
Abstract
Introduction and Objectives:
The Moses effect (ME) was described >30 years ago during normal laser functioning in a fluid medium. Recently, a laser device equipped with a pulse-modulating system called Moses™ technology (MT; Lumenis®) was marketed for both stone lithotripsy and prostate endoscopic surgery. We aimed to perform a literature revision of ME from a historical perspective up until its present-day applications.
Evidence Acquisition:
A search of Medline, PubMed, and Scopus was performed to identify articles published in English within the past 30 years addressing both ME and MT in relation to their urologic applications. Relevant studies were then screened, and the data were extracted, analyzed, and summarized. The preferred reporting items for systematic reviews and meta-analysis criteria were applied.
Results:
ME was first described in 1986 during endovascular laser tissue ablation. During the late 1980s and the early 1990s, the interest raised around ME led to its characterization and better definition. Despite this initial interest, ME gradually disappeared from the focus of researchers and clinicians. In 2017, MT was launched on the market, although postmarketing comparative efficacy and safety data are lacking.
Conclusions:
Although ME had been described and characterized during normal laser functioning >30 years ago, only very recently it began to regain some consideration after the marketing of MT, whose clinical outcomes are still awaited.
Introduction
Since its first urologic application in 1992, 1 holmium:yttrium-aluminum-garnet (Ho:YAG) laser has become the main player among lasers currently used for lithotripsy, because of its effectiveness, versatility, and safety profile. 2 Despite the superiority of Ho:YAG laser, still considered the gold standard of endoscopic laser lithotripsy, 2 the need for a more efficient laser lithotripsy prompted research toward two main directives: the development of new laser sources and the improvement in energy delivery of Ho:YAG itself.
Urologic lasers work by definition immersed in a liquid fluid environment. This might entail both advantages and disadvantages. For instance, the laser beam energy, before reaching its target, will be partly delivered and, therefore, dispersed to the fluid. The effect of this profile of energy delivery has been known and enquired since >30 years. In particular, the formation of vapor cavities/bubbles at the tip of the laser through which the laser pulse may travel directly to its goal has raised considerable interest in the research community, and was named “Moses effect” (ME) for the first time in 1986. 3 Although ME has been known to exist since >30 years and was rather unconsciously utilized by urologist during the past decades, only recently this mechanism has begun to gain some glimpses of popularity in the endourologic community with the recent commercial introduction of a laser device overtly referring to it, that is, Moses™ technology (MT; Lumenis®).
To better clarify what the ME is and how it affects laser functioning, we aimed at performing a narrative review of the historical background of ME, from its origins and development up to its current endourologic applications.
Evidence Acquisition
An initial search was carried out using the Medline, PubMed, and Scopus databases. We largely selected publications from the past 30 years (January 1988–December 2018), but did not exclude commonly referenced and highly regarded older publications. Keywords included: Moses effect OR technology AND lithotripsy OR stone OR BPH OR prostate [Title/Abstract]. Abstracts were reviewed by the panel for relevance to the defined review question. If it was not clear from the abstract whether the article might contain relevant data, the full article was assessed. The references cited in all full-text articles were also assessed for additional relevant articles. Non-English articles were excluded from the analysis. With the consensus of the coauthors, the relevant studies were then selected and screened, and the data were extracted, analyzed, and summarized after an interactive peer review process of the panel.
The preferred reporting items for systematic reviews and meta-analysis flowchart were used to report the numbers of articles identified and included or excluded at each stage (Fig. 1). A narrative synthesis of the selected studies was, therefore, conducted, integrating with further theoretical notions available from selected book chapters referenced in included studies.
