
Abstract
Introduction:
Public awareness regarding the influence of diet on kidney stones is unknown. We sought to evaluate such perceptions among an unselected community cohort.
Materials and Methods:
A survey was created to assess perception of beverages/foods on risk of kidney stone formation. Surveys were distributed to attendees of a State Fair. Participants were categorized to determine the effect of stone history on prevention knowledge (no prior stone vs prior stone).
Results:
Seven hundred fifty-three participants completed the survey, including 264 (35%) with a prior stone. Participants with prior stones were less likely to believe stones were preventable compared to those without (56% vs 65%, p = 0.01). Appropriate perceptions regarding influence of diet on stones were highest for water (>90% of participants) and cola/salt/red meat (>50%). Fewer than half of respondents correctly identified the influence of the remaining 14 substances. On multivariable analysis, stone formers were more likely to correctly identify the influence of lemonade (odds ratio [OR] 2.09; 95% confidence interval [CI] 1.32–3.31), nuts (OR 2.60; 95% CI 1.60–4.23), and spinach (OR 5.06; 95% CI 2.89–8.86), but less likely to identify the influence of coffee (OR 0.43; 95% CI 0.23–0.82) and red meat (OR 0.52; 95% CI 0.23–0.59).
Conclusion:
Patients with prior stones hold different attitudes regarding the influence of certain foods and drinks on stone formation relative to the public. Such attitudes are not always correct, and as a group they are less likely to believe in dietary stone prevention. Such findings may indicate confusion among stone formers and highlight an opportunity for improved dietary counseling.
Introduction
Recent epidemiologic data report the prevalence of kidney stone disease in the United States to be ∼11% in men and 7% in women. 1 This is a considerable increase; nearly double to what it was 20 years ago. 1 A number of factors have been linked to increasing rates of stone disease. Notably, changing dietary habits with subsequent increases in corresponding medical conditions such as obesity, diabetes, and hypertension have been shown to be a contributor. 2,3
There is increasing recognition that preventative efforts to combat rising rates of stone disease are sorely needed. 4 Current practice guidelines 5 advocate dietary evaluations and counseling as a standard part of kidney stone management, and prior studies 6 have demonstrated that adherence to stone prevention recommendations can lead to substantial clinical benefits and health care savings. However, dietary counseling for kidney stones can be complex, and the treating clinician is most commonly the person responsible for this process.
One of the most fundamentally important considerations in providing effective dietary counseling for stone prevention is first understanding how much baseline familiarity and knowledge patients have regarding the link between diet and stone formation. This is particularly true as many patients may have misconceptions regarding potential associations that may need to first be broken before implementing better dietary plans. 7 To date, there have been no studies that have formally evaluated public awareness regarding kidney stone prevention or public perceptions of dietary contributions to stone formation and prevention. We sought to characterize public perceptions regarding associations between diet and stone formation among a large community based cohort in an effort to improve counseling on dietary stone prevention.
Materials and Methods
Study population
A survey was administered to a convenience sample of voluntary participants over a 4-day period at the 2017 Minnesota State Fair through the University of Minnesota Driven to Discover (D2D) Research Facility. 8 This facility is a freestanding structure on the fairgrounds that supports University associated research studies and draws attendees as they pass. The Minnesota State Fair attracts roughly 2 million visitors per year with visitor demographics roughly representing the state as a whole and the greater Midwestern United States. 9 The study was approved by the Institutional Review Board at the University of Minnesota before data collection (Study No. 00000327). All participants were self-identified and approached the research booth where they were confirmed to meet eligibility criteria before participating. Eligibility criteria were adults 18 years of age or older who were able to provide consent and read English. Recruitment occurred during four separate 8-hour sessions. During the first two sessions, surveys were handed out to all interested participants regardless of stone history. To draw a sufficient comparison group, during the second two sessions a prior history of stones was required as eligibility criteria. Participants were eligible to receive either a tote bag or enter a prize drawing for a mobile health tracker valued at $55.
Survey design
The survey was designed to capture participant data, demographics, and attitudes toward the association between foods and beverages and stone risk. As there were no previously validated surveys for this purpose, a new questionnaire was created in-house. Standard Likert scales were utilized for questions with subjective responses. 10 The survey was distributed to participants on mobile electronic tablets (iPad®) using Research Electronic Data Capture (REDCap) software. 11
Standard information regarding demographics and past medical history was obtained from all participants. Participants were asked about attitudes toward stone prevention as it related to medications, foods, and beverages. Those who responded that diet was associated with stone risk were subsequently asked to classify various foods and beverages by their influence on promoting stone growth. American Urological Association (AUA) guidelines on medical management of stones and previous literature were used where applicable to categorize each substance (see Supplementary Fig. S1 for specific citations). Subjects were asked to classify dietary substances as stone favorable (prevents stones), stone unfavorable (leads to stone formation), or neutral.
