
Abstract
Objective:
To conduct a prospective randomized trial to evaluate the efficacy of a novel prophylactic procedure for inguinal hernia (IH) after transperitoneal robot-assisted radical prostatectomy (RARP).
Methods:
The prophylactic procedure for IH after RARP involved the dissection of the peritoneum ∼5 cm outward from internal inguinal ring (IIR), separating the spermatic cord and vessels from the peritoneum. This was randomly performed on one side (left or right).
Results:
A total of 148 cases were included, and IH after RARP was observed in 19 (12.8%) cases, with 11 (7.4%) cases in the right side only, 3 (2.0%) in the left side only, and 5 (3.4%) bilaterally. IHs developed in 9 (6.1%) sides that underwent prophylactic procedure and in 15 (10.1%) that did not. Kaplan–Meier curve analysis revealed no significant difference between the preventive and nonpreventive sides (p = 0.197). Based on the observation during laparoscopic hernioplasty, the prophylactic procedure that strengthened the abdominal wall was by adhesion conglutination of the exfoliated peritoneum in the effective side, and IIRs were opened and developed IH in the ineffective sides. Predictive factors for IH after RARP were not found using Cox proportional hazard model.
Conclusion:
The preventive procedure for IH used in this study reduced the incidence of IH after RARP, but the difference was not significant.
Introduction
Radical prostatectomy (RP) is a standard treatment for localized prostate cancer, and inguinal hernia (IH) is a clinically important complication after RP. A meta-analysis reported that the incidence of IH after open radical prostatectomy (ORP) was 15.9%, and most IH cases occurred within the first 2 years after RP. 1 The mechanism of IH after RP remains unclear. After minimally invasive laparoscopic radical prostatectomy (LRP) and robot-assisted radical prostatectomy (RARP), the incidence of IH was reported to be lower than that after ORP but higher than that of control without operation. 2,3 As a prophylactic procedure for IH after RP, the transection of the patent processus vaginalis (PPV) during operation 4 and releasing the spermatic cord from the peritoneum 5 were reported to reduce the incidence of IH after ORP. However, the evidence level of ORP was not high in these reports because of the historical control for comparison. As a prospective randomized trial of prophylactic intervention for IH after ORP, a nonresorbable figure-eight suture placed lateral to the internal ring of the inguinal canal and spermatic cord could substantially reduce the incidence. 6 Alternatively, there were few reports of a prophylactic procedure for IH after RP through a transperitoneal laparoscopic approach, including RARP, without using artificial materials. 7
In this study, a prospective randomized controlled trial (RCT) of a prophylactic procedure for IH after transperitoneal RARP was designed and its effectiveness was evaluated. The prophylactic procedure was randomly performed for one side (left or right) and compared with intra-abdominal findings after laparoscopic hernioplasty after incidence of IH.
Methods
Inclusion criterion in the study was patients with localized prostate cancer scheduled to undergo RARP at the Kanazawa University Hospital. Patients with a history of IH repair or clinical IH on preoperative physical examination were excluded. All IH prevention procedures were performed by YK or two other surgeons under the observation of YK. RARP was performed using a standard six-port transperitoneal approach at 12 mm Hg insufflation pressure, and the transection between the bladder neck and prostate was performed using an anterior approach.
Based on intra-abdominal observation during laparoscopic hernioplasty in our hospital, scar contraction of the intra-abdominal wall at the Hesselbach's triangle, which is a triangular area on the inferior interior aspect of the anterior abdominal wall within the groin, weakened the area around internal inguinal ring (IIR), which is located outside the Hesselbach's triangle. Subsequently, IH developed. Therefore, we designed a new prophylactic procedure for IH after RARP to dissect the peritoneum from the abdominal wall outside of the spermatic cord near IIR; thereby, the dissected peritoneum conglutinating to the area outside of IIR would reinforce the area of the abdominal wall. In this procedure, the peritoneum was dissected ∼5 cm outward from IIR. As a result, the spermatic cord and vessels were separated from the peritoneum (Fig. 1). In patients with PPV, PPV was dissected along the peritoneal inguinal canal and transected with coagulation at the middle of PPV.