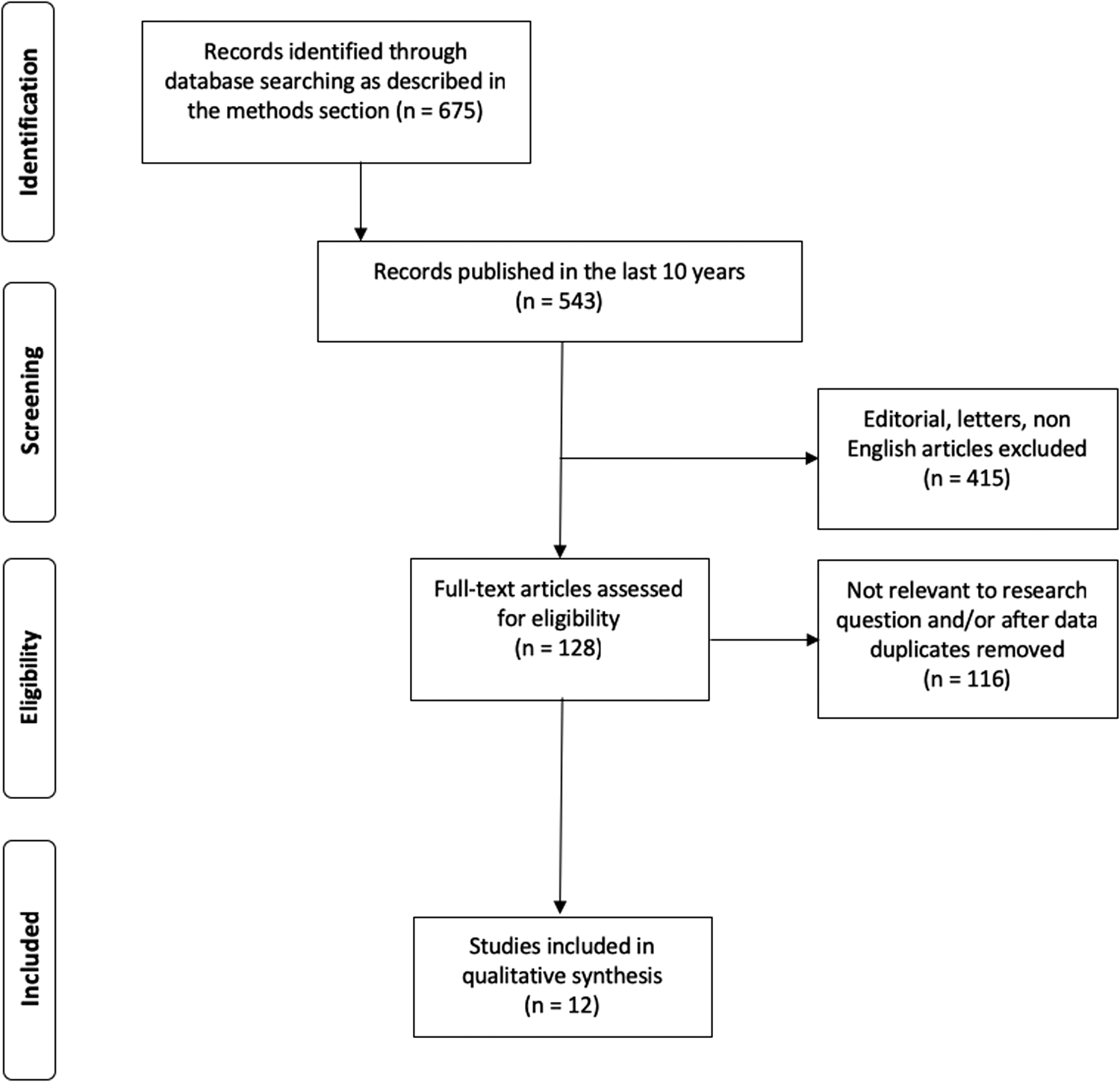
Preferred reporting items for systematic reviews and meta-analysis flow diagram showing the outcome of the initial and additional searches resulting in the full studies included in the review.