Additional questions were designed to assess the respondents' history of stone disease and management and determine risk status as to whether a metabolic evaluation was indicated. For the purposes of this study, “high risk” was defined using AUA guidelines 5,12 as follows: recurrent stones, family history of stones, as well as stones in the context of specified medical comorbidities, solitary kidney, and “high risk” vocation (i.e., pilot). Report of prior 24-hour urine collection test was used as a surrogate measure for having previously undergone a metabolic evaluation.
Statistical analysis
Respondents were first categorized as either stone formers or nonstone formers. Stone formers were later recategorized by treatment intensity (surgically managed stone vs conservatively managed stone). Data analysis was performed in R (version 3.4; R Foundation for Statistical Computing, Vienna, Austria). Continuous variables were reported as means if normally distributed or medians if not and compared with student's T or Wilcoxon/Kruskal–Wallis tests, respectively. Categorical variables were reported as frequencies and compared with chi square (χ2). Multivariate logistic regression analyses were conducted using gender, age, minority status, education, insurance, and treatment intensity to characterize predictors of guideline knowledge and receiving a metabolic work-up. All p-values were two sided, and statistical significance was set at 0.05.
Results
Demographics
A total of 753 participants completed the survey. Thirty-five percent reported a history of prior stones, including 99 who had undergone prior procedures (13.1%) and 165 who had not (21.9%) (Table 1). On average, participants with a history of stone disease were statistically more likely to be white, male, greater than age 50, and insured (p < 0.01). Education level was not statistically different between those with a history of stones and those without.
Demographics of Study Participants
SE = standard error.
General beliefs about kidney stone prevention
Stone formers were significantly less likely than nonstone formers to believe that kidney stones were preventable (Fig. 1). A minority of patients believed that medications can be used to prevent kidney stones with fewer than one third of those with prior stones agreeing to this statement compared to nearly half of the nonstone formers. In addition, these beliefs were amplified with increasing stone treatment exposure. Respondents who had undergone procedures for stone removal were less likely to believe that stones were preventable than those who were treatment naive or who had never had a stone. There were no significant differences between the three groups on the subject of food or beverage involvement with stone prevention with a majority of respondents agreeing that foods and beverages have a role in kidney stone formation.
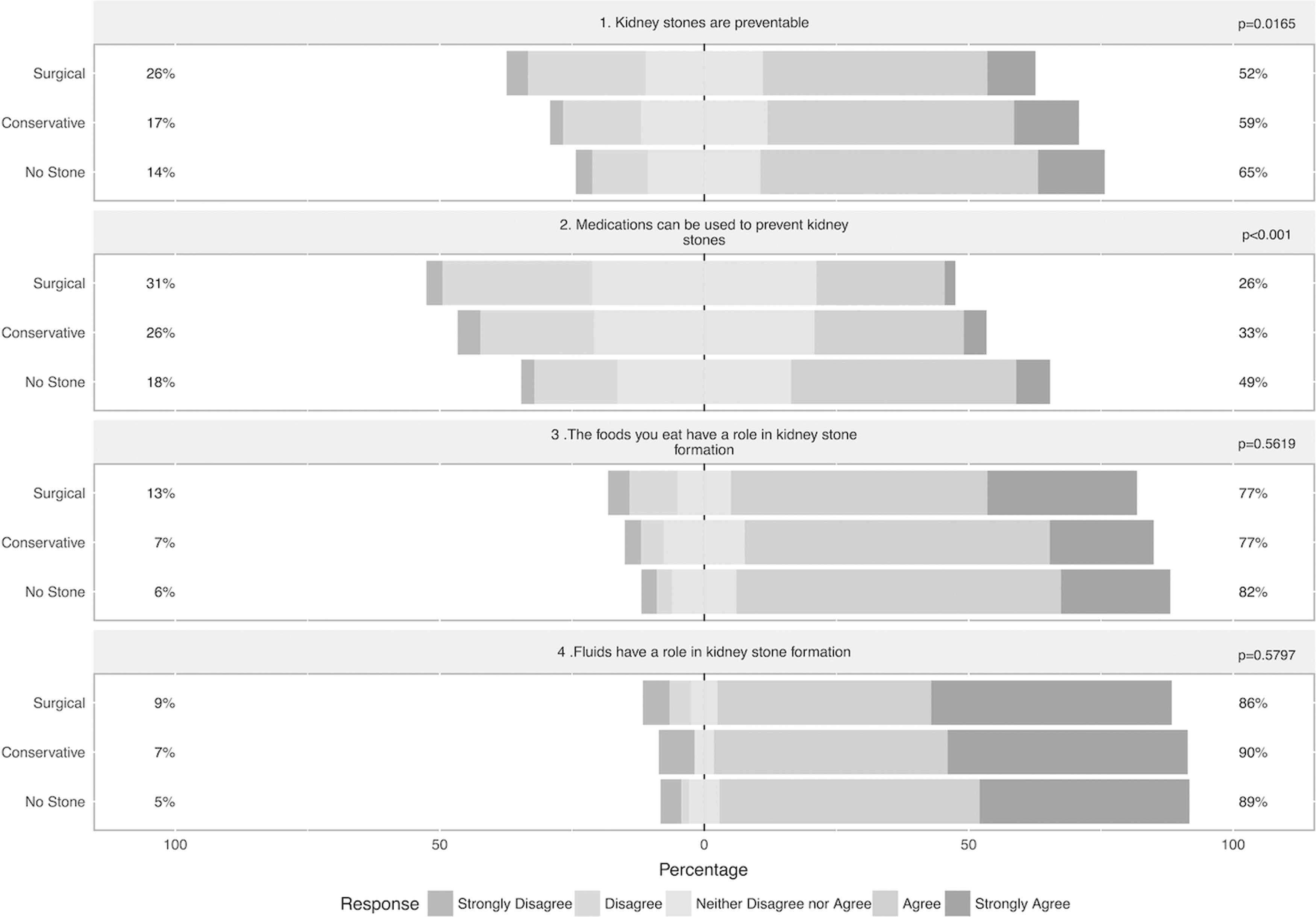
Participants rated their feelings on a 5-point Likert scale on preventability of kidney stones in general and the relationship between medications, foods, and fluids in regards to stone preventability. Percentages to the right of the figure indicate percent of respondents who responded either agree or strongly agree. Percentages on the left indicate those who responded either disagree or strongly disagree.
Perceptions of foods and beverages