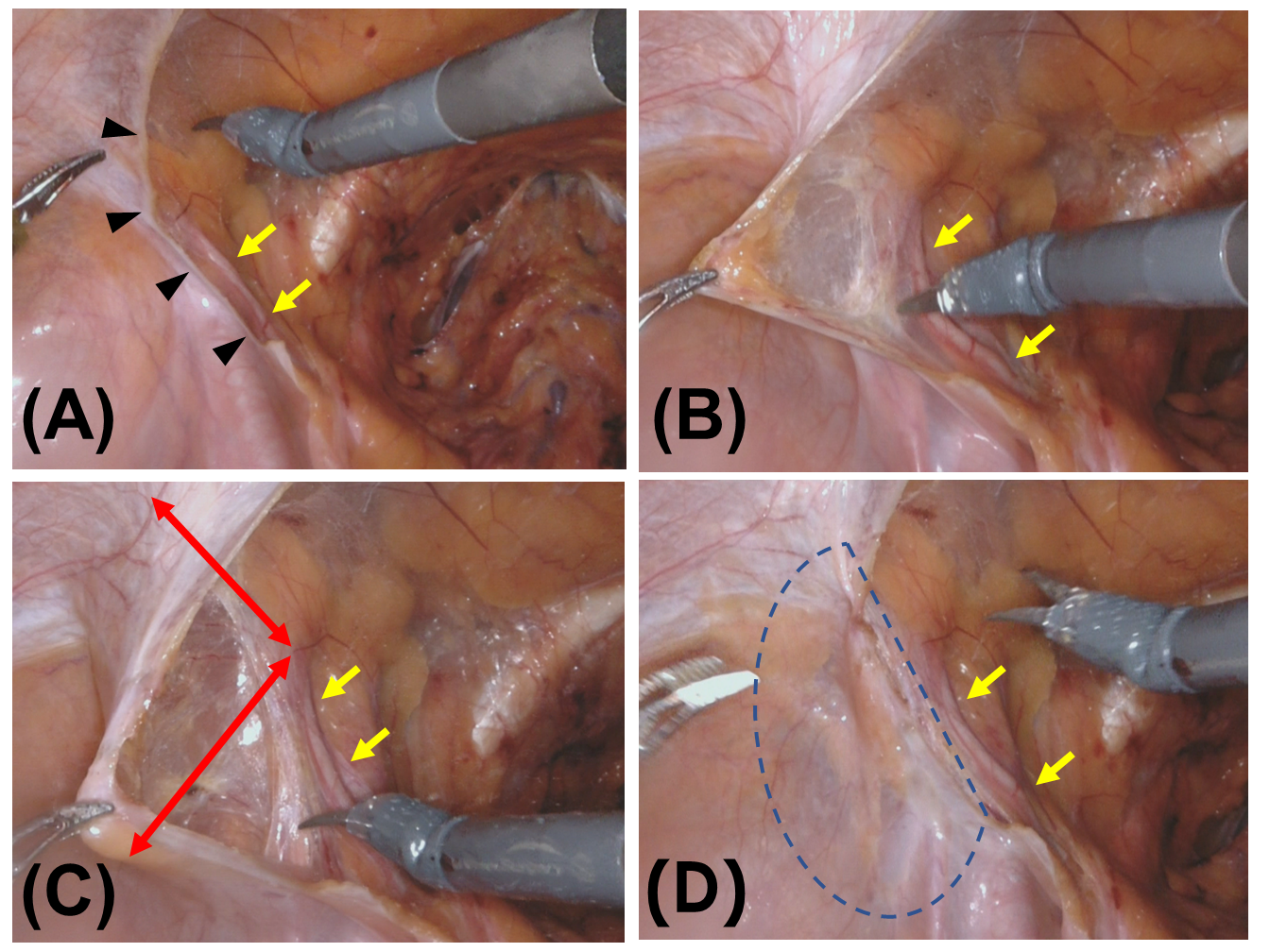
Preventive procedure for inguinal hernia after robot-assisted radical prostatectomy is shown.
Patients were randomized in two groups (using
Relationships among demographic data were assessed using chi-squared test for categorical valuables and independent t-test for continuous valuables. Patients were followed up until IH development or until they withdrew from the study. Cumulative incidence of IH for the intervention side over time was compared with that for the control side using Kaplan–Meier method. Differences among groups were assessed using log-rank tests. The influence of clinical variables that affected prognosis was evaluated using Cox's proportional hazard regression model. All data analyses were conducted using SPSS for Windows (SPSS, Inc., Chicago, IL), with p < 0.05 considered statistically significant.
Results
During the recruitment period from September 2012 to January 2016, 170 patients who met the inclusion criterion in consecutive 183 RARP cases were offered participation in this study. Informed consent was obtained from 154 patients; 6 of these 154 patients with no clinical IH had obvious IH during operation and were excluded. Thus, a total of 148 patients were included, of whom 74 underwent the prophylactic procedure on the right side and 74 on the left side. Our prevention procedure required approximately two additional minutes, and adverse events arising from the procedure were not observed. Clinical characteristics of patients of each group are shown in Table 1. There were no statistically significant differences between the groups in terms of clinical characteristics. During the average follow-up period of 49.4 months, IH after RARP was observed in a total of 19 (12.8%) cases, with 11 (7.4%) on the right side, 3 (2.0%) on the left side, and 5 (3.4%) bilaterally. In all 148 cases, 9 sides (6.1%) that underwent the prophylactic procedure and 15 (10.1%) that did not undergo the procedure developed IH. PPV was observed in 22 (14.9%) cases on the right side, 11 (7.4%) on the left side, and 10 (6.7%) bilaterally. The Kaplan–Meier curve revealed no significant difference between the preventive and nonpreventive sides (Fig. 2). Based on the observation during laparoscopic hernioplasty around IIR with the prophylactic procedure, the abdominal wall was strengthened by adhesion conglutination of the exfoliated peritoneum with the prophylactic procedure on the effective side, and IIR was opened and developed IH on the ineffective sides as in cases without the prophylactic procedure (Fig. 3A, B). Predictive factors for IH after RARP were not found using Cox proportional hazard model (Table 2).