Evidence Synthesis
Brief history of laser
Although laser has been widely diffused in many areas of the medical world, urologic applications for lasers became available only relatively recently compared with nonurologic ones. The initial experiences were carried out with lasers using a synthetic ruby crystal as a gain medium and a flashlamp as an energy “pump.” 4 As the technology evolved, several and different gain media with different inherent mechanisms were developed to adapt to each setting requiring specific energy and wavelength parameters. 5 Both gas and dye lasers, among the first ones employed for medical purposes, have inherent limitations both when working in a liquid environment and when trying to achieve an effective lithotripsy. 5 –7 After these initial experiences, solid-state lasers (i.e., using a solid-state gain medium, such as crystals doped with ions, which can be excited to the desired energy levels) emerged as the leading characters in the field, especially in their Ho:YAG declination.
The origins
The first report overtly referring to the ME was a conference communication in 1986 3 (Fig. 2). Back then, the interest into lasers was prompted by their supposed application in intravascular ablation of atherosclerotic lesions. 8,9 Isner and colleagues, when describing 16-mm high-speed motion pictures recorded during ultraviolet and infrared focused beam laser irradiation of myocardial tissues, hypothesized the formation of “dynamic optical cavities,” that is, vapor tunnels serving as a pathway for the transmission of the laser pulse 10 (Fig. 3A). These observations were initially carried out into a blood-composed medium, and the early interpretation of these optical cavities was rather uncertain, or at least not translatable to the current urologic laser applications. What was clear was that these vapor tunnels enabled the transmission of laser energy over much longer distances in liquids than expected from the optical penetration depth. 11 It came quite straightforward that ME was named Moses after the Exodus prophet, when he parted the Red Sea and the Israelites walked on the exposed dry ground and crossed it safely. 12 Royston and colleagues 13 further quantified this effect, observing an unexpected increase in the transmission (up to 10%) of laser radiation in a 50/50 blood–saline, suggesting that the microbubble flow created a dynamic channel in the blood–saline through which the laser radiation was transmitted. Despite these promising early findings, only few reports later discussed the ME, 14 with rather slow spread in both clinical and research setting. Later advanced described how bubble formation, expansion, and collapse (Fig. 3D) may result in generation of acoustic transient, i.e. shock waves theoretically capable of interfering with and damaging nearby tissue. 10,11,15
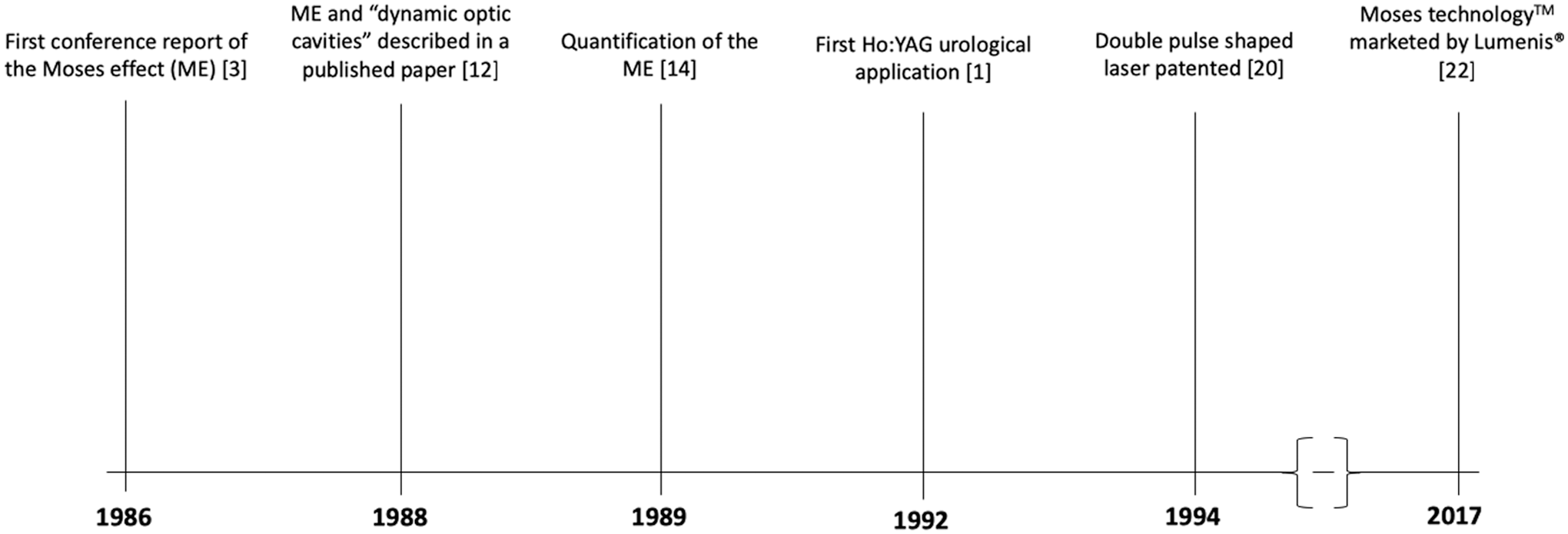
Historical timetable of ME appearance, description, and development. ME = Moses effect.