There was wide variation in regards to the perception of nine foods and nine beverages on stone risk (Fig. 2). Water was the item with the most accurate perceptions among the cohort with over 90% of all respondents appropriately identifying it as a stone favorable dietary item. Salt was similarly identified appropriately by the majority of respondents, although as a stone unfavorable item. Fruit punch, dark cola, and red meat were the only other items where an appropriate association with stone risk was identified by greater than 50% of the overall cohort.

Percentage of each group with guideline-appropriate perception regarding influence of favorable and unfavorable beverages
Fewer than half of the study population appropriately identified the influence of the remaining 13 dietary items on stone risk. There were, however, differences in the way stone formers perceived the influence of some of these items compared to nonstone formers. For example, high oxalate foods, including nuts, spinach, beets, and rhubarb, were more likely to be identified as stone unfavorable among those with a stone history compared to those without a history of stones (Fig. 2). Stone formers were also more likely to appropriately identify lemonade as stone favorable. In some instances, stone formers were less likely to hold appropriate perceptions as was evident with tea, coffee, dark cola, and fruit punch. There was no difference in perceptions of the remaining dietary items on stone risk between groups (wine, beer, clear soda, chocolate, peanut butter, and potatoes).
A multivariate analysis was performed to determine the likelihood of correct dietary perceptions when subject responses were controlled for demographic factors (age, gender, ethnicity, and insurance) and education level (Table 2). Those with a history of surgically treated stones were significantly more likely to have correct perceptions of the influence of several high oxalate foods (chocolate, beets, nuts, and spinach), as well as lemonade and beer. However, they were also significantly less likely to identify coffee, tea, and red meats with regards to their influence on stone formation.
Multivariate Analysis Controlling for Demographic Factors and Education
p < 0.05.
Bold = stone favorable; CI = confidence interval; italic = stone unfavorable; OR = odds ratio.
Metabolic work-up
Based on survey responses, 240 (32%) of the participants met AUA guideline criteria for consideration of metabolic work-up. Of those, only 95 (39.6%) indicated that they had previously undergone work-up. In those whom work-up was indicated and performed, having seen a urologist greatly improved the likelihood of having undergone metabolic work-up (odds ratio 16.71; 95% confidence interval 8.95–31.19; p < 0.001) compared to those who had not seen a urologist.
Discussion
Changes in dietary habits have been theorized to be one of the main contributing factors to the rapid rise in the incidence of kidney stones over recent years. 2 Dietary evaluation and counseling is considered a cornerstone of stone management 5 yet there are no real-world data to quantify baseline levels of knowledge held by patients when they come in for first time counseling. Our findings among a large community cohort demonstrate that baseline knowledge regarding the relationship between most foods and beverages on stone risk is low and several misconceptions exist, highlighting an opportunity for targeted efforts to improve dietary counseling as part of care pathways for patients with kidney stones.
