes between study and control groups.
Median ± IQR Daily and Total Drainage Volume in Patients Treated with Autologous Fibrin Glue Versus Control Group
Lymphocele was developed in 7 (20%) and 15 (37.5%) patients in study and control groups, respectively (p = 0.112). One patient in control group developed symptomatic lymphocele with pelvic pain and eventually percutaneous aspiration required. Other patients with asymptomatic lymphocele needed no further intervention. None of the patients have developed symptomatic lymphocele in study group. No adverse effects (allergic reactions, drain tube obstruction, etc.) or complications were noted in study group because of fibrin glue application.
Discussion
Pelvic lymphadenectomy has highlighted as the essential step for optimizing and risk assessment in prostate cancer surgery. 14 Technically challenging steps of the pelvic dissection facilitated with 3D vision and dexterity features of the robotic platform even in more complicated cases. In contrast, pelvic dissection area boundaries for LN involvement historically were the topic on debate. 15 Several nomograms were published to assess and predict preoperative nodal involvement risk. 12,16,17 European Association of Urology (EAU) and National Comprehensive Cancer Network (NCCN) guidelines recommend pelvic LN dissection based on specific cutoff values (5% and 2% involvement risk) according to nomograms, 18,19 whereas American Urological Association considers PLND for patients with high risk involvement without cutoff value. 20 EAU and NCCN guidelines also recommend that PLND should include extended dissection areas for accurate nodal staging.
Despite known beneficial effects, ePLND can lead to several complications related to prolonged lymphatic drainage and lymphocele formation, which in turn can translate to impairment of quality of life and may raise costs because of additional diagnostic tests, and rarely surgical intervention. 21 Several techniques, such as transperitoneal approach, ligation of lymphatic tissues, and bipolar cautery of small lymphatic vessels, have been suggested to prevent lymph leakage. 22 However, these methods cannot adequately reduce the drainage and prevent lymphocele formation in all patients. Before designing this study, we thought that fibrin glue could be used where conventional methods would not adequately decrease lymphatic leakage. After monitoring the significant decrease in postoperative drainage output in study group, we continued steady application of fibrin glue in consecutive patients.
Several techniques such as transperitoneal approach or peritonectomy during extraperitoneal RARP have been studied for prevention of lymphocele. 23 Absorptive feature of peritoneal surface allows lymphatic fluids to re-enter into the circulation. Transperitoneal approach can facilitate lymphatic fluid absorption with a large peritoneal surface, and thereby reduces lymphocele development. Interestingly, in a study published by Horovitz and colleagues, authors found no difference in the rate of symptomatic lymphocele development in a large series of patients undergoing extra-(2.83%) and transperitoneal (1.49%) RARP (p = 0.09). 6 Possible reason for this phenomena may be explained by sealing off pelvic dissection area from peritoneal cavity and trapping lymphatic fluids after adhering the PLND bed with perivesical fat during a transperitoneal RARP, which was described by Lebeis and colleagues. 24
Several studies evaluated effectiveness of hemostatic agents for decreasing drainage and lymphocele formation in urology field. Simonato and colleagues showed that TachoSil (equine collagen patch; coated with human fibrinogen and thrombin) effectively reduced drainage amount, and also lymphocele development in prostate cancer patients who underwent open retropubic prostatectomy. 7 In another study, Waldert and colleagues reported efficacy of FloSeal® (bovine-derived gelous matrix mixed with human thrombin) for symptomatic lymphocele prevention in laparoscopic transperitoneal RP series. 25 Both of these studies were similar to this study aiming to decrease lymphatic drainage and lymphocele formation by sealing damaged lymphatic vessels with hemostatic agents. However, in our study we preferred to use patient's own blood-derived autologous fibrin solution. Autologous fibrin glue solution carries zero risk of bacterial or viral contaminating (hepatitis B and C, HIV, etc.) and allergic reactions as it is derived from patient's own blood.
In our study, lymphatic drainage started on postoperative day 2. There was not a difference between the groups during the 1st day of operation, which likely accounts mostly of perioperative irrigation fluids. Drainage volume was reduced by 50% (110 mL vs 210 mL) and 75% (70 mL vs 270 mL) in study group than control group at postoperative 2nd and 3rd days, respectively (Table 2 and Fig. 2). The total drainage volume was also 50% reduced in study group (277 mL vs 577 mL). In contrast, lymphocele formation rate in study group was twofold lower than control group (n = 7 vs n = 15), although it was not statistically significant probably because of small number of lymphoceles developed patients (p = 0.112). Moreover, none of the patients developed symptomatic lymphocele in study group. Several studies assessed the complications related to increased drainage amount after PLND, but only few studies focused on lymphorrhea. 26,27 Capitanio and colleagues reported increased clinically significant lymphocele formation above the median amount of 615 mL lymphorrhea in their RRP series. 22 The authors also indicate the increased risk of lymphorrhea and lymphocele development with PLND extent in patients >65 years. In another study, Kim and colleagues evaluated the effectiveness of octreotide in patients with lymphatic drainage amount >200 mL at postoperative day 3 after PLND. 28 Authors report reduced lymphatic amount (205.7 mL vs 95.2 mL) along with early drain removal, shorter hospital stay, and lymphocele development. In this study, we have demonstrated intraoperative management of lymphorrhea using fibrin glue that may help clinicians during the treatment decision-making.
We believe that sealing of damaged small lymphatic vessels with microadhesive layer has a preventive effect for lymphatic flow. Comparing with previously operated control group patients, it seems clear that bipolar cautery and clipping do not adequately seal the channels. Thereby, our goal was to create an additional microscopic fibrin barrier over the dissection areas. Considering the technical difficulty placing clips over the obturator and internal iliac plans, fibrin solution will create additional layer and reduce the lymphatic fluid coming from dissection bed.
Limitations of this study include relatively small number of patients and nonrandomized retrospective design. As the main goal of this study was to assess the postoperative drainage volume and fibrin glue contribution to drainage control, the cost-effectiveness was beyond the scope of this study. The cost of Vivostat fibrin glue kit is estimated 250€ in Turkey and has complete coverage by health insurance companies. The results of this study suggest that autologous fibrin glue can be used to manage prolonged postoperative drainage output after ePLND without adverse effects. We believe that fibrin glue application in addition to conservative methods may lower cost-effectiveness for the reasons outlined earlier, but it must be still validated in future series.
Conclusions
The results of this study suggest that autologous fibrin glue is an effective and safe method that can reduce postoperative lymphatic drainage, and also lymphocele formation after extended pelvic lymph node dissection in robot-assisted radical prostatectomy operation. Furthermore, our preliminary results showed that this technique may be applicable in addition to conventional methods for lymphatic control. Additional studies are needed to validate the results of our study.
Footnotes
Author Disclosure Statement
No competing financial interests exist.