Slow-motion picture comparison of ME and Moses technology laser pulse.
Toward the application to urologic procedures
The interest in noncontact laser energy delivery met halfway with the concept of these laser-induced “vapor cavities.” The research group by van Leeuwen and colleagues 16,17 focused their attention in the early 1990s on holmium:yttrium-scandian-gallium-garnet (Ho:YSSG) laser for noncontact tissue ablation, better characterizing the ME in both blood and saline media in terms of pulse duration, tissue penetration, and characteristics of the vapor cavity.
When the focus of research moved toward Ho:YAG lasers, the need for better understanding and exploiting the ME became more impellent. The wavelength output of the Ho:YAG laser (∼2.1 μm) is highly absorbed in water, with a consistent decrease of the amount of energy delivered to the target. 5 As explained earlier, part of the energy absorbed by the water results in creation of vapor microbubbles; once these bubbles reach the target, the laser beam can pass through with very little attenuation since the density of the water molecules in the steam is considerably lower compared with the liquid phase. 18 The kinetics of bubble formation (100–200 μs) is in the order of the Ho:YAG pulse. 18 Moreover, the formation of the vapor bubble can be triggered by a very small amount of laser energy, and the speed at which the bubble forms is relatively independent from the duration or the energy of the pulse. 18
The actual characterization of the amount of energy needed to create the bubble made it clear 19 that the laser pulse could be effectively optimized to achieve the best delivery of energy to the desired target. More in detail, considering the initial experiments when the ME was noticed and described, it was estimated that up to a half of the emitted energy could be absorbed by the liquid medium before reaching the target, partly contributing to fluid vaporization and bubble formation 19 (Fig. 3B, C). By making this process more efficient, it would have been theoretically possible to dedicate the least possible amount of energy to bubble formation, with the intent of maximizing laser delivery. To achieve this, a new pulse delivery format was developed, in a way that the very first pulse would have had an energy level adequate to initiate the formation of the vapor bubble corresponding to only a small proportion of the energy level that could be generated by the laser. 19 This “initiation pulse,” followed then by a regular, high-energy pulse with an adequate time delay between the two pulses would be sufficient so that the vapor bubble will have had a chance to expand and displace a substantial portion of the liquid medium in the region between the delivery end of the fiber and the target. It was hypothesized that the time delay could be dependent upon the spacing between the fiber and the target (in the order of 100–200 μs) 19 (Fig. 3B, C). Since relatively little energy is used to create the bubble, it was reasonable to think that and most of the generated energy could reach its goal with little waste in water heating compared with conventional laser pulse. 19
This idea was explained and patented by Trost between 1993 and 1994. 19 Trost further estimated the amount of energy required for the first pulse, in the order of the amount of energy needed to raise the volume of liquid adjacent to the delivery end of the fiber to its boiling point, and proposed the following formula for its estimation 19 :
A × L × C × ΔT = minimum energy
where A stands for the cross-sectional area of the fiber, L is the absorption length of the radiation in the liquid medium, C is the specific heat of the liquid medium, and ΔT is the difference in temperature between the ambient temperature of the liquid medium and the boiling point temperature.
Further studies were dedicated to the finer understanding and codification of the physical mechanisms of laser properties in fluids, in relation to the dynamics of bubbles formation and laser transmission. 5,11,20
ME and MT
According to what described earlier, ME is a physical phenomenon taking place whenever a urologist activates a Ho:YAG in the operating theatre, irrespective of laser parameters, fiber dimension, and manufacturer (and given that the laser fiber is correctly working in a fluid environment). The inherent characteristics of ME were the rationale for developing MT (Lumenis). The purpose of this device is to modulate the laser pulse from a Ho:YAG energy source in two components, where the first one is used for separating the water between the laser tip and the target (e.g., the stone), whereas the second directly delivers the energy to it. 19,21 The delivery of energy through the water is thus optimized in a way that the first pulse component creates a vapor cavity through which the laser beam from the second pulse can travel without considerable energy loss.
MT became commercially available in 2017 for stone lithotripsy and benign prostatic obstruction (BPO) endoscopic surgical treatment. Two different working settings have been designed for Moses technology: a contact (Moses A) and a distance (Moses B) mode. Both Moses A and B are recommended for lithotripsy, the first one to be used at a 1 mm distance, the second at 2 mm. 21 Aside from MT, other available laser devices are equipped with pulse systems (e.g., the “Vapor Tunnel™“ by Quanta System® and the “Stabilization mode™“ by Olympus®) marketed as capable of exploiting the ME phenomenon, although published studies are currently lacking, and specific features are obtainable only from company-distributed marketing material.
Current clinical use and available postmarketing data
It is clear how the clinical demand for better lasers brought along a better understanding of their functioning principles. According to the manufacturer, MT improves energy transmission and, therefore, efficacy thanks to its split pulse shape. Manufacturer (and yet not fully published at the time of this article writing) data account for a 20% reduction in procedure time, 60% reduction in retropulsion, and 25% reduction in fragmentation time as far as lithotripsy. 22 These findings are based on industry-sponsored studies, which, to date, were mostly presented at international meetings and not published in peer-reviewed journals yet. 21,23,24
The same should be outlined for MT prostate laser enucleation result, promising but still not confirmed in an independent postmarketing setting. 24,25 Considering available laboratory studies, MT was found to produce dust more structurally different from the original crystalline structure (i.e., conversion of calcium oxalate dihydrate toward calcium oxalate monohydrate, changes in carbapatite spectra toward an amorphous phase, changes of magnesium ammonium phosphate toward a differing amorphous, and crystalline phase and the appearance of hydroxyapatite on brushite fragments) compared with conventional laser dusting. 26 Although not confirmed in a clinical setting, MT was also capable of achieving in vitro greater ablation of soft stone (i.e., Begostones mimicking uric acid stones) both in contact and at 1 mm distance compared with traditional Ho:YAG settings, whereas pulse type did not have a significant impact on ablation for distances >1 mm and for hard stones at any distance. 27 Although subsequently confirmed in a laboratory setting, 28 the clinical efficacy of these findings remains to be confirmed.
Only one report analyzed the economic impact of introducing MT; more precisely, a cost analysis questioned the cost-effectiveness of MT in stones >10 mm. 29
Conclusions
ME was described for the first time >30 years ago. It takes place during traditional Ho:YAG laser functioning in a liquid fluid, and, therefore, during all endourologic laser applications. In 2017, a Ho:YAG laser-emitting device equipped with MT was made clinically available for both laser lithotripsy and endoscopic prostate enucleation. If, on the one hand, ME is accurately described and characterized, on the other, a substantial lack of published comparative clinical studies in terms of safety and effectiveness does not allow to draw any conclusion on the clinical advantages of using MT over standard Ho:YAG laser, despite its underlying rationale and initial laboratory results.
Footnotes
Author Disclosure Statement
Prof. Olivier Traxer is a consultant for Coloplast, Rocamed, Olympus, EMS, Boston Scientific and IPG.