One unexpected finding of our analysis was the fact that respondents with a stone history were significantly less likely to believe that stones could be prevented and that medications could be used to prevent stone recurrences than those without a history of stones. The reason for this is unclear. It could indicate some frustration at the patient level related to high stone recurrence rates, particularly as beliefs in preventative efforts became worse with increased treatment intensity. It also may be indicative of inadequate counseling. Regardless, it would seem to signal a growth opportunity at all levels of clinical care to raise awareness about stone prevention.
In regard to perceptions between dietary items and stone risk, we suspect that responses were heavily influenced by generally held notions regarding certain foods as “healthy” or “unhealthy.” In some instances these general categorizations can be appropriately applied toward kidney stone risk as in the case of certain foods such as water, cola, fruit punch, salt, and red meat. Indeed, prior studies have demonstrated cola and red meat to be among the most commonly “vilified” foods, while water is almost universally seen as healthy. 13,14 However, in certain cases a food that is generally believed to be “healthy” may in fact be an unfavorable food from a stone risk perspective, as may be true in foods with high oxalate contents. Spinach, for example, is known to be a high oxalate containing food, yet is commonly perceived as healthy. This misconception was more common among nonstone formers (80%) but it is worth noting that over half of the prior stone formers miscategorized the influence of spinach on stone risk as well. Similar misconceptions were demonstrated for the other high oxalate foods as well (nuts, spinach, beets, and rhubarb) (Fig. 3). These findings highlight the fact that when providing dietary counseling on stones, many patients are likely to come in with misconceptions that must be broken.

Percentage of respondents responding “good for stones” (decreases stone formation) for high oxalate-containing foods.
Two particularly interesting dietary substances worth mention are red meat and coffee. In each case there appeared to be a worse awareness regarding influence on stone risk among those with a history of stones compared to those without. It is not clear how or why stone history would decrease dietary knowledge for these two substances. Those with a history of stones did perform significantly better with regards to some commonly counseled substances (lemonade, spinach, and nuts). This effect is even greater among those who have had previous stone surgeries, yet still quite low overall. We suspect that this small increase in knowledge is due to greater exposure to opportunities for dietary counseling.
Finally, the participants were examined for rates of metabolic stone work-ups in accordance with guideline recommendations. Approximately 40% reported previously undergoing at least one metabolic work-up, which is significantly higher than previously reported estimates of <10% of qualified stone formers. While these results are encouraging, the expected knowledge benefits from this intervention were not readily apparent in our survey results. In addition, our data suggest that urologists are more likely to be ordering these metabolic work-ups compared to other physicians. Therefore the best opportunity for improving educational efforts may be centered in the urologist's office.
We recognize several limitations to our study. First, our survey is not currently validated, and as such there is risk of introduction of measurement bias in our sample. Any survey-based study is also suspect to some degree of response error (e.g., 13 respondents who endorsed previous stone surgery also reported having never seen a urologist prior—an unlikely finding). Second, it is conceivable that we presented an overly simplistic categorization of food being “good” or “bad” when the truth is invariably more complex. However, research suggests that individuals invariably categorize food according to a good–bad dichotomy and that this simplified approach may be most effective for counseling purposes. 15
We also acknowledge that the evidence between dietary consumption and stone risk is certainly stronger for some foods/beverages than others; however, all of the included dietary selections were mentioned in the AUA guidelines. In some cases, survey selections may have altered outcomes. For example, we used red meat as a surrogate for animal protein when in fact attitudes may potentially differ among poultry, fish, and red meat. There are also substances not included in this survey that may be of interest for future study—perception of dairy items, as well as certain uniquely high salt-containing foods such as canned soup, would be interesting.
Another potential limitation is the potential for geographical bias given that our participants were all from the Midwestern United States. However, the demographics among our respondents is quite similar to existing epidemiologic data on stone disease in the United States. 16 Finally, the dietary recommendations tested herein apply primarily to those with a history of calcium-based stones and are not as applicable to those with other stone types (i.e., Uric Acid or Struvite). However, since calcium stones make up ∼80% of all kidney stones, 17 these recommendations should apply to the majority of stone formers.
Our study also has several strengths. First, it is the only attempt, to our knowledge, to quantify public perceptions of diet in relation to stone disease. Our study population also benefits from recruitment outside of a medical setting, thus avoiding selection bias toward people actively seeking medical care. Another strength is the relatively large sample size with nearly 500 respondents who participated despite never having had a kidney stone.
Conclusion
We found that the general public demonstrates a poor baseline level of knowledge with regards to the influence of most foods/beverages on stone risk. Stone formers had only slightly increased levels of knowledge for select substances (and slightly worse for others). These results suggest that greater efforts are needed to slow the ever-increasing incidence of kidney stone disease. Our findings can be used to help build more effective and practical educational materials to help counsel patients with stones.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.