Kaplan–Meier method showing rates of no inguinal hernia after robot-assisted radical prostatectomy with or without preventive procedure for inguinal hernia.

Laparoscopic view of
Characteristics of the Study Population
BMI = body mass index; EPE = extracapsular extension; ICIQ-SF = International Consultation on Incontinence Questionnaire-Short Form; IPSS = International Prostate Symptom Score; LND = lymph node dissection; NADT = neoadjuvant androgen deprivation therapy; PSA = prostate-specific antigen; QOL = quality of life; RM = resection margin; SD = standard deviation.
Univariate and Multivariate Cox Proportional Hazards Regression Models Predicting Inguinal Hernia After Robot-Assisted Radical Prostatectomy
CI = confidence interval; HR = hazard ratio; PPV = patent processus vaginalis.
Discussion
IH after RP is a clinically important complication, and several effective prophylactic procedures for IH after ORP have been reported. 3 –5,8 The incidence of IH after RARP is lesser than after ORP. 3 However, there are no reports stating a clearly effective prophylactic procedure for IH after RARP.
The incidence of IH after various operations has been reported. Lodding and colleagues 9 have reported that the incidence of IH after ORP plus pelvic lymph node dissection (PLND), PLND only, and no surgery was 13.6%, 7.6%, and 3.1%, respectively. Ichioka and colleagues 10 reported that the incidence of IH after ORP, PLND, and cystectomy was 21.3%, 11.4%, and 5.4%, respectively. They determined that injury to the transversalis fascia was related to the incidence of IH after ORP. Abe and colleagues 2 have reported that the incidence of IH after ORP, conventional LRP, and radiotherapy was 17%, 14%, and 1.4%, respectively. Stranne and colleagues 3 have reported that the incidence of IH after RARP was 5.8%, which was higher than that of 2.6% found in the control group with no surgery. The incidence of IH after perineal RP was reported to be 1.8%. 11 In another study, 12 the incidence of IH after Retzius-sparing robot-assisted radical prostatectomy (RS-RARP) was 3.69% and that after conventional RARP was 7.76%, which are lower than rates reported after other approaches of RP; however, in that study, the incidence of IH was not compared with rate in a control group that did not undergo RP. The mechanism of development of IH after RP remains unclear; however, several hypotheses have been reported. Shimbo and colleagues 7 hypothesized that the peritoneum and vas deferens were stretched after vesicourethral anastomosis, resulting in medial shifting of the internal ring, thereby facilitating IH. It was unclear whether the vas deferens transected at the proximal side of ampulla of the vas deferens in RP was actually stretched; however, it could be possible to stretch the vas deferens through repositioning of the adhered peritoneum after vesicourethral anastomosis.
Based on previous reports, the speculated mechanism of IH after RP is as follows: an anatomical change caused by adhesion after each lower abdominal incision, opening of the Retzius space, and vesicourethral anastomosis accompanied by prostate removal would contribute to the development of IH. Peripheral shifting of IIR area caused by adhesion after the opening of the Retzius space and vesicourethral anastomosis would contribute to the development of IH, and medial shifting of IIR area caused by adhesion after lower abdominal incision would also contribute to the development of IH because the incidence of IH after PLND and cystectomy with lower abdominal incision was reported to increase. 9,11 In perineal RP and RS-RARP, IH caused by peripheral shifting of inguinal area would not occur even after vesicourethral anastomosis because relocated adhesion did not develop without the opening of the Retzius space. Based on intra-abdominal observation during laparoscopic hernioplasty in our hospital, scar contraction of the intra-abdominal wall at the Hesselbach's triangle and the opening of IIR developed at the internal inguinal area. These findings would support our speculations. Therefore, we designed a new prophylactic procedure for IH after RARP to dissect the peritoneum from the abdominal wall outside of the spermatic cord near IIR; thereby, the dissected peritoneum adhering to the area around outside of IIR would reinforce the area of the abdominal wall.
An RCT was designed to evaluate the efficacy of this prophylactic procedure for IH after RARP. To the best of our knowledge, this trial is the first RCT studying the effectiveness of prophylactic procedure for IH after RARP. In this study, the prophylactic procedure was randomly performed on the right or left side, thereby observing intra-abdominal findings of success and failure case of the prophylactic procedure during laparoscopic hernioplasty. In successful cases, peritoneal adhesion would occur outside the area of IIR and strengthen the abdominal wall as predicted (Fig. 2B). However, in cases of the development of IH despite performing the prophylactic procedure, the inner side of IIR shifted inward owing to its shifting to the adhered area, consequently opening or weakening IIR; IH developed because it tends to develop without the prophylactic procedure (Fig. 3B). We could not identify effective cases with prophylactic procedure and predictive factors.
In this study, our prophylactic procedure for IH after RARP contributed to reducing the incidence to approximately one-half of that in cases without the prophylactic procedure; however, the difference was not statistically significant. Therefore, our prophylactic procedure was inadequate to prevent IH after RARP. In contrast, prevention techniques for IH after retroperitoneal RP have been reported to be effective because a separated peritoneum would adhere to the pelvic wall between transected processus vaginalis. 4,5,8 The procedure would strengthen the IIR area. However, the same procedure will not be effective in preventing IH after transperitoneal RARP because the peritoneum dissected at the IIR area in transperitoneal RARP would shift inward, making it incapable of appropriately adhering to the pelvic wall to strengthen the IIR area. In an effective prophylactic procedure for IH after RARP, Lee and colleagues 12 reported plugging hemostatic agents into the end of canal incised and dissected between the lateral side of the internal inguinal floor and processus vaginalis for patients with PPV during RARP. However, this method was only applicable for patients with PPV. Concomitant repairs of IH using mesh placement during RARP using either transperitoneal or extraperitoneal approach to existing IH were effective and safe, despite the longer duration of the operative time. 13 –15
It may be desirable to perform preventive procedure for postoperative IH during RARP without using artificial devices to avoid any difficulty after RARP because of the low incidence of IH after RARP originally, although preventive procedures using artificial devices were reported to be safe. Shimbo and colleagues 7 reported an effective preventive procedure for IH after transperitoneal RARP. The procedure was similar to our procedure; however, our procedure was to dissect the peritoneum outside of the vas deferens from the lateral abdominal wall. This was unlike Shimbo's method in which the vas deferens was separated toward the inside ∼5-cm long, and the vas deferens was cut in some cases. In their report, the mean observation period of the preventive group was 14 months, which was significantly shorter than that of the historical control group. However, IH after preventive procedure occurred in several cases, even in such a short observation period. 7 Further investigation would be needed to confirm the effectiveness of this preventive procedure.
Patient-dependent risk factors for developing IH are male sex, old age, the presence of PPV, and low body mass index (BMI). 16 As for the laterality of the incidence of IH, right side dominance after RP was reported. 1 In our investigation of risk factors for IH after RARP using multivariate Cox regression analysis, right side groin, low BMI, and the presence of PPV showed a tendency for a high incidence of IH after RARP; however, the difference was not statistically significant. High intra-abdominal pressure is also a risk factor. 16 In patients with a high International Prostate Symptom Score (IPSS) before RARP, the incidence of IH after RARP is significantly higher 17 ; however, in our cohort, IPSS either before or after RARP was not a significant predictor of IH after RARP (Table 2). Urinary straining contributing to IH after RP was reported 18 ; however, straining scores (IPSS question 6) were not significantly different between the IH and non-IH groups in our study.
RARP was usually transperitoneally performed because of the large working space; however, the lower incidence of IH after perineal RP 19 and RS-RARP 20 has been reported. For the prevention of IH after RP, these approaches would be desirable. Kurokawa and colleagues 21 reported a low incidence of IH after RARP using an extraperitoneal approach with preventive procedure of postoperative IH; therefore, this method would be a choice for the prevention of postoperative IH.
This study has some limitations. The real incidence of IH after RARP with preventive procedure was higher than that expected before RCT, and the incidence without preventive procedure was lower than that expected; therefore, the necessary number of trial cases for statistically sufficient power may be lower than our estimation. However, the incidence of IH after RARP with preventive procedure was not sufficiently low in our study, and our preventive procedure would be insufficient for the prevention of IH. During RARP, scissors were used with the right hand; therefore, the preventive procedure may not be completely the same on the right and left sides because of the angle of scissors. There was a higher probability of IH after right side procedure than after the left side procedure 1 ; however, the higher probability of IH on the right side in our study could be caused by the slight difference in the preventive procedure between the right and left sides.
Conclusion
The preventive procedure for IH used in this study reduced the incidence of IH after RARP, but the difference was not significant.
Footnotes
Author Disclosure Statement
No competing financial interests